
Abstract
Objectives:
The prevalence and correlates of sexual risk behaviors among unmarried youth in Thailand are poorly documented. The objectives of this study were to compare the differences in sexual behaviors across age groups and gender and to identify the relationships between sexual risk behaviors and general health risk behaviors among unmarried Thai youth.
Methods:
A population-based, nationally representative, cross-sectional survey was conducted between January and March 2013. The Thai version of the Youth Risk Behavior Survey questionnaire was used to collect data from 800 unmarried Thai youth.
Results:
Majority of the respondents (65.9%) had not engaged in any sexual risk behavior, 18.7% had engaged in 2–3 sexual risk behaviors, and only 5.5% had engaged in a single sexual risk behavior. Current sexually active youth had higher risk of participating in physical fights (odds ratio = 3.41, 95% confidence interval = 1.53–7.57), smoking cigarette (odds ratio = 4.05, 95% confidence interval = 1.89–8.67), and drinking alcohol (odds ratio = 2.17, 95% confidence interval = 1.08–4.36).
Conclusion:
Thai youth were more likely to be involved in multiple sexual risk behaviors than a single sexual risk behavior. Physical fighting was the strongest general health risk behavior associated with the sexual risk behaviors, followed by substance abuse.
Keywords
Introduction
Adolescence is a critical period of changes in physical, psychosocial, emotional, cognitive, and sexual aspects. Adolescent sexuality has changed over the past few decades, with adolescents reaching puberty and having sexual experiences earlier than before. 1 Previous research reported that the average age of menarche decreased from 12.76 years in the 1960s data to 12.5 years in the 1988–1994 data. 2 Results from the 2013 Youth Risk Behavior Surveillance showed that the prevalence of ever having sexual intercourse among Thai youth was slightly lower than that reported in American youth (41.9% and 46.8%, respectively).3,4
According to the problem-behavior theory developed by Richard Jessor, the involvement of adolescents in any kind of problem behavior was more likely to predict their involvement in other kinds due to the impact of socio-ecological factors. Multiple problem behaviors may occur as a function of a single behavioral syndrome. 5 Relationships between sexual risk behaviors and general health risk behaviors have been identified in some research studies in both the Asian and Western contexts.6,7 A previous research conducted in Thailand reported that high school students who drank alcohol were more likely to smoke, carry a weapon, feel depressed, attempt suicide, use illicit substance, and have sexual intercourse. 8 Another study among unmarried Asian youth reported the co-occurrence between sexual behaviors and general health risk behaviors that included smoking, drinking, drug use, and running away from home. 9 Similar findings in the United States reported that a history of sexual activity featured strongly as a behavior that co-occurred with other risk behaviors including suicide, cigarette smoking, and using cell phone while driving. 10 Although many studies have provided evidence for relationship between sexual risk behaviors and general health risk behaviors, others have reported negative relationships.11,12
At present, there is an increasing concern in the Thai society regarding the sexual risk behavior among the youth and its consequences, which include teenage pregnancy, sexually transmitted diseases, sexual violence, emotional problems, and co-occurrence of other general health risk behaviors. According to the Thai Ministry of Public Health (MoPH), adolescent birth rates increased from 47 per 1000 in 2002 to 54 per 1000 in 2012. 13 Data from a study in Northern Thailand reported the prevalence of Chlamydia trachomatis, Neisseria gonorrhoeae, and HIV infections among youth to be 2.8%, 0.3%, and 0.3%, respectively. 14
To the best of our knowledge, there was no study focusing on the correlation between various forms of sexual risk behaviors and the relationship between sexual risk behaviors and general health risk behaviors among Thai youth. The objectives of this study were to compare the differences in sexual behaviors across age groups and gender and to identify the relationships between sexual risk behaviors and general health risk behaviors among unmarried Thai youth.
Materials and methods
Study design and participants
The Thai Youth Risk Behavior Survey (YRBS) is a population-based, nationally representative, cross-sectional survey completed between January and March 2013. Adolescents aged between 13 and 24 years old were included in the study using stratified multistage sampling. The primary strata consisted of Bangkok, central region, northern region, northeastern region, and southern region of Thailand. Two provinces were randomly selected from each of the four regions (Chiang Mai, Phrae, Nakhon Ratchasima, Nong Khai, Nakhon Pathom, Samut Sakhon, Nakhon Si Thammarat, and Songkhla). Each province was secondarily stratified into urban and rural districts. Households were selected within each cluster using enumeration, followed by simple random sampling method. A respondent was randomly selected from each household using “Kish Grid” method. 15 The respondents and their parents were asked to give consent to participate in the survey. Respondents who agreed to participate were instructed to complete the self-administered questionnaire in a private area to ensure privacy from family members. Ethics approval was obtained from the Srinakharinwirot University, Thailand (reference: SWUEC/EX22/2555).
Questionnaire
The 2011 National YRBS questionnaire is a self-administered questionnaire that has been developed and tested for reliability and validity by the US Centers for Disease Control and Prevention. 16 The questionnaire was translated into the Thai language and reviewed by a developmental pediatrician and research teams from the Mahidol University, Thailand. Prior to study initiation, the pilot testing has been conducted to validate the questionnaire for accuracy and appropriateness. A total of 50 adolescents were instructed to complete the questionnaire and interviewed about the appropriateness of the questionnaire. In all, 22 questions were deleted from the final Thai version questionnaire. The Thai version YRBS questionnaire contained 75 multiple choice questions that measured six categories including unintentional injuries and violence, tobacco consumption, alcohol and marijuana consumption, sexual behaviors, dietary behaviors, and physical activity.
In this research study, we selected eight questions from the sexual behaviors category. These questions were as follows: (1) Have you ever had sexual intercourse? (2) During your life, with how many people have you had sexual intercourse? (3) During the past 3 months, with how many people did you have sexual intercourse? (4) How old are you when you had sexual intercourse for the first time? (5) The last time you had sexual intercourse, did you or your partner use a condom? (6) The last time you had sexual intercourse, what one method did you or your partner use to prevent pregnancy? (7) During the past 12 months, did your boyfriend or girlfriend ever hit, slap, or physical hurt you on purpose? and (8) Have you ever been physically forced to have sexual intercourse when you did not want to? Risky sexual behavior was defined as all the selected sexual behaviors except for “ever had sexual intercourse.”
We selected five general health risk behaviors, including (1) in a physical fight one or more times during the past 12 months, (2) smoked cigarette on at least 1 day during the past 30 days, (3) had at least one drink of alcohol on at least 1 day during the past 30 days, (4) ever used marijuana one or more times during their life, and (5) attempted suicide one or more times during the past 12 months.
Age groups in the sample
There were four age groups identified in the sample: (1) early adolescence (ages 13–14 years), (2) middle adolescence (ages 15–17 years), (3) late adolescence (ages 18–21 years), and (4) early adult (ages 22–24 years).
Statistical analysis
Descriptive statistics characterizing the sample and estimating the prevalence of sexual risk behaviors were generated. Spearman correlation was used to report the correlation between the sexual risk behaviors. Exploratory factor analysis was used to explore the factors that were extracted from sexual risk behaviors. Chi square was used to test the independence of the age groups, gender, and sexual risk behaviors of the samples. Odds ratio (OR) was used to measure the association between the sexual risk behaviors and the general health risk behaviors. Statistical analysis was performed using SPSS software (version 23.0; SPSS Incorporated).
Results
Demographic characteristics
In total, 1000 adolescents were invited, of which 920 adolescents agreed to participate in the survey. Response rate was 92%. In all, 120 respondents were excluded from this study because they have been married or divorced. Finally, data from 800 unmarried respondents were analyzed. About 60% of respondents were studying in school, 57.8% were boys, and 97% were Buddhists. Approximately 80% of students were studying in secondary school. The highest proportion of respondents was in the middle adolescent group (38.5%) followed by late adolescent group (33.5%), early adulthood group (19.1%), and early adolescent group (8.9%), respectively. The mean age of respondents was 18.20 years (standard deviation (SD) = 3.41). The highest proportion of respondents came from the northeast region (31.9%), followed by the central region (21%), northern region (18.1%), southern region (17.6%), and Bangkok (11.4%), respectively.
Prevalence of single and multiple sexual risk behaviors
Table 1 shows the prevalence of sexual risk behaviors. Approximately 30% of respondents ever had sexual intercourse and 24.1% were currently being sexually active. The prevalence of “ever had sexual intercourse” and “used any prevention method during the last sexual intercourse” was significantly higher among older respondents. The prevalence of sexual risk behaviors was significantly higher in boys than girls in all items except for not using condom and contraceptive method during the last sexual intercourse. The prevalence of sexual experience, sexual prevention, and sexual violence factors was not significantly different between the various age groups. The prevalence of sexual experience (53.7% vs 4.7%, p < 0.001) and sexual violence factors (21.5% vs 7.0%, p < 0.05) was significant higher among boys than girls.
The prevalence of sexual behaviors by age group and gender.

Only respondents who ever had sexual intercourse.
Significance of bold values represents n, % and p value of sexual risk behavior factors.
Table 2 shows the prevalence of multiple sexual risk behaviors. Majority of the respondents (65.9%) had not engaged in any sexual risk behavior, 18.7% had engaged in two to three sexual risk behaviors, and only 5.5% had engaged in single sexual risk behavior.
The prevalence of multiple sexual risk behaviors by age group and gender.

Correlation and factor loading of sexual risk behaviors
Table 3 shows the correlation coefficients between sexual risk behaviors. Current sexually active behaviors significantly correlated with “having multiple sexual partners” and “being physically hurt by boy/girlfriend.” Having multiple sexual partners significantly correlated with “having early sexual experience.” Respondents’ behavior of not using condoms significantly correlated with “did not use any method to prevent pregnancy.” Physical hurt by boy/girlfriend significantly correlated with “ever being physically forced to have sexual intercourse.”
The correlation between sexual risk behaviors and factor loadings with the first principal component.

p < 0.01.
p < 0.05.
The Factor Analysis yielded 3 factors with eigenvalues greater than 1 and all factor loadings greater than 0.5 was acceptable. The “sexual experience” factor consisted of 3 risk behaviors including “current sexually active” (factor loading = 0.591), “having multiple sexual partners” (factor loading = 0.832), and “having early sexual experience” (factor loading = 0.665). The “sexual risk prevention” factor consisted of 2 risk behaviors including “did not use condom” (factor loading = 0.859) and “did not prevent pregnancy” (factor loading = 0.865). The “sexual violence” factor consisted of 2 risk behaviors including “being physically hurt by boy/girlfriend” (factor loading = 0.812) and “ever physically forced to have sexual intercourse” (factor loading = 0.808).
Association between sexual behaviors and general health risk behaviors
Table 4 shows the association between first-order factor of sexual behaviors and general health risk behaviors. Youth having sexual experience had higher risk of participation in physical fights (OR = 3.70, 95% confidence interval (CI) = 1.93–7.10), drinking alcohol (OR = 2.16, 95% CI = 1.02–4.60), and using marijuana (OR = 2.91, 95% CI = 1.37–6.18). Both the factors of sexual prevention (OR = 1.93, 95% CI = 1.01–3.72) and sexual violence (OR = 3.20, 95% CI = 1.51–6.82) predicted higher risk of participating in physical fights. We also found the association between sexual behaviors and general health risk behaviors. Current sexually active youth had higher risk of participating in physical fights (OR = 3.41, 95% CI = 1.53–7.57), smoking cigarette (OR = 4.05, 95% CI = 1.89–8.67), and drinking alcohol (OR = 2.17, 95% CI = 1.08–4.36). Youth having multiple sexual partners had higher risk of substance abuse as well as engaging in physical fight (OR = 2.90, 95% CI = 1.30–3.99), smoking cigarette (OR = 2.30, 95% CI = 1.15–4.62), drinking alcohol (OR = 2.06, 95% CI = 1.07–3.96), and using marijuana (OR = 2.75, 95% CI = 1.49–5.06). Youth reporting early sexual experience had higher risk of participating in physical fights (OR = 7.10, 95% CI = 3.46–14.54) and smoking cigarette (OR = 15.19, 95% CI = 2.00–114.85). Youth who reported being physically forced to have sexual intercourse had higher risk of participating in physical fights (OR = 6.91, 95% CI = 2.41–19.73), using marijuana (OR = 7.51, 95% CI = 2.59–21.77), and attempting suicide (OR = 7.90, 95% CI = 1.64–38.11).
The association between sexual risk behaviors and general risk behaviors.
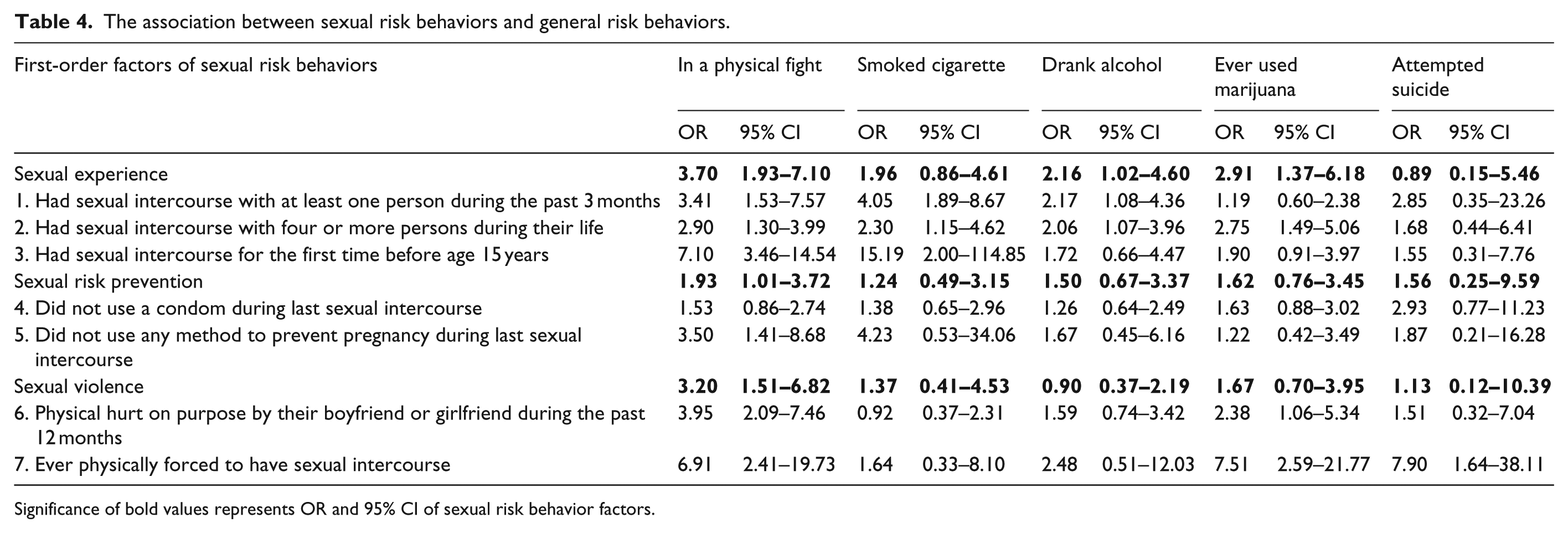
Significance of bold values represents OR and 95% CI of sexual risk behavior factors.
Discussion
The prevalence of ever having sexual intercourse was higher in this study when compared to the data collected in 2001 by the Bangkok YRBS (32.5% vs 26.5%). 17 Compared with the 2013 United States YRBS, the prevalence of ever having sexual intercourse and currently being sexually active were higher in American youth than in Thai youth. 3 Compared with the European countries, the prevalence of early sexual intercourse before age 15 years among Thai youth (5.1%) was lower than those reported in Austria (21.1%), Belgium (13.5%), Denmark (35.4%), France (16.3%), Germany (15.2%), Iceland (17.3%) and United Kingdom (15.9%). 18 Data from this study found that the prevalence of sexual risk behavior was significantly higher in boys than among girls in Thailand. The gender difference in sexual risk behaviors has been identified in most Asian and Western countries.3,19–21
Previous research found that girls were more likely to report being physically or sexually abused by intimate partner than boys. 22 In this study, it is interesting to note that 3.2% of boys reported being forced to have sexual intercourse but none of the girls did. Underreporting among female respondents might be one reason for this finding. However, recent research demonstrated that sexual violence against boys is a significant problem that has been neglected. A few population-based studies conducted in developing countries reported the prevalence of sexual assault among male adolescent ranges from 3.6% to 20%. 23 Qualitative research should be conducted to explore the root cause of this problem.
According to the sexual developmental theory, early adolescence coincides with the onset of puberty, sexual curiosity, and exploration that may lead to initiating sexual experimentation.24,25 In middle adolescence, the youth begin to have romantic relationships characterized by serial monogamy or having several partners at once and over brief periods of time. They do not fully understand the consequence of their actions and may engage in sexual risk behaviors such as unprotected sexual activity. Later, adolescents have more understanding of the risks and consequences and develop more intimate and serious relationships.24,25 The finding from this study showed that the majority of Thai youth start initiating sexual experience after the middle adolescent period and develop more mature relationships during late adolescent or early adulthood. Large numbers of Thai youth had unprotected sexual intercourse even when they were in early adult age group. This shows lack of knowledge and concern in consequences of unsafe sexual intercourse.
According to the problem-behavior theory developed by Jessor, 7 the involvement of a youth in any one problem behavior increases the likelihood of involvement in other problem behaviors. The 2011 Philadelphia YRBS, which analyzed co-occurrence among eight risk behaviors, reported that more than half of youth were engaging in two to four risk behaviors. 12 Similar to the previous research works, results from this study found that Thai youth were more likely to be involved in two to three sexual risk behaviors than a single sexual risk behavior. It is important for a health professional to consider that when first sexual risk behavior has been established, the other sexual risk behaviors should also be monitored. We also found significant correlation between sexual risk behaviors and general health risk behaviors. Respondents who participated in sexual risk behaviors had strong correlation with a physical fight and substance abuse. The evidence for how sexual risk behaviors relates to other health risk behaviors is mixed. The YRBS in US students found that alcohol, tobacco, marijuana use, and physical fight were strong predictor for an increased number of sexual partners among public high school adolescents. 26 Another study in US students found that almost 50% of male fighter reported having multiple partners and did not use condom. 27 A cross-sectional study in Chinese students reported that cigarette smoke and illicit drug use were related to unprotected sexual intercourse and younger age of first sexual intercourse was related to having multiple sexual partners. 28 Although many studies have identified the association between sexual risk behaviors, physical fight, and substance abuse, other studies found no significant relationships. A study in three Asian cities found that sexual risk behavior among unmarried youth correlated with general health risk behaviors but with different patterns across the three settings. Adolescents who were at high risk of sexual behavior were more likely to have a higher risk of substance abuse and running away from home. However, sexual risk behavior did not increase the risk of physical fighting in Hanoi and of gambling in Shanghai and Taipei. 11 A study in Kenya has reported non-significant relationship between sexual risk behaviors and substance abuse among out-of-school youth. 29
The present research found that respondents who reported being physical abuse by dating partners were more likely to participate in a physical fight and use marijuana. This finding has been confirmed by an earlier research conducted in United States. Silverman et al. 22 reported that physical and sexual dating violence against adolescent girls increase risk of substance use, unhealthy weight control behaviors, first intercourse before age 15 years, pregnancy, and attempted suicide. Previous research has identified a strong association between alcohol drinking and sexual violence and unwanted sexual experience. 30 Many researchers have identified risk factors of sexual violence that included being young, consuming alcohol or drugs, having previously been raped or sexually abused, having many sexual partners, involvement in sex work, becoming more educated, and poverty. 23 A cross-sectional study in central Thailand found that the female youth who were currently drinking alcohol were more likely to experience dating violence and ever being forced to have sexual relationship. 31 A study in lowland Thai youth and ethnic minority in Northern Thai province found the association between ever having sex and ever drinking alcohol in the past year. 32
This study had several limitations that should be noted. First, this survey relied on self-reported data by the respondents. Adolescents may be reluctant to fully disclose their sexual behavior, especially girls and young respondents. However, one study in American youth demonstrated that early adolescent girls can provide reliable romantic and sexual information. 33 In this survey, we tried to minimize underreporting by stressing the confidentiality of the data and finding a private place for respondents to fill the questionnaire. Second, although this study was a cross-sectional study, however, youth sexual risk behaviors change rapidly over time. Hence, a longitudinal study should be done to closely monitor sexual risk behaviors and their consequences. Third, we did not conduct a power of analysis because the sample size selected for this study was based on the Thai YRBS.
Conclusion
Thai youth were more likely to be involved in multiple sexual risk behaviors than single sexual risk behavior. Physical fighting was the strongest general health risk behavior associated with sexual risk behaviors, followed by substance abuse.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Srinakharinwirot University, approval number SWUEC/EX22/2555.
Informed consent
Written informed consent was obtained from all subjects or their legally authorized and minor subjects prior to study initiation.