
Abstract
Background. This study examined the sociodemographic as well as other determinants and outcome of community-acquired late-onset neonatal sepsis (LONS) in rural Bangladesh at Matlab. Methods. In this retrospective chart review, we used an unmatched case-control design (1:2 ratio) to evaluate the factors associated with LONS and their outcomes among babies admitted to the neonatal ward of Matlab Hospital of icddr,b, from January 2012 to December 2014. Neonates presenting with any of the clinical signs of serious bacterial infection during 3 to 28 days of life constituted the cases (LONS), and those without LONS constituted the controls. All the data were retrieved from the electronic databases of Matlab Hospital and Matlab Health and Demographic Surveillance System. Results. Among 1482 admitted neonates, 202 were cases and 404 were randomly selected controls. In babies with LONS, case fatality rate (1% vs 0%, P = .037), duration of inpatient stay (4 days vs 2 days, P < .001), and referral to higher center (9% vs 5%, P = .020) were higher. In an adjusted model, undernutrition (weight for length Z score < −2; odds ratio [OR] = 1.8, 95% confidence interval [CI] = 1.2-2.94), admission in winter season (OR = 1.62, 95% CI = 1.09-2.41), mother’s schooling <10 years (OR = 1.76, 95% CI = 1.09-2.85), primiparity (OR = 1.55, 95% CI = 1.05-2.29), home delivery (OR = 1.87, 95% CI = 1.07-3.26), and household food insecurity (OR = 2.78, 95% CI = 1.31-5.88) were found to be independently associated with LONS. Conclusion. LONS posed considerable socioeconomic burden to the rural community. Further studies are required to consolidate our findings.
Keywords
Introduction
Clinical sepsis in neonates denotes a spectrum of diseases such as septicemia, pneumonia, and meningitis featuring clinical signs of serious infection in the presence or absence of bacteremia in the first 28 days of life.1-3 On the list of causes of neonatal death, severe infection sits within the top 3,4-8 which is a major concern for low- and middle-income countries in particular. In resource-poor countries including Bangladesh, sepsis alone contributes to about 7% of the child deaths occurring in the first 28 days of their lives. 9
Neonatal sepsis can be classified into early-onset sepsis (EONS) and late-onset sepsis (LONS) depending on the time of onset.10-12 EONS occurs mostly by infections acquired from mother prior to or during childbirth, 13 while postnatal environment (community or hospital) plays a direct role in the development of LONS.11,14-18 Globally, incidence of EONS has reduced over decades, whereas the picture is quite opposite for LONS,19-21 and Bangladesh is not an exception. 22
Evidence suggests that in Matlab, a rural area of Bangladesh, LONS is the single largest contributor to all the deaths occurring in the late neonatal period. 23 Lots of efforts have been made to identify the factors contributing to LONS.24-26 The majority of these information are based on studies related to neonatal intensive care unit, especially focusing nosocomial infections.18,27 A prospective study in Switzerland have found that community-acquired LONS contributes to nearly one third of the total burden of LONS. 28 However, most studies on the community-acquired LONS, including the lone study in Bangladesh, have focused on pathogen identification,16,28-31 lacking valid information on sociodemographic influence on community-acquired sepsis, especially LONS and its outcome. 29
In this context, the aim of this study was to identify the sociodemographic as well as other determinants and outcome of community-acquired LONS in rural Bangladesh at Matlab.
Methods
Study Setting
Our study population resided in Matlab, a rural subdistrict of the Ganges-Meghna Delta, lying 55 km southeast of the capital city, where the level of poverty was 26%, 32 rate of illiteracy was 26.2%, 96% households use tube well water for drinking, and 93% households use solid fuel for cooking. 33
In Matlab, icddr,b has been maintaining an internationally recognized and unique Health and Demographic Surveillance System (HDSS) since 1966 involving 142 villages, comprising a population of 230 000 people. The HDSS area is divided into 2 parts, an icddr,b service area and a comparison (government service) area, each covering a population of about 110 000. 34 Matlab Hospital is a primary health facility in Matlab, which offers free-of-cost clinical care to all diarrheal patients, and maternity and child health care to women of reproductive age and children younger than 5 years coming from half of the HDSS area (icddr,b service area).
Study Design, Population, and Data Source
This was a retrospective chart review. For this chart analysis, we used an unmatched case-control design and evaluated the factors associated with LONS in neonates and their outcome between the groups. Data on clinical features and outcome of patients, admitted to the neonatal ward of Matlab Hospital of icddr,b from January 2012 to December 2014, were extracted from Matlab SHEBA, an online database of Matlab Hospital. Neonates with LONS constituted the cases, and those without LONS constituted the controls. Controls were randomly selected from the children without LONS using Stata/PC (version 14.1; StataCorp, College Station, TX) from the personal computerized data source of this study. A 1:2 unmatched case-control ratio was used to increase the statistical power of our analyses. Sociodemographic, maternal, and childbirth-related information were retrieved from the electronic database of HDSS. Case report forms were developed, pretested, and finalized for acquisition of relevant data.
Late-Onset Neonatal Sepsis
LONS was defined as the appearance of any of the clinical signs enlisted in Box 1 between >72 hours (3 days) of birth and first 28 days of life.10,35 All of these signs indicate serious bacterial infection (sepsis) in neonates. 35
Signs of Serious Bacterial Infection (Sepsis) in Neonates a .

Source: Pocket Book of Hospital Care for Children. Second edition, 2013. 35
In our present study, infants with LONS were classified as having community-acquired LONS if neonates who are resident of the region presented with the symptoms of interest between the age of 3 and 28 days, with no history of discharge from any hospital within past 48 hours. 16
Patient Management
Both the cases and control children received standard management including antibiotics if necessary following the World Health Organization (WHO) recommended treatment guideline of neonatal sepsis. 35
Determinants of LONS
We presumed several nutritional, maternal, childbirth-related, sociodemographic, and environmental characteristics as potential risk factors for LONS. Characteristics considered and analyzed included age, sex, nutritional status, breastfeeding practice, season of hospital admission, mother’s age, education and parity, place of delivery, mode of delivery, type of birth attendant, socioeconomic status (wealth quintile), family size, household food security, possession of livestock, type of fuel used in cooking, drinking safe water, and use of sanitary latrine. The climate in Bangladesh is characterized by a hot summer from March to May, a rainy monsoon season from June through October, and a cool, dry winter season from November to February. 36 Wealth quintile was computed by HDSS as asset score in a 1 to 5 scale, where 1 indicates the lowest. It served as an indicator of household-level wealth consistent with expenditure and income measures. The index was constructed using household asset data via principal component analysis. 33 Household food security was defined by HDSS as the availability of food for all family members, 3 times every day in the previous year. 33 Wood, wood dust, paddy husk, leaves, or straw use with/without kerosene were categorized as solid fuel, and gas and electricity were classified as clean fuel.
Statistical Analysis
All data were first extracted in Microsoft Excel, coded, cleaned, and entered into Stata/PC (version 14.1; StataCorp) for further statistical analyses. Weight for length Z scores was calculated by the WHO Anthro (version 3.2.2; Department of Nutrition, WHO, Geneva, Switzerland). Differences in proportion were compared by the χ2 test or Fisher’s exact test as appropriate. Student’s t test was used to compare the means of normally distributed data, and Mann-Whitney test was used for comparison of data that were not normally distributed. P < .05 was considered statistically significant. Strength of association in determining differences in proportion was determined by calculating odds ratio (OR) and their 95% confidence intervals (CIs). In identifying risk factors for LONS, variables were initially analyzed in a univariate model (Table 2), and then factors independently associated with LONS were identified using multiple logistic regression analysis after controlling for the covariates (Table 4). For logistic regression model building, independent variables were selected purposefully based on the method described by Hosmer et al. 37 Only the significant variables were retained in the final model.
Ethics and Informed Consent Statement
This study was solely a chart review and did not involve any interviews with patients or their care givers. Data for this study were retrieved from the case records of Matlab Hospital. Data were made anonymous and de-identified prior to analysis. Authors had no access to patient identifying information. Waiver of an ethical approval for this study was taken from the institutional review board (Ethical Review Committee) of icddr,b.
Results
A total of 1482 neonates were admitted during the study period, and among them, 202 were found to be cases and 404 were randomly selected controls (Figure 1).

Flow chart of the selection of study participants and analytic sample.
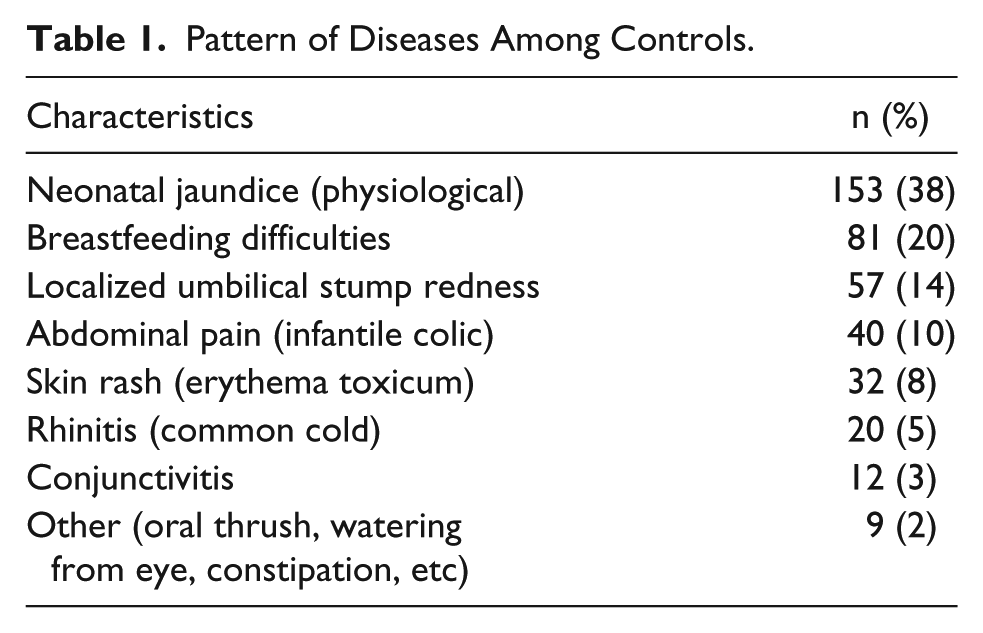
Cases have been defined in the Methods section, and common diagnosis of controls are enlisted in Table 1.
Pattern of Diseases Among Controls.
Median age of the neonates among the cases was 13 days and that of the controls was 10 days (P = .001; Table 2). In bivariate analyses, the cases more often had undernutrition (weight for length Z score < −2), admission in winter season, mother’s schooling <10 years, home delivery, delivery conducted by traditional birth attendants, vaginal delivery, larger family size (>4 members), household food insecurity, possession of livestock, and family’s practice of using solid fuel in cooking compared with the controls (Table 2).
Characteristics of Neonates With (Cases) or Without (Controls) LONS.

Abbreviations: LONS, late-onset neonatal sepsis; OR, odds ratio; CI, confidence interval; IQR, interquartile range; WLZ, weight for length Z score.
Statistically significant at 5% level.
The cases more often had longer hospital stay, required referral to higher center, and experienced higher case-fatality rates compared to the controls (Table 3).
Outcome of Neonates With (Cases) or Without (Controls) LONS.
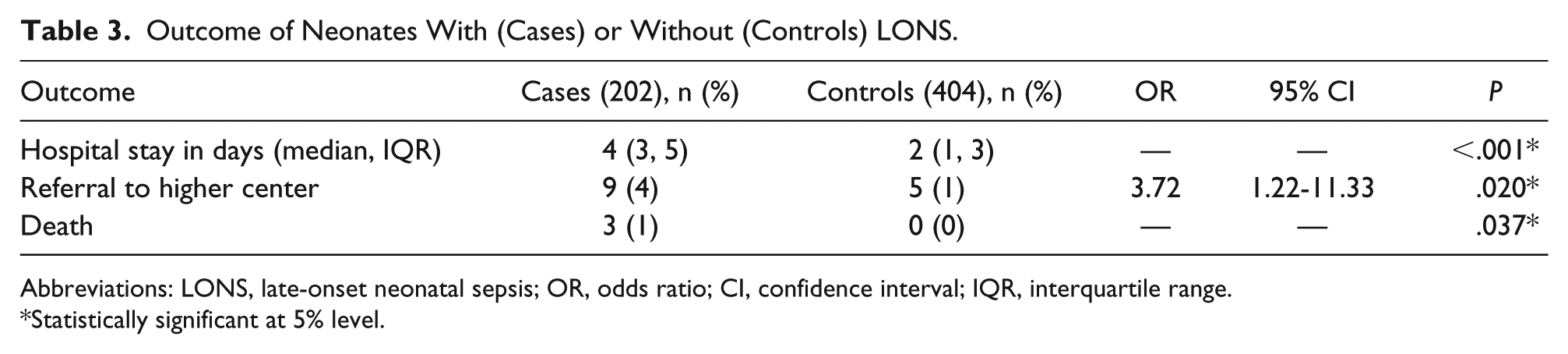
Abbreviations: LONS, late-onset neonatal sepsis; OR, odds ratio; CI, confidence interval; IQR, interquartile range.
Statistically significant at 5% level.
In an adjusted logistic regression model, undernutrition, admission in winter season, mother’s schooling <10 years, primiparity (a woman who has had one pregnancy that resulted in a fetus that attained a weight of 500 g or a gestational age of 20 weeks, regardless of whether the infant was living at birth or whether it was a single or multiple birth; also written para I or I-para), 38 home delivery, and household food insecurity were found to be independently associated with LONS (Table 4).
Results of Multiple Logistic Regression to Explore the Independent Predictors of LONS in Neonates.

Abbreviations: LONS, late-onset neonatal sepsis; OR, odds ratio; CI, confidence interval; WLZ, weight for length Z score.
Adjusted OR from multivariable model that includes child’s age in days, nutritional status, season of admission, maternal education and parity, whether the child had home delivery, and household food insecurity.
Discussion
To our knowledge, this is the first study that shed light on the factors, especially sociodemographic factors, contributing to the development of community-acquired LONS in rural Bangladesh. Undernutrition, winter season, mother’s schooling, primiparity, home delivery, and household food insecurity were observed to be the independent determinants of community-acquired LONS.
The observation of independent association of LONS with undernutrition is understandable. Underdeveloped immune system and skin barrier of undernourished neonates especially of those who born with low birth weight might make them vulnerable to environmental acquired infections. 29 However, we did not have data on birth weights of the participants of this study.
In this study, seasonality (winter season) was found to influence the development of LONS. In an Indian study, Bang et al found that umbilical infections, bacterial skin infections, conjunctivitis, and upper respiratory symptoms of neonates were increased in the winter. 39 Becker et al and Burkart et al also observed that neonatal death due to respiratory diseases peaked in the winter in rural areas.40,41 In the cool season, inadequate thermal protections along with increased congestion of people inside house, indoor air pollution from fire, decreased bathing, and washing of clothes are common in low socioeconomic condition and in rural areas like Matlab. 39 Although we do not have all these data, we can speculate our patient population often had an exposure to these risks and might have an impact on our observation.
Our finding that the offspring of less educated mothers were in higher risk of developing LONS was in line with the observation of a Brazilian study by Victoria et al where they found that infants of mothers with less or no education were prone to develop sepsis. 42 Gebremedhin et al also had somewhat similar findings. 43 Lack of appropriate maternal care, which is related to maternal illiteracy, might be responsible for the babies’ acquiring serious infections in the late neonatal period. 42
Primiparity was found to be associated with EONS in a Brazilian study by Vaciloto et al, 44 but no study directly explored the relationship between primiparity and LONS. Schrag et al concluded that some special characteristics of primiparous women (age <20 years, prolonged labor, prolonged rupture of membranes, and low infant birth weight) made their neonates vulnerable to adverse outcomes like sepsis, 45 which might explain the relation found in the current study between LONS and primiparity.
In this study, home delivery was one of the important determinants of community-acquired LONS. We can speculate that contaminated floor and unhygienic practice in the delivery room, unsterile cord care, and scarcity of skilled birth attendants might contribute to the development of sepsis in home deliveries as observed in previous studies.29,39
Our observation of association of the babies from food-insecure households with LONS is understandable. Household food insecurity prevailing in poor socioeconomic conditions along with lack of maternal education may lead to maternal malnutrition and consequently may result in low birth weight infants. 46 These babies may again face that food insecurity and become malnourished and susceptible to LONS.
Among the LONS cases, the duration of hospital stay was higher compared with the control group, which imposed a significant financial burden to the rural community. Besides, adverse outcomes (referral to higher center, death) were also higher among the cases in comparison to the controls. These findings were consistent with the observations of Stoll et al in a study in the United States. 25
In this study, median age of the babies with LONS was 13 days, which was aligned with the findings of Vergnano et al, 11 Boghossian et al, 14 and Hammoud et al, 17 who found that the peak incidence of LONS occurred between the 10th and the 22nd day. No difference in sex distribution was observed between the cases and the controls. Ng et al had a similar finding in a study of LONS. 47
Although this study is important due to its unique nature for being the first study done in low-resource setting exploring the influence of sociodemographic and other factors on the development of community-acquired LONS, its findings should be interpreted in light of several limitations. The first limitation was the retrospective nature of our study, which confined our sample size, and did not allow for the systematic collection of data with stringent quality control. Since the study was done on admitted neonates, the results might not be generalized to all neonates in the catchment community. Although controls were taken from admitted neonates who had minor illnesses as evident by the absence of deaths, they merely represented healthy community controls. Moreover, as we did not have access to antenatal data, it was not possible for us to adjust certain maternal characteristics (ie, antenatal checkup, maternal disease, etc). The lack of laboratory evidence and the subjectivity in the assessment of the clinical signs of sepsis in neonates was another limitation.
To conclude, in our study, LONS posed a considerable economic and social burden to the families and the community considering that neonates with LONS had a longer hospital stay, higher number of referrals, and most importantly, higher case fatality compared with those without LONS. Our study revealed that undernutrition, winter season, mother’s schooling <10 years, primiparity, home delivery, and household food insecurity were the independent determinants of community-acquired LONS. Further studies with larger sample size are required to consolidate our observation on the relationship between community-driven factors and LONS especially in resource-limited settings.
Footnotes
Acknowledgements
The authors would like to express their sincere thanks to all the staff members of the “Neonatal Ward” of Matlab Hospital including physicians, nurses, clinical attendants, feeding team, and cleaners for their invaluable support in patient care. The authors also offer their sincere gratitude to Dr Syed Imran Ahmed for his moral and intellectual support.
Author Contributions
KNS, SMTH, MAK, TA, and MJC conceived and designed the study; KNS, SMTH, and MJC collected, merged, and cleaned the data; SMTH, KNS, and MJC analyzed the data; MAK and TA gave technical support and conceptual advice; KNS, SMTH, MAK, and TA wrote the manuscript; MJC finally approved the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by core donors that provide unrestricted support to icddr,b for its operations and research. Current donors providing unrestricted support include Governments of Australia, Bangladesh, Canada, Sweden, and the United Kingdom. The authors gratefully acknowledge these donors for their support and commitment to icddr,b’s research efforts.