
Abstract
Objectives:
ICD-10-based approaches often provide the basis for retrospective estimation of potential palliative care need. Applying the ICD-10-based Murtagh et al. classification from 2014 (Murtagh classification), developed using mortality data, to administrative claims data leads to inconsistencies in estimating palliative care need. The aim of the study was to refine the classification for palliative care need estimation in deceased individuals with cancer and non-cancer diagnosis.
Methods:
A retrospective population-based study comparing Murtagh classification to a new ICD-10-based classification (revised by expert opinion) was conducted using outpatient and inpatient claims data, including billing codes for palliative care. Palliative care need was estimated for diagnoses groups and was contrasted with palliative care utilization rates in the last year of life. Our dataset included records of 417,405 individuals who deceased in 2016–2019.
Results:
Out of individuals deceased in 2019 (n = 117,436), 81.4% had at least one diagnosis from the new classification, while 97.0% had at least one diagnosis from the Murtagh classification. Classification revision thus identified fewer individuals as potentially in need of palliative care. Among individuals with cancer, 70.7% (vs. 55.7% via Murtagh classification) received palliative care. In non-cancer subgroups, the utilization rate was considerably lower, with a maximum of 36.7% (vs. 33.7% via Murtagh classification) in 2019. Similar results were observed for the other years.
Conclusion:
Compared to the ICD10-based Murtagh classification, the revised ICD-10-based classification enables more realistic estimations if the cause of death is unavailable and reveals higher rates of palliative care coverage and differences especially in cancer versus non-cancer diseases. German Clinical Trials Register (DRKS00024133).
Keywords
Introduction
Palliative care need estimations regularly serve as tool to policymakers for capacity planning.
Palliative care that is known for improving quality of life and avoiding burdening interventions and transitions at the end of life with a potential to also save on health care costs targets individuals who experience functional decline in the end of life.1–4 In aging societies, the percentage of individuals who would benefit from palliative care is expected to rise further.5–7 In addition to cancer, individuals with chronic conditions like chronic obstructive pulmonary disease, dementia, heart failure, and neurodegenerative diseases—which made up to 73.4% of all deaths worldwide in 2017—may also benefit from palliative care.8–15
Current estimations of palliative care need worldwide range from 38% to 90% of the yearly deceased.15–25 In Germany, a death-cause-data-based analysis revealed palliative care need for 78.0%. 21
Approaches for retrospective identification of individuals who may have benefited from palliative care vary from expert opinion to machine learning models using various sources of data (mostly hospital and insurance claims, death certificates).19,20,26–28 Applying the appropriate method for analyzing large datasets with respect to palliative care need seems to be crucial for enhancing the reliability of results.
Often an ICD-10-based approach based on Murtagh et al. 19 classification (Murtagh classification) provides the basis for the retrospective estimation of palliative care need and its projection into the future.22–24,29 The Murtagh classification was derived from expert consensus on diagnoses documented in hospital records of the last year of life and underlying causes of death.30,31 The resulting classification represents a compilation of a whole chapters of ICD-10-classification. This classification is now commonly used for retrospective estimation of palliative care need based on health insurance claims data.32,33 However, although claims data certainly provide a reliable basis for an analysis of palliative care utilization, it, frequently, like in Germany, lacks information on the cause of death.
Although the Murtagh classification appears suitable for analyzing mortality data, it does not seem appropriate due to its lack of specificity when applied to administrative diagnoses documented within the last year of life. This lack of specificity becomes evident as the Murtagh classification contains many non-specific diagnoses and non-life-threatening conditions, such as arterial hypertension, flu, kidney cysts, and upper respiratory tract infections—diagnoses that do not constitute criteria recommended for admitting a patient into palliative care.34–36 Although diagnoses alone may not be sufficient to fully determine the need for palliative care, ICD-10-based methods using diagnoses data might help to estimate the potential need for palliative care in deceased individuals and thus to identify potential gaps in palliative care coverage.
Moreover, it is still not common practice to exclude concomitant cancer diagnoses in deceased with other non-cancer (NC) diagnosis, whose needs are still known not to be met.37,38 Data distortion can be avoided by a hierarchical structure of diagnoses, which is common for death certificates (main and antecedent death causes), allowing the extraction of NC-related deaths. In claims data, however, ICD-10 diagnoses are documented in a non-hierarchical way. That makes it difficult to differentiate between cancer and NC groups. As a result, it can easily lead to an overestimation of palliative care need and accordingly to an underestimation of palliative care utilization, especially in the population of mostly elderly, multimorbid deceased individuals.
In the current study, we addressed this research gap by distinguishing between deceased individuals with cancer and NC diagnoses when determining the potential need for palliative care and analyzing the utilization rate in these disease groups. The aim of our study was to develop a refined diagnosis-based internationally applicable classification that enables the use of claims data—not containing cause of death information—for analyzing the palliative care need and utilization overall and in specific diagnosis groups of interest.
Methods
Study design and setting
A retrospective population-based analysis was conducted using outpatient and inpatient claims data covering the last year of life for individuals deceased in the years 2016–2019. There were 417,405 adult (BARMER) health insurance beneficiaries continuously insured at least throughout the last year of life. With more than 8 million insured persons, representing approximately 10% of the total German population, BARMER is a large statutory health insurance. 39
Diagnoses selection
In the process of identifying diagnoses that could define palliative care need, experts from the Institute of General Practice and Family Medicine and the Department of Palliative Care of Jena University Hospital (see eSupplement) followed a methodology similar to that used in the development of clinical assessment tools.34,40,41 Specifically, the following question was posed: “Who would have had potentially benefited from palliative care?”—considering a dataset containing only information on ICD-10 diagnoses of deceased individuals.
As listed in the eSupplement, ICD-10 codes with severity grading were selected (e.g., New York Heart Association III/IV heart failure, coronary heart disease, intracerebral hemorrhage or ischemia, renal function impairment, chronic obstructive pulmonary disease (COPD), liver cirrhosis and its possible complications, Parkinson’s disease, and multiple sclerosis). Dementia codes selected by Murtagh et al. 19 were expanded to include further forms of dementia; the unspecific code of senility was excluded. In addition, new NC chapters were created, specifically targeting “acute life-threatening conditions” and “consciousness disorders,” such as severe respiratory distress or locked-in syndrome, which may also entail palliative care need and utilization. Cancer diagnoses in Murtagh classification were limited to advanced cancer (e.g., metastasis (except lymph node metastasis), cancer overlapping body sites, and blood cancer “without mention of complete remission”), whereas cancer diagnoses with a favorable prognosis due to pathophysiological factors or available treatment options were excluded. This procedure is consistent with clinical assessments suggesting palliative care for individuals with poor prognosis of primary tumor or to those with progressive metastatic cancer.42,43
Case ascertainment
Deceased individuals were considered to have been in palliative care need if at least one of the ICD-10 codes listed in the eSupplement was documented in their last year of life in inpatient or outpatient data. Bias due to false-positive diagnoses was reduced by including only valid diagnoses, internally marked as “verified” in the outpatient data or as “main discharge diagnosis” or “secondary diagnosis” in the inpatient data.
To avoid data distortion due to possibly concurrent cancer, C00-C97 diagnosis or an advanced cancer diagnosis (see eSupplement) was excluded in presenting NC groups. Among NC diagnoses, no ranking between selected diseases of high severity was conducted in order to underline the equality of these diseases in palliative care. This approach deviates from Murtagh et al. 19 and other research groups who presented deceased with NC diagnosis without excluding coexisting cancer diagnosis.32,33
The rate of palliative care utilization was determined following the approach reported by Ditscheid et al. 44 based on the documentation of at least one corresponding service for billing purposes in the last year of life.
Reporting and statistical analysis
Results were reported based on the recommendations of the STROBE, STROSA, RECORD statements, and GPS guidelines.45–48 Data processing was done using SAS Enterprise Guide Version 8.3 (SAS 9.4, SAS Institute Inc., Cary, NC, USA), and descriptive statistical analysis and graphics were performed using R, Version 4.1.2.
We present descriptive statistics (i.e., rates and absolute frequencies) regarding palliative care need and palliative care utilization, both overall and for each cancer and NC groups (cardiovascular, cerebrovascular, neurological, kidney, liver diseases, and dementia) without adjustment for other comorbidities. Palliative care need rates (percentage of patients with need divided by the number of all deceased) were calculated per year in order to consider annual changes in disease prevalence, ICD-10 codes and, subsequently, diagnosis encoding practices. Specificity analyses were conducted by determining palliative care need-based utilization rates in each group. Rates were calculated per year in order to consider annual changes in palliative care provision in Germany elucidated by Ditscheid et al. 44 Sensitivity analyses were conducted by determining the utilization rate of palliative care in the group of deceased individuals for whom the respective classification suggested no palliative care need.
To correct for differences in the distribution of age and gender between BARMER beneficiaries and the general population in the federal states of Germany and to allow the extrapolation of results, all analyses were standardized by age and gender. The weights we applied for this purpose were determined in previous studies (for details, see Ditscheid et al. 44 ).
Results
In order to support more realistic retrospective population-level and diagnoses group-level measurements of palliative care need and utilization, we used routinely collected administrative data of deceased. We revised the widely used but unspecific ICD-10-based Murtagh classification. Palliative care experts shortened this classification from over 1300 four-digit diagnoses to about 300.
Palliative care need
In 2019, 95,597 (81.4%, out of N = 417,405) deceased individuals had at least one of the ICD-10 diagnoses specified in the new classification, while 113,931 (97.0%) had one of the diagnoses of the Murtagh classification (Figures 1 and 2, and Table 1). Focusing only on NC diagnoses, the frequencies turned out to be 66,093 (56.3%) (for the new classification) versus 64,777 (55.2%) for the Murtagh classification, respectively. An increase of palliative care need rates over the years was observed in both classifications (Figure 1).
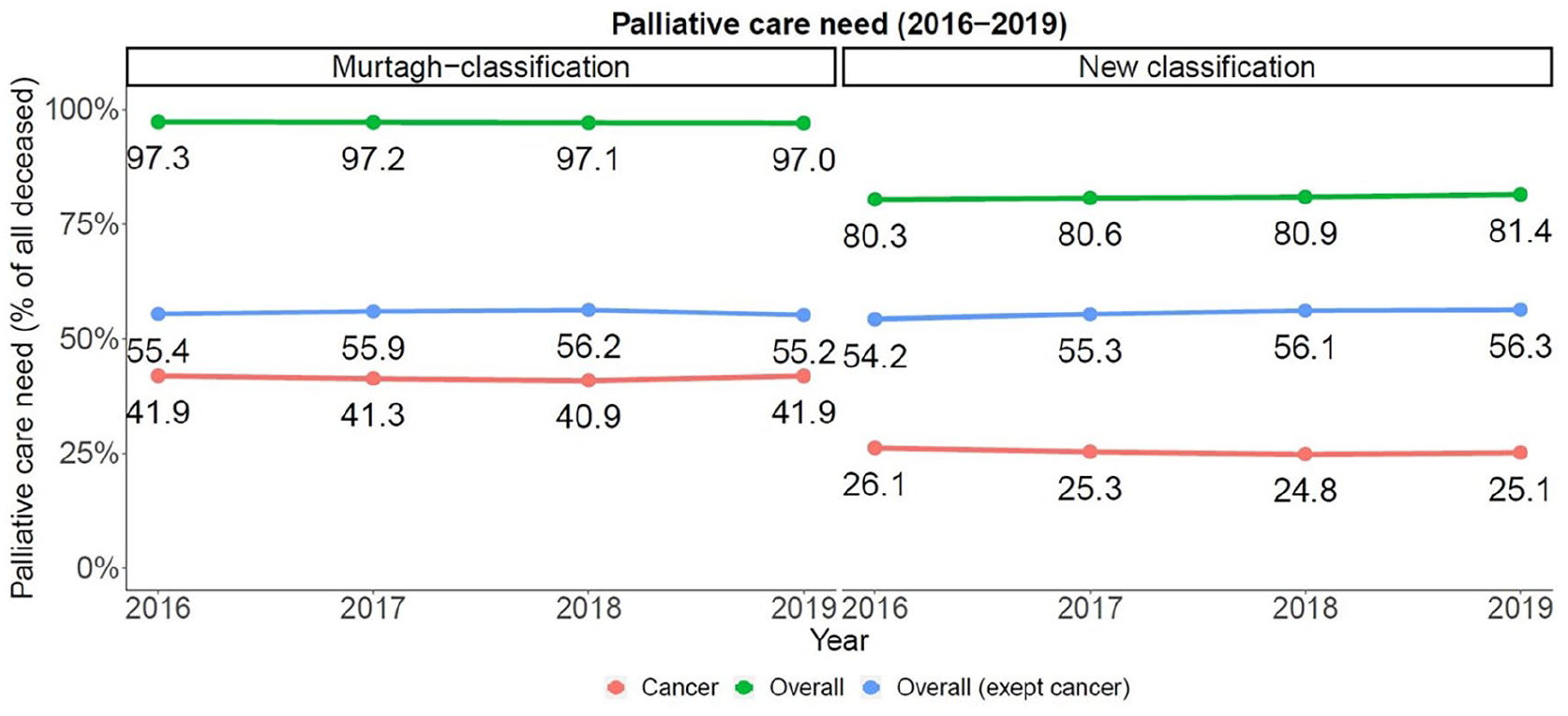

Palliative care NEED 2019 among all deceased within each group if analyzed according to Murtagh et al. 19 (blue) versus new classification (green) in percentage of all deceased in 2019 (n = 117,436), cancer excluded in non-cancer groups.
Palliative care need (n, %) in deceased and palliative care utilization (n, %) in deceased with palliative care need (N = n (deceased within diagnosis group)) based on the Murtagh classification and the new classification.

N(2016) = 97,260; N(2017) = 99,585; N(2018) = 103,124; N(2019) = 117,436.
Palliative care utilization
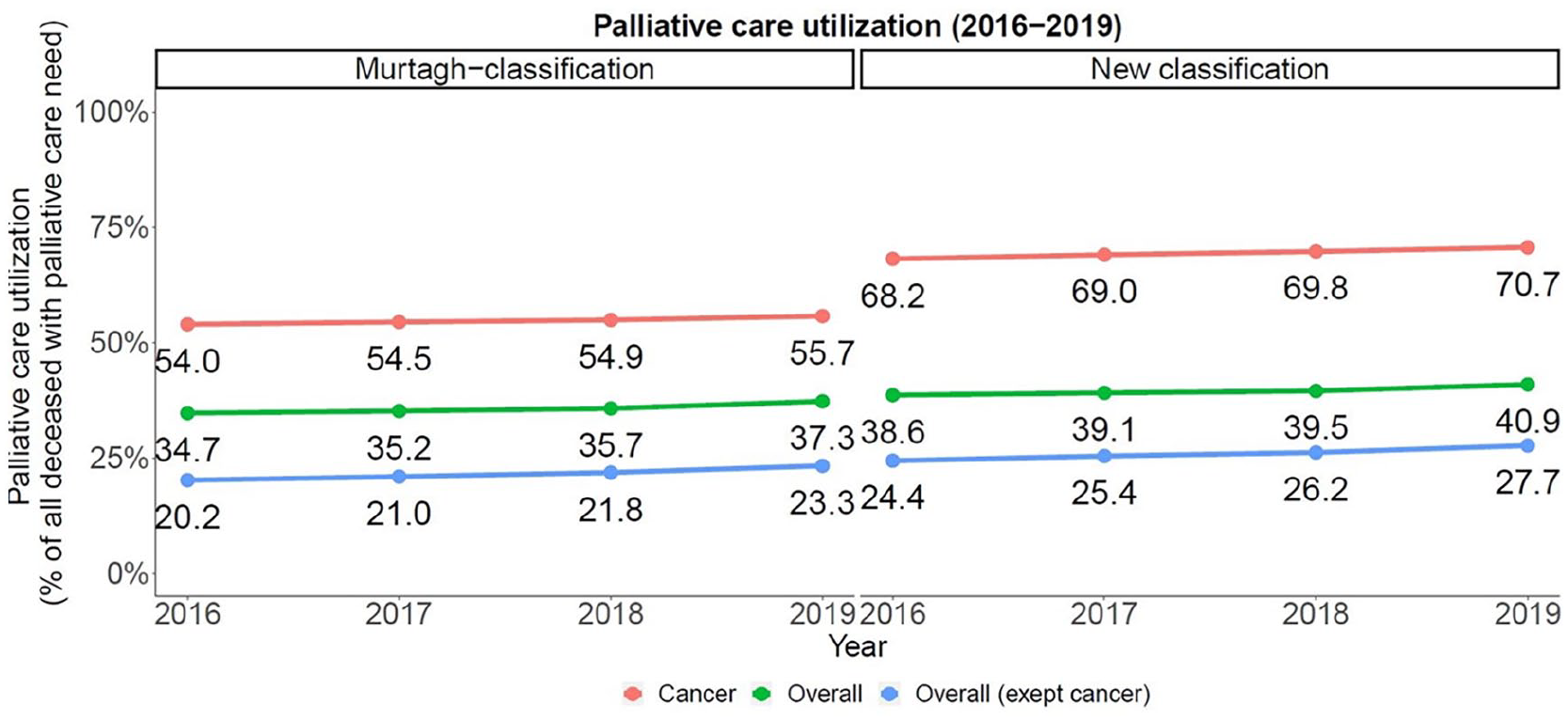
In 2019, 39,138 (40.9%) of all deceased with potential palliative care need due to the new classification versus 42,487 (37.3%) due to the Murtagh classification received palliative care before death (Figures 3 and 4, and Table 1). An increase of palliative care utilization over the years 2016–2019 could be found in both classifications in all cancer und NC groups. According to new classification, 18,292 (19.1%) of the descendants with NC diagnosis received palliative care utilization versus 15,091 (13.2%) according to the Murtagh classification.
Comparing classifications’ sensitivity for all deceased over the years, max. 3417 (15.6%, 2019) of deceased without palliative care need actually received palliative care (“false-negative”) versus max. 68 (1.9%, 2019) if the Murtagh classification was applied.
Extrapolation to the population of deceased individuals in Germany
According to the German mortality statistics, there were 910,920 deceased in 2016 and 939,520 in 2019; more than half a million deceased with NC-diagnosis. 49 For 2019, extrapolation of standardized data from our study would result in about 767,000 (new classification) and 911,000 (Murtagh classification) deceased with potential palliative care need. Despite this lower number of individuals with palliative care need, and steadily rising palliative care utilization, the provision of palliative care remains inadequate: applying the new classification, about 236,000 in 2019 had cancer of which roughly 70,000 did not receive palliative care; and about 529,000 had an NC diagnosis of which roughly 382,000 did not receive palliative care. 44 Altogether, the number of deceased with palliative care need having received palliative care increased by 31,300 from 2016 to 2019, by about 4800 in cancer and 26,500 in NC group (new classification).
Discussion
Summary of main findings
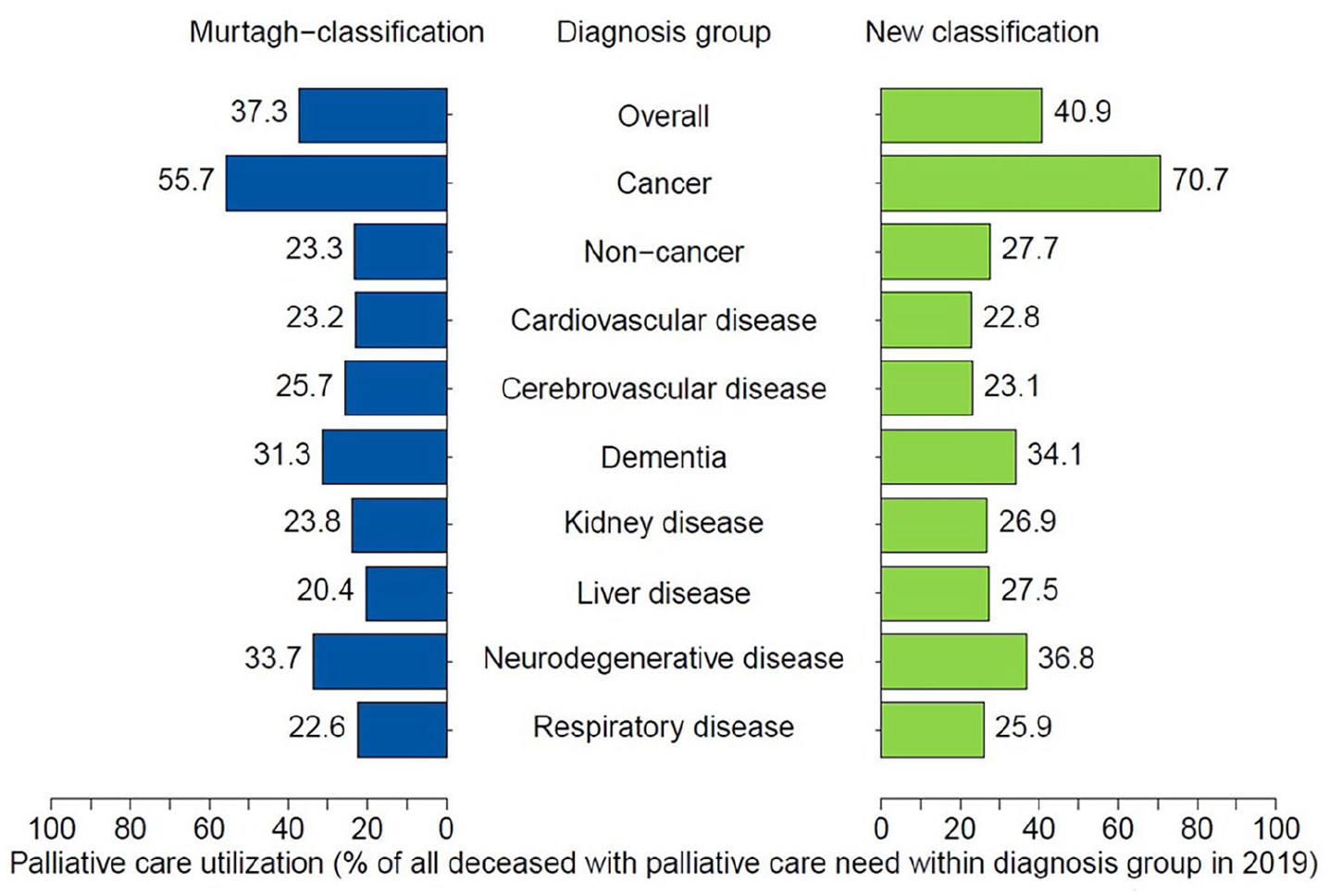
The choice of classification changed the results of palliative care need and utilization analysis substantially. Overall in 2019, the number of deceased with potential palliative care need identified with the new classification was 15.6%-points smaller than the number identified based on the Murtagh classification. However, in NC groups, palliative care need was almost equal comparing both classifications. Classification revision also led to fewer individuals identified as potentially in need of palliative care when focusing on disease groups, with a drop of 31.2%-points (respiratory diseases), 25.9%-points (kidney), 21.4%-points (cardiovascular disease), 18.3%-points (cerebrovascular disease), 16.8%-points (cancer), and 9.4%-points (liver) in 2019. The estimation of individuals in need in the dementia and neurodegenerative groups changed only marginally.
In all revised groups, palliative care utilization in 2019 increased by 3.7%-points than if evaluated using Murtagh classification. 19 Need was better covered by utilization in most groups due to specificity of diagnosis: 15.0%-points (cancer), 7.1%-points (liver), 3.3%-points (respiratory diseases), 3.1%-points (kidney), 3.0%-points (neurodegenerative disease), and 2.8%-points (dementia) more. A remarkable finding is the utilization rate in the newly defined group of deceased individuals with consciousness disorders. Amounting to 21.6% (new classification), it is higher than in most other groups (except for cancer, dementia, and neurodegenerative disease). While 70.7% of all deceased with advanced cancer received palliative care in 2019, the maximum among the NC groups reached only 33.3% (in deceased with neurodegenerative diagnosis in 2019, new classification).
Comparison with previous research: Estimation of palliative care need
If analyzed according to Murtagh et al., 19 97% of all deceased would have been identified as people in need of palliative care. This finding is consistent with other regional German claims data studies conducted in Nordrhein, Cologne, and Lower Saxony.29,32,33 We excluded concomitant cancer diagnoses (C00-C97), which turns out to be crucial for need estimation as it leads to much lower numbers of deceased with palliative care need (Murtagh classification (2019) vs. literature; see also eFigures 1 and 2 in eSupplement): cardiovascular (52.5% vs. 83%–90.7%), respiratory (34.7% vs. 42%–61.3%), dementia incl. senility (30.4% vs. 39%–48%) cerebrovascular (21.3% vs. 27%–34.5%), liver (10.4% vs. 14%–20.3%), and neurodegenerative disease (5.0% vs. 5.6%–7.4%).32,33,44
The difference to mortality statistics can be demonstrated by comparing the proportional percentage of deaths attributed to a particular disease in death certificates with claims data. Minimization of these disparities can be an indicator of reduced overestimation. Strikingly, our findings are quite close to the international mortality statistics.32,33,44
Analysis of death certificates in Westphalia (Germany) showed that 22.1% had a cancer diagnosis and, according to the authors, were in need of palliative care. 50 The new classification with estimated 25.2% aligns more closely with these and other findings.16,18,24 In contrast, the Murtagh classification identified 41.9% of deceased as having cancer, which deviates massively from death certificate numbers. The overall estimation of NC deaths according to both approaches was 54.5%–55.4%, which both correspond to previously published literature.16,18,50 Regarding single NC groups, the new classification (2019) resulted in percentages much closer to international mortality statistics than the Murtagh classification: cardiovascular disease (31.1% vs. 23.3%–30.8%), respiratory (3.5% vs. 6.2%–10.1%), cerebrovascular (3.0% vs. 6.6%–7.4%), neurodegenerative (4.0% vs. 1.4%–1.6%), liver (1.0% vs. 1.7%–2.1%), and kidney (3.2% vs. 2.1%–7.6%).18,21 Dementia (32.3% vs. 4.2%–11.7%) is known to be the mostly underreported underlying cause of death in mortality certificates.18,21,24 In hospital claims, which are considered to be the more accurate source for cause of death diagnoses, dementia is much more often represented. 51
Strengths and limitations
This study is based on high-quality retrospective claims data collected for documentation and remuneration purposes, despite the known weaknesses of such data, that is, among ambulatory diagnoses.52–57 Although our study yielded notable results, the main methodological limitation that has already been described by Murtagh et al. 19 is that diagnoses alone may not suffice to infer the necessity for palliative care. 15 Even in existing clinical assessments, diagnosis-related criteria do not seem precise enough (nonspecific grading such as “severe cardiovascular disease”) or are based on examination results (e.g., echocardiography) or treatments (e.g., cardiac implants).43,58,59 The administrative dataset lacks several information that would be crucial for a medical indication of palliative care in an individual, such as symptom burden, prognosis, patients’ and families’ preferences, psychosocial well-being, but also information on possible barriers to access to palliative care such as language and availability of providers in rural areas.42,43,58,60–63
Positively noted, it is favorable that the presence of diagnoses was linked to the crucial and certain information that all individuals had died within a maximum of 1 year. These cases are more likely to have required palliative care based on the given diagnoses compared to cases where the time or occurrence of death is unknown. The information on the occurrence of death was crucial in selecting the diagnoses for the new classification, which may otherwise limit its application for prospective use.
A significant advantage of considering only diagnoses information is the enhancement of international comparability of the results. This approach can facilitate an increase in comparative international population-level studies.17,64 The Murtagh classification is applicable only to datasets where the cause of death is known. In contrast, our method provides an opportunity to achieve internationally comparable results by focusing exclusively on diagnoses, excluding additional needs-related information. This restriction ensures that our findings can be uniformly compared across different countries and studies.
Another limitation of our study can be seen in the process of diagnoses evaluation: On the one hand, a comprehensive evaluation of every specific four-digit documented diagnosis code was carried out by experienced medical specialists. On the other hand, medical experts conducted the selection of diagnoses without considering the perspectives of other groups involved in palliative care, such as other medical specialist groups, nursing staff, pastoral care workers, psychologists, patients, and their families. 65 Therefore, establishing a standardized consensus among these care groups in accordance with disease prevalence and treatment opportunities specific to each country would be beneficial.15,66,67
To estimate individuals’ palliative care needs in claims data as precisely as possible, several approaches can be taken, though this was not the aim of our study. One approach involves recording the aforementioned factors described in international assessments and recommendations within health insurance claims. Another method is linking other data sources, such as causes of death data, or considering further utilization data recorded in health insurance claims, such as medical consultations, treatments, prescribed drugs, and other records characteristic of known patterns of specific disease progression at the end of life.16,25,43,58–60,68 Additionally, methods of excluding sudden deaths due to maternal mortality, suicide, injury (including fractures, poisoning, and external causes like road traffic deaths, which account for 6.4% of the palliative care need worldwide) may be used to narrow the study cohort to chronically ill deceased with non-communicable diseases.15,20,21,69
In summary, the application of our refined diagnosis-based classification can effectively substitute the cause of death information, which is not available in claims data. It provides more realistic results when analyzing palliative care need and coverage in claims data than the widely used Murtagh classification. While palliative care utilization for deceased with cancer increased by 20%-points compared to the application of the inadequate Murtagh classification, palliative care coverage for non-cancer groups remained largely unchanged. This may indicate that non-cancer diagnoses require closer attention in real-life care and future research.
While the new classification approach offers more appropriate results than the Murtagh classification, it does not and cannot provide a complete picture of palliative care need. Being a simple diagnosis-based approach as well, it remains inherently limited in its capacity to provide a comprehensive view of patients’ needs. This shortcoming reduces the approach’s utility for palliative care capacity planning. However, as we also have to consider constrained resources when we plan capacities, it is important to look beyond need estimation. Identifying patient groups that are likely to experience overmedicalized death seems worthy of consideration. This makes them candidates for (earlier) palliative intervention. 70 Against this background, future research should combine need estimation based on the refined ICD10-classification and further needs-associated information as mentioned above with identifying predictors for overmedicalization at the end of life in order to support evidence-based capacity planning and a more precise allocation of scarce resources.
Conclusion
Our classification provides an expandable ICD-10-based approach for analyzing routine data diagnoses of deceased when documented cause of death is not available. The use of this method yields results comparable to mortality statistics, indicating higher palliative care need coverage through grown utilization rates, but also highlighting gaps in non-oncological palliative care coverage. Our refined classification is more specific and therefore more adequate for retrospective claims data analysis on need and coverage of palliative care than the widely used Murtagh et al. 19 classification.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241269599 – Supplemental material for A refined ICD-10 diagnoses-based approach for retrospective analysis of potential palliative care need and coverage in claims data of deceased
Supplemental material, sj-docx-1-smo-10.1177_20503121241269599 for A refined ICD-10 diagnoses-based approach for retrospective analysis of potential palliative care need and coverage in claims data of deceased by Ekaterina Slotina, Bianka Ditscheid, Franziska Meissner, Ursula Marschall, Ulrich Wedding and Antje Freytag in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express particular gratitude to Dr. med. Markus Krause for valuable clinical input.
Author’s contributions
ES and AF drafted the paper. AF and ES designed the study. ES, BD, and FM managed and prepared data. FM, AF, and BD conceptualized, ES performed the statistical analyses. ES, AF, UW, UM, FM, and BD interpreted the data. AF planned, headed and supervised the whole study. All authors revised the manuscript for intellectual content, read, and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ekaterina Slotina, Bianka Ditscheid, Franziska Meissner, and Antje Freytag state having no conflict of interest. Ulrich Wedding as a specialist in internal medicine with a focus on hematology and internal oncology and additional training in palliative medicine provides services for general and specialized outpatient and inpatient palliative care. He further states that he is the deputy spokesperson for the Working Group on Palliative Medicine (AG Palliativmedizin) of the German Cancer Society (Deutsche Krebsgesellschaft, DKG).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research project pallCompare was funded by the German Innovations Fund of the Federal Joint Committee (G-BA) (grant number: 01VSF19026). The funder did not influence the design of the study, the writing of the manuscript and will not influence the collection, analysis and interpretation of data.
Ethics approval and consent to participate
Ethical approval was granted by the Ethics Committee of Jena University Hospital (Reg.-Nr. 2021-2162-Daten). Access to data of statutory health insurance funds for research purposes was possible in accordance with the German Social Law (SGB V § 287). Patient consent was not necessary. The present study is part of the pallCompare project (DRKS00024133). The study was registered with the German Clinical Trials Register German Clinical Trials Register (Reg.-Nr. 2021-2162-Daten). All methods were carried out in accordance with relevant guidelines and regulations in accordance with the Declaration of Helsinki.
Informed consent
Informed consent was not sought for the present study because we did only analyze anonymized claims data from dead insurants.
Trial registration
Deutsches Register für Klinische Studien, German Registry for Clinical Studies, DRKS: DRKS00024133.
Prior publication
Congress contribution: Ekaterina Slotina, Bianka Ditscheid, Franziska Meissner, Ursula Marschall, Ulrich Wedding, and Antje Freytag. Retrospective estimation of palliative care need based on administrative ICD-10 diagnoses from claims data of deceased individuals. 16th Congress of German Network Health Service Research; 04.10.-06.10.2023; Berlin.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.