
Abstract
Consumer products are often associated with fall injuries, but there is limited research on nonfatal unintentional falls in children that examines both the child’s age group and the involvement of consumer products and activities. We combined 2 data sources to investigate products and activities that contribute to fall injuries in children at different developmental ages (ie, <1, 1-2, 3-4, 5-9, 10-14, and 15-19 years). We analyzed data from the National Electronic Injury Surveillance System–All Injury Program for the years 2010 through 2013 and augmented it with product information from the National Electronic Injury Surveillance System. Between 2010 and 2013, children aged <1 to 19 years accounted for 11.1 million nonfatal unintentional fall-related emergency department visits. Fall injuries associated with home furnishings/fixtures were highest among children in age groups <1 year, 1 to 2 years, and 3 to 4 years. In the home furnishings/fixtures product group, beds were the leading contributor to falls. Fall injuries associated with sports/recreation were highest among children in age groups 5 to 9 years, 10 to 14 years, and 15 to 19 years. In this product group, monkey bars and basketball were the leading contributors to falls. Our findings indicate priority areas for falls injury prevention and intervention.
Introduction
Falls are defined as events that result in a person coming to rest inadvertently on the ground/floor or other low level. 1 Children are highly vulnerable to falls. 2 Indeed, falls are the leading cause of nonfatal injuries among children aged <1 to 19 years. Fall injuries in children have substantial impact on US emergency departments (EDs). Approximately 8000 US children are treated for fall-related injuries in EDs every day. 3 Falls, although largely predictable and preventable, too often lead to serious injuries, including soft tissue injuries, fractures, and head injuries.4,5 Age of a child plays a role in fall injuries as injury incidence, causes, and severity vary with age.6-8 Therefore, developmental ages at which children begin to crawl, walk, grasp and reach for things, attend school, and play sports are important considerations in understanding fall injuries in children.
Consumer products, including items and merchandise for use in or around a home, school, or recreational area, contribute to a large proportion of injuries and injury costs in the US. 9 The US Consumer Product Safety Commission (CPSC) monitors injuries related to consumer products and activities. To guide falls prevention programs in the development and dissemination of age-appropriate and developmentally appropriate resources, it is important to understand which everyday products and activities are associated with fall injuries in children at various stages of growth and development. Previous research shows that falls from furniture (eg, bed) and home structures (eg, stairs) are common among younger children who have limited mobility, while older children frequently suffer falls in playground activities and sports.5,9 There is limited research on nonfatal unintentional falls in US children that examines both the child’s age group and the products and activities contributing to fall injuries. Using national estimates, this study aimed to investigate products and activities that contribute to fall injuries among US children aged <1 to 19 years by age group (ie, <1, 1-2, 3-4, 5-9, 10-14, and 15-19 years).
Methods
The study combined 2 data sources to investigate consumer products associated with fall injuries in children. We computed data from the National Electronic Injury Surveillance System–All Injury Program (NEISS-AIP) and augmented it with product information from the National Electronic Injury Surveillance System (NEISS), maintained by the CPSC. Data were from January 1, 2010, through December 31, 2013. NEISS, a weighted national probability sample of consumer product-related injury visits to EDs in a sample of 100 US hospitals, includes data on approximately 400 000 ED injury visits per year for all causes. The expanded system, called the NEISS-AIP, collects data on more than 500 000 ED injury visits per year, both intentional and unintentional. Since 2000, two thirds of the NEISS hospitals have participated in NEISS-AIP. The augmented NEISS-AIP data provide a comprehensive understanding of the contribution of consumer product-related injury to the overall injury problem. NEISS tracks all ED-presented injuries that are associated with a consumer product, as well as those sustained during sports or recreational activities.
We used the CPSC codes for product groups and products. 10 Product groups, established by CPSC, were sports and recreation (eg, basketball, football, soccer), home furnishings and fixtures (eg, beds, tables, chairs), home structures and construction materials (eg, stairs, floors, ceilings and walls), toys (eg, skateboards, scooters), child nursery equipment (eg, car seats, baby gates, baby walkers), personal use items (eg, footwear, daywear, pens and pencils), and other products (eg, home electronics, packaging and containers). Product codes for sports identify not only injuries associated with the equipment or apparel associated with the sport, but participation in the sport, even if the injury does not involve a specific product.
We restricted analysis to children aged <1 to 19 years and analyzed unintentional nonfatal fall injuries presented in EDs, including those admitted, treated and released, or left against medical advice. We aggregated data from 2010 to 2013 to get a reliable sample size. Cases with missing age were excluded from the analysis (n = 354). We examined fall injury rates per 100 000 for boys and girls in different age groups (<1, 1-2, 3-4, 5-9, 10-14, and 15-19 years). We also examined frequencies of fall injuries related to product groups and products. All statistical analyses were performed in SAS version 9.4.
Ethical Approval and Informed Consent
This study was exempt from institutional review board approval due to the nature of secondary analysis with de-identified data.
Results
Between 2010 and 2013, children aged <1 to 19 years accounted for 11 146 277 nonfatal unintentional fall injuries seen in EDs. Fall injury rates were highest in children aged 1 to 2 years (6844.6 per 100 000), followed by children aged 3 to 4 years (4766.4), <1 year (3642.5), 5 to 9 years (3201.4), 10 to 14 years (2913.8), and 15 to 19 years (2101.9). Rates were higher among boys (3760.0) and Whites (3434.0). Table 1 displays fall injury rates by sex and race/ethnicity across different age groups. The provided Supplementary Table 1 (available in the online version of this article) includes counts and standard errors for fall injuries by sex and race/ethnicity.
Nonfatal Unintentional Fall Injury Rates per 100 000 in Children Aged <1 to 19 Years, the United States, 2010 to 2013.

Abbreviation: ED, emergency department.
Other disposition includes children who left against medical advice, left without being seen, and unknown.
Seventy-four percent of fall injuries in children were related to consumer products. Table 2 shows the leading product groups associated with fall injuries. Product groups accounting for falls were sports and recreation products (22.7%), home furnishing and fixtures (21.6%), home structures and construction materials (18.5%), toys (5.5%), child nursery equipment (1.8%), personal use items (1.4%), and other products (2.6%). As shown in Table 3, in the sports and recreation product group, basketball (2.8%), monkey bars (2.6%), and football (1.8%) were associated with most falls. In the home furnishing and fixtures product group, beds (7.0%), tables (3.2%), and chairs (3.2%) were associated with most falls. In the home structures and construction materials product group, stairs (7.6%), floors (6.2%), and ceilings and walls (1.1%) were commonly related to falls.
Leading Product Groups Associated With Nonfatal Unintentional Fall Injuries in Children by Age Group, the United States, 2010 to 2013.

Other products include home electronics, packaging and containers, yard and garden equipment, products covered by existing regulations, and unknown products.
Leading Products Contributing to Nonfatal Unintentional Fall Injuries in Children by Age Group, the United States, 2010 to 2013.
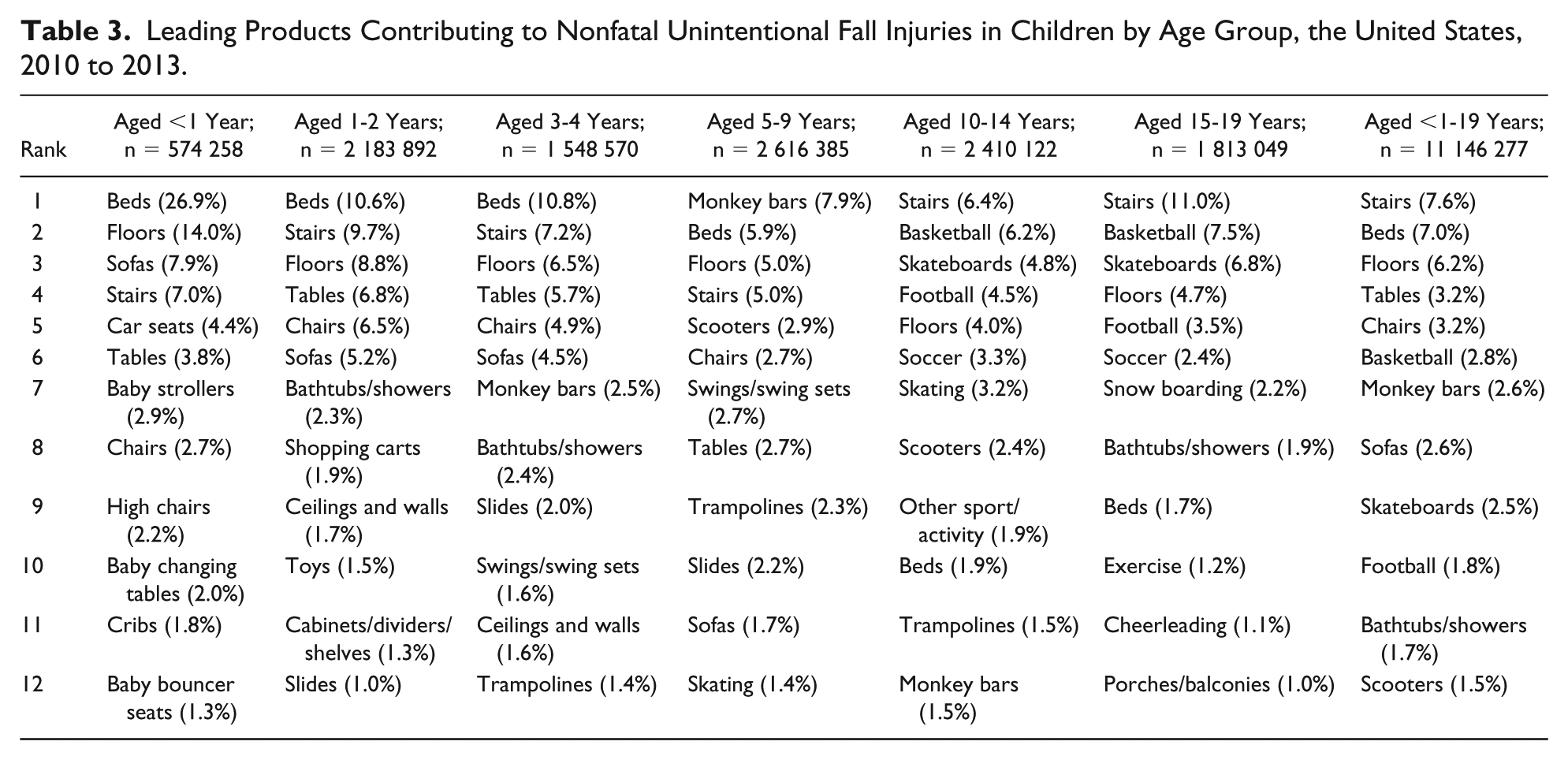
Product groups contributing to fall injuries varied across age groups. Home furnishings and fixtures accounted for most falls in children aged <1 year (45.7%), 1 to 2 years (37.7%), and 3 to 4 years (34.5%). In this product group, beds, sofas, and tables were primarily related to falls in children aged <1 year. Similarly, beds, tables, and chairs were related to falls in children aged 1 to 2 years and 3 to 4 years. Sports and recreational products and activities contributed to most falls in children aged 5 to 9 years (28.9%), 10 to 14 years (38.2%), and 15 to 19 years (30.3%). In this product group, monkey bars, swings, and trampolines were commonly associated with falls in children aged 5 to 9 years. Basketball, football, and soccer were frequent contributors to falls in children aged 10 to 14 years and 15 to 19 years.
Discussion
Although not all childhood falls require medical attention, many result in medically treated injuries. Falls are common among children, and they are the most common principal mechanism of traumatic brain injury in all age groups. 11 A serious injury from a fall can have a lasting impact on the child’s behavioral and emotional development. This research confirms prior findings that childhood falls with injury typically involve consumer products. 4 We found that products related to sports and recreation, home furnishing and fixtures, and home structures and construction materials accounted for nearly three fourths of the fall injuries in children. Because children’s age and stage of development affect fall injuries, this study examined consumer products associated with falls in children by age group.
Stairs are commonly associated with falls across all age groups. 9 In this study, stairs were the first leading consumer product related to fall injuries among children aged 10 to 14 years and 15 to 19 years, the second leading product among children aged 1 to 2 years and 3 to 4 years, and the fourth leading product among children aged <1 year and 5 to 9 years. Accidental stair falls frequently occur due to distractions, improper foot placement or missing handrails, or tripping on objects on stairs, and the structural design of stairs also affects the risk of falls. For younger children, use of home safety devices, such as stair gates and guard rails, are recommended preventive measures.7,12 Falls in older children may be reduced by avoiding use of prefabricated stairs in new construction, which often have the top step with a different going/rise ratio than the lower steps.13,14 Building codes for new construction have been changing to require safer stairway tread-to-riser ratios, smooth and graspable handrails, and closely spaced side-rails, but retrofitting handrails in existing construction merits evaluation. 15
Children less than 5 years often fall by rolling off surfaces they are placed on, or by being dropped. Our findings show that a large proportion of fall injuries in infants, toddlers, and preschoolers were associated with home furnishings and fixtures. When young children fall, they are at heightened risk of head injuries from falls given their inability to shield themselves during a fall.11,16 Falls from beds have been consistently noted as the leading contributor to injuries among young children and a major fall risk throughout life.9,17 Yet, bed safety interventions remain largely unevaluated. Strategies that support parent education and home safety visits focusing on fall risks have been linked to knowledge, attitudes, and behaviors that reduce falls,7,18 though their direct impact on falls needs further evaluation. Research is needed to evaluate the effects of parental education on bed safety. Because fall outcome varies with fall height and surface type, research should also examine how fall injury frequency and severity differ in homes where beds are on frames versus on the floor, by the height of mattress/box-spring set, and by the type of floor surface (eg, hardwood, tile, carpet). Test facilities used to evaluate stairway design may be used to assess safe bed geometry.
Infants less than 1 year also experience falls from child nursery equipment, for example, car seats. We identified that fall injuries from car seats are common among infants. Car seats, often used as infant carriers, are dangerous when carried outside the car and handled inappropriately. Falls from car seats occur while infants are being carried or being placed on an elevated surface in their car seat. 19 When placed on tables, countertops, or other high surfaces, car seats can flip over leading to falls in infants. Parental supervision and education regarding the dangers of car seat misuse are critical to prevent falls in infants.
Among children aged 5 to 19 years, sports and recreational products and activities accounted for most fall injuries. Monkey bars, the second leading cause of injury costs among children aged 5 to 9 years, 9 proved to be the leading product associated with fall injuries. Although football causes most injury costs among children aged 10 to 19 years, 9 basketball was associated with the greatest percentage of sports and recreation fall injuries for this age group. These findings highlight the need for playground safety. The Public Playground Safety Handbook, published by the US CPSC, 20 provides recommendations on playground equipment and materials to mitigate the risk of falls. Children aged 5 to 9 years require adequate supervision to ensure proper playground safety and adherence to playground rules and equipment standards. Enforcement of safety rules and proper use of safety gear during competitive sports are necessary for children aged 10 to 19 years. Given Ball et al’s 21 findings that switching to forgiving playground surfaces result in a greater child risk-taking and laxer parental supervision rather than in injury prevention, a combination of safety equipment, rules, and supervision may be necessary.
Injury prevention strategies include education, enforcement, and engineering, collectively referred to as the “Three Es.” Reviews on falls in children support caregiver education and supervision as an important prevention recommendation 1 but underscore the need for formal investigation on the effectiveness of falls prevention strategies. 12 In the “Three Es” of injury prevention, engineering solutions are the most effective way for removing injury risks. For example, baby walker redesign mandated by CPSC reduced associated stairway falls by 88% between 1994 and 2008. 22 Implementation and evaluation of effective falls prevention strategies should be a child safety priority.
Limitations
Despite the strengths of the augmented NEISS-AIP data in providing national estimates, our study has limitations. We did not examine how fall injuries in children vary by socioeconomic status, as those data were not available. Previous studies on falls indicate that children with low socioeconomic status are at increased risk for fall injuries 23 and injuries in general. 24 Also, we were unable to thoroughly investigate where frequent falls occurred due to an absence of location information for a large proportion of injuries. We found that more than one third (34%) of fall injuries in the study occurred at unknown locations. Therefore, it is highly likely that we undercounted home injuries. Missing location was not a surprise as location of injury incidents are often underreported in vital statistics. 25 ED visit and hospitalization data are primarily collected for administrative and billing purposes, and there is no incentive for including codes with no financial incentives. 26
The study included only patients admitted through the ED. It omitted inpatient admissions that did not go through the ED and cases treated at urgent care clinics, doctors’ offices, and school health clinics. For every fall case treated in the ED, we estimate that an additional 1.2 fall injuries resulted in treatment in a doctor’s office or outpatient department (ratio based on the methodology detailed in a CPSC report 27 ). Thus, our findings are based on ED cases, which represent less than half of all medically treated falls. Last, we did not thoroughly assess the severity or bodily location of fall injuries in children. The occurrence and severity of falls depend on various factors, including height of the fall, type of surface, location (eg, day care or home), individual anatomy (eg, bone structure, fat composition), and cause of the fall (eg, fall from a baby walker, fall down stairs).1,23,28 Previous research indicates that head and neck injuries are more frequent in children younger than 1 year, upper extremity injuries are higher among children aged 3 to 8 years, and lower extremity injuries are higher among children aged 12 to 17 years. 5 We observed that for the 3 dominant product groups, more than half of the fall injuries involving home furnishings and fixtures and home structures and construction materials were to the head or face, while sport injuries commonly involved fractures to the lower arm and wrist (data not shown but available on request). Additional research is needed to investigate severity and preventability of falls associated with consumer products across age groups.
Conclusions
This study identifies consumer products associated with nonfatal unintentional fall injuries in children across varying stages of development. Our findings based on augmented NEISS-AIP data provide a comprehensive understanding of products and activities that contribute to fall injuries seen in EDs. The patterns of falls identified in this study will help set priorities for fall prevention programs and suggest development of tailored strategies to fit children’s stages of growth and development.
Supplemental Material
SupplementMaterial_CL – Supplemental material for Consumer Products Contributing to Fall Injuries in Children Aged <1 to 19 Years Treated in US Emergency Departments, 2010 to 2013: An Observational Study
Supplemental material, SupplementMaterial_CL for Consumer Products Contributing to Fall Injuries in Children Aged <1 to 19 Years Treated in US Emergency Departments, 2010 to 2013: An Observational Study by Bina Ali, Bruce Lawrence, Ted Miller, David Swedler and Jennifer Allison in Global Pediatric Health
Footnotes
Author Contributions
BA, TM, and DS: performed literature review.
BA and BL: conducted analysis.
BA: developed the first draft of the manuscript.
BL, TM, DS and JA: provided critical revisions to the manuscript.
All authors contributed to and have approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under the Child and Adolescent Injury and Violence Prevention Resource Centers Cooperative Agreement (U49MC28422). This information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.