
Abstract
Objective. The objective of this study was to determine factors contributing to improvements in infant mortality rates (IMR) and composite morbidity-mortality in very-low-birth-weight (VLBW) infants after initiating a new perinatal program in 2009 at Regional One Health (ROH). VLBW infants account for 67% of infant deaths. Design. This is a pre-/postintervention cohort study of prospectively gathered data. Population. VLBW infants delivered at ROH during the 2004 to 2015 study period. Setting. ROH is a Regional Perinatal Center affiliated with the University of Tennessee Health Science Center. Methods. We studied 2364 consecutive VLBW infants. Multivariate models were applied to determine factors contributing significantly to the reduction in the outcome measures as well as trends over time. Main Outcome Measures. Primary outcomes were IMR and composite morbidity-mortality rates. Standardized, risk-adjusted mortality and composite morbidity ratios were also reported as defined by the Vermont Oxford Network. Results. Mortality declined from 15.5% in Pre-Implementation to 13.1% in Post-Implementation (P = .093), corresponding to an 18% reduction in odds. The combined factors of composite morbidity-mortality rate decreased from 55.7% in Pre-Implementation to 43.9% in Post-Implementation (P < .0001), representing a 38% reduction in odds. Standardized, risk-adjusted mortality and composite morbidity ratios improved during the study period from 20% above to 20% below the expected rate. Increases in the administration of antenatal steroids, surfactant administration, cesarean delivery, and perhaps other programmatic changes that were observational and unaccounted in the model were associated with improvements in outcome measures. Conclusions. Decreased mortality and composite morbidity-mortality in VLBW infants delivered at ROH were found following the initiation of a new perinatal program.
Introduction
The infant mortality rate (IMR) is the rate of death of live-born infants less than 1 year of age per 1000 live births, and it is commonly accepted as a measure of the general health and well-being of a population. It is associated with a variety of factors, such as maternal health, quality of and access to medical care, socioeconomic conditions, and public health practices.1-3
Over an extended period of time, Memphis has had one of the highest IMRs among US cities. In 1932, the US Census Bureau reported that Memphis had the highest IMR of any city of 100 000 or more people in the US birth registration area.4,5 Until 2008, the IMRs in some of the Memphis ZIP codes were comparable with those of a third world country. 6 More than 60% of the infant deaths in Memphis occur during the neonatal period.7,8
Very-low-birth-weight (VLBW) infants are a significant contributor to the high infant mortality in Memphis. They represent 2.5% of all live births in Shelby County, and account for 67% of infant deaths.7,8 Eighty-four percent of VLBW infant deaths occur during the neonatal period. 9
More than 60% of VLBW infants in Memphis are delivered at Regional One Health (ROH; Table 1). The number of these infants at ROH has ranged from 3.5% to 5.5% (median = 4.7%) of total deliveries from 2004 to 2015; this is more than 3 times the national average and 1.5 times higher than the national average for African Americans. 10
Shelby County and Regional Medical Center, Regional One Health (ROH) Data.
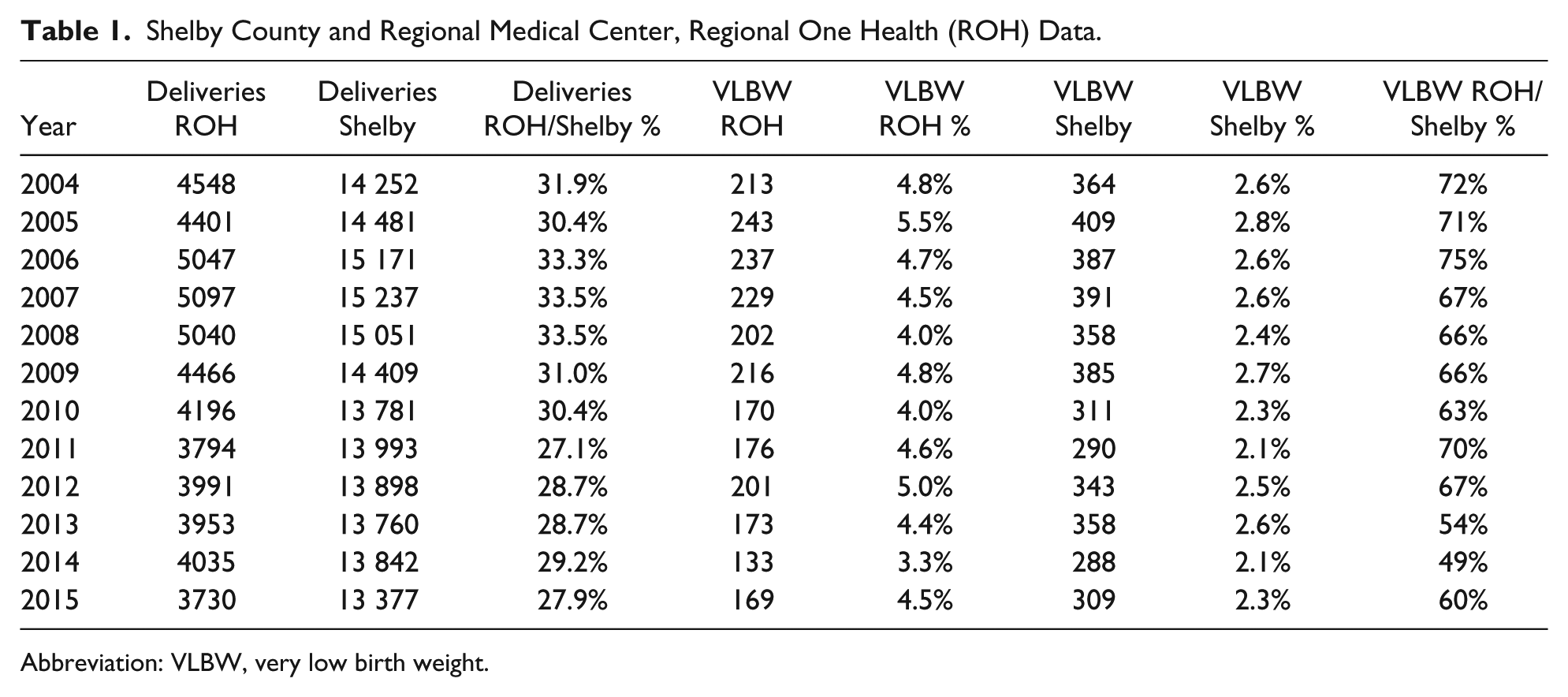
Abbreviation: VLBW, very low birth weight.
The Department of Obstetrics and Gynecology and the Division of Neonatology at the University of Tennessee in Memphis reorganized the perinatal program. Many changes started to occur in the organization, management of labor and delivery (L&D), and in the communication among all teams involved. The changes were designed to improve obstetrical and neonatal care at ROH.
In this study, we report the mortality and composite morbidity-mortality for VLBW infants following delivery and during their hospital stay; 5 years before (2004 through 2008) and 7 years after (2009 through 2015) the beginning of our new perinatal program.
Methods
Design and Setting
This work was a study of prospectively collected data on VLBW infants delivered at ROH from 2004 to 2015, 5 years before and 7 years after the beginning of a new perinatal program. ROH is 1 of 5 Regional Perinatal Centers in Tennessee and is affiliated with the University of Tennessee Health Science Center (UTHSC).
The UTHSC and the ROH institutional review board approved this study.
Study Population
VLBW infants included those infants with a birth weight from 500 g up to and including 1500 g. The data were tracked and stored in an online database called Slim Prim, which is accessed through a customizable web application. VLBW infants’ data were extracted from our center’s Vermont Oxford Network (VON) reports. The VON, a worldwide voluntary collaboration of health care professionals established in 1988, has as its mission to improve the quality and safety of medical care for newborn infants and their families through a coordinated program of research, education, and quality improvement. Today, VON is composed of over a 1000 neonatal intensive care units (NICUs). 11
Perinatal Program at ROH
The Division of Neonatology, starting in 2006, made changes in the NICU designed to follow national guidelines. However, it was in June 2008 that both the Department of Obstetrics and Gynecology and the Division of Neonatology at UTHSC started a reorganization of the perinatal program at ROH designed to improve obstetrical and neonatal care. Our new program included 3 overlapping phases: Observation, Awareness, and Implementation. The Observation phase examined the obstetrical and neonatal care provided at ROH, particularly looking for opportunities for improvement. This initial phase went from June to September 2008.
During Observation, the opportunities we found for improvement were numerous. We realized that there were differing definitions for the same clinical conditions. For example, a survey on the definition of tachysystole among 42 doctors and nurses resulted in 12 different definitions. Also, there were no protocols for the management of conditions such as diabetic ketoacidosis, intrauterine growth restriction, twin gestations, and obesity. Most often, these conditions were managed by the obstetrician without input from the maternal-fetal medicine (MFM) specialist. Many neonates were admitted to the NICU with a temperature below 36°C, because the operating and delivery rooms did not have a protocol regarding an optimal temperature. There was poor communication between obstetricians and neonatologists. There was no peer review of cases that ended with low cord pH and Apgars, or other complications. The Morbidity and Mortality Conference consisted of the presentation of an interesting case selected by the residents. The attendance at didactic conferences for the residents was poor, and it was not an expectation. Until 2008, there were no structured rounds for the L&D area. In the case of an emergency for maternal hemorrhaging, the time before a blood transfusion was started could be 45 minutes or more. Until 2008, there was no mandatory training for the L&D personnel.
The Phases
The Awareness phase (started in October 2008) included meetings, discussions, and surveys, including all personnel involved with the Department of Obstetrics and Gynecology, the Division of Neonatology, and hospital administration. Each group acknowledged problems, sought areas for improvement, and spread awareness of changes we were going to make. A SWOT (strengths, weaknesses, opportunities, and threats) analysis was conducted among all personnel involved with L&D, and its results were made aware to the entire team.
The above-mentioned 2 phases led to the Implementation phase, started in January 2009. This phase brought the development of protocols, standardization of definitions, improved communication among the different teams, recruitment of more MFM specialists, and the initiation of an MFM fellowship. Among the new protocols implemented, there were induction of labor, diabetic ketoacidosis, and poorly controlled diabetic patient management; timing of delivery for the intrauterine growth restriction fetus; dating of the gestational age for pregnant women presenting later in the third trimester; and a blood bank protocol. With the latter protocol, in case of an emergency, a maternal blood transfusion must begin between 5 and 10 minutes from the time the blood is requested for transfusion.
The rounds on L&D increased from 2 to 10 in each 24-hour period. The directors of MFM and neonatology started to meet on a daily basis to improve the communication between the 2 teams. They standardized the neonatal thermal support and resuscitation including surfactant administration. They also emphasized the importance of administration of steroids in pregnancies at risk of prematurity.
Multidisciplinary meetings started to occur frequently to manage difficult obstetrical cases. The MFM team increased from 2 full-time faculty, 1 part-time faculty, and no fellows to 6 full-time faculty and 3 fellows. The MFM faculty coverage as the primary attending for L&D from 7:30
After 2008, a series of mandatory trainings began for all personnel rotating or working in L&D, including simulation training, currently called OB-FAST (Obstetric Feasible Approach Safety Training), and fetal heart rate monitoring training.
A large emphasis has been given to education. There is a mandatory didactic time for all residents. During this time, the residents do not have any clinical responsibility. Our program has also recruited a patient safety nurse who facilitates quality assurance in L&D.
Central Outcome Measures
Our primary outcomes included the infant mortality and the composite infant morbidity and mortality in VLBW infants delivered from 2004 through 2015. Infant mortality was defined as a death during initial hospital stay. The composite infant morbidity was defined as presence of any one or more of the following during the hospital stay: intraventricular hemorrhage, chronic lung disease, necrotizing enterocolitis, pneumothorax, any late infection, and periventricular leukomalacia.12-14
Statistical Analyses
Our center has reported data on VLBW infants to VON since 1999. For this study, we compared 2 groups of VLBW infants born at ROH: those born between 2004 and 2008 (Pre-Implementation) and those born from 2009 to 2015 (Post-Implementation). The rationale for this pre and post time-period division was that we started a new perinatal program in 2008.
Standardized, risk-adjusted mortality and combined mortality-morbidity ratios (SMR) were reported from VON as the number of observed to expected cases. The SMR and the lower and upper bounds of the 95% confidence interval are based on a multivariable adjustment model, which considers the case mix of our center compared with all other centers. The following factors are taken into consideration for calculating the SMR: gestational age, small for gestational age, indicator measures that identify whether the infant had a birth defect (and if so, the severity of the defect), multiple births, Apgar score at 1 minute, infant sex, maternal race, vaginal delivery, and birth location. For this study, a best estimate of gestational age in weeks and days was based on the following hierarchy, as established by VON: obstetrical measures based on last menstrual period, obstetrical parameters, prenatal ultrasound as recorded in the maternal chart or neonatologist’s estimate based on physical criteria, neurological examination, and combined physical and gestational age exam (Ballard or Dubowitz exam).
The SMR and its confidence interval indicate whether our center has more or fewer infants with the outcome than would be expected, based on the characteristics of infants treated in our center. An SMR upper bound less than 1 indicates that our center had fewer than expected infants with the outcome. An SMR lower bound greater than 1 indicates that our center had more than expected infants with the outcome. A lower and upper bound including 1 indicates that the number of infants with the outcome was not significantly statistically different from the number expected after adjusting for the characteristics of infants treated. Other parameters not included in the calculation of the SMR are reported in Table 2.
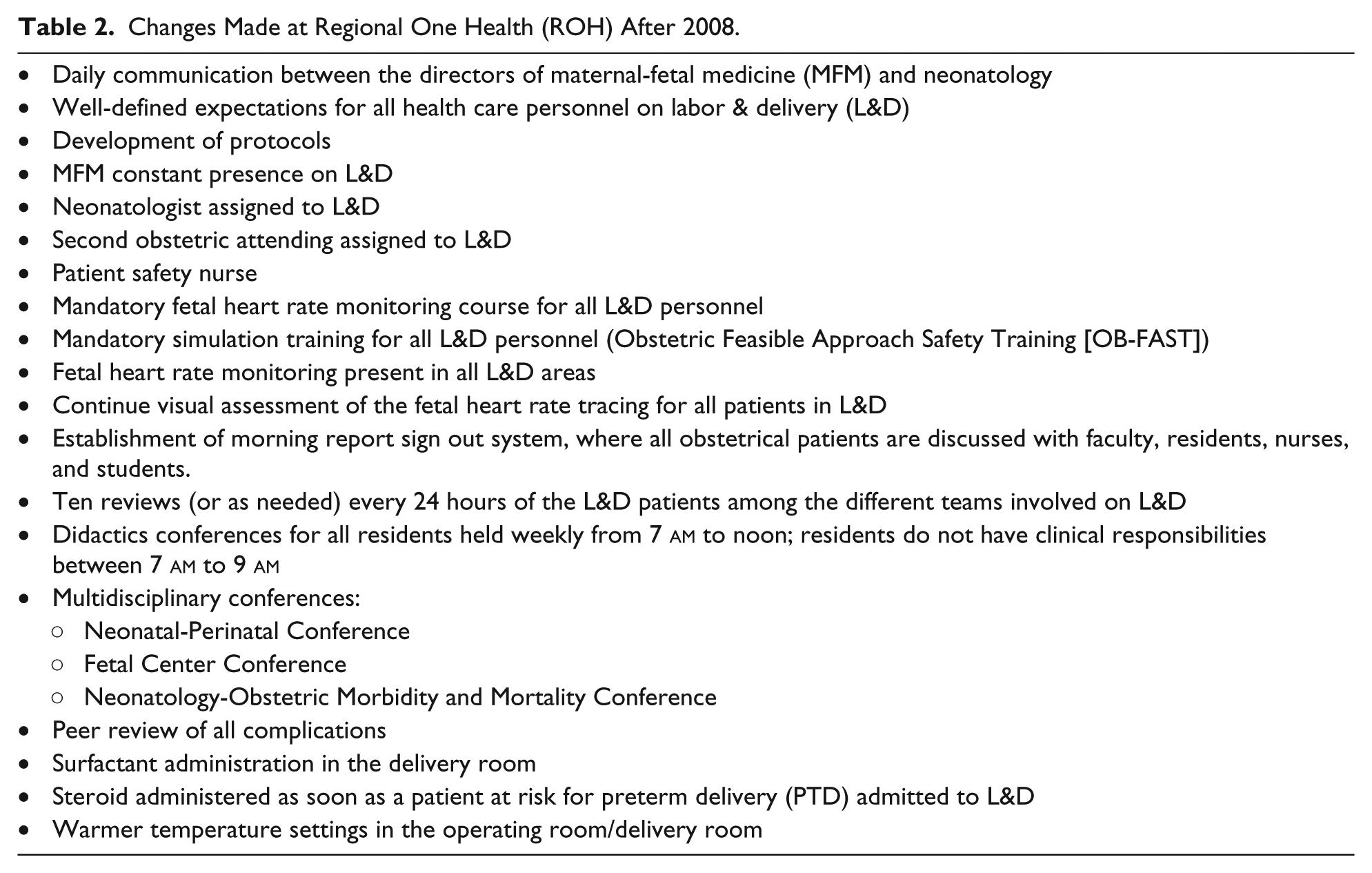
Changes Made at Regional One Health (ROH) After 2008.
The χ2 test was used to compare the equality of proportions, while a 2-sample t test was used to compare the equality of means between the 2 defined time periods, respectively. Trends in infant mortality and composite mortality-morbidity outcome over the entire time frame were tested using a Cochran-Armitage test for trend. Furthermore, infant mortality and composite mortality-morbidity rates over the years were compared using the logistic regression model. Within the same model, we tested the clinical variables associated with a decrease in mortality and composite morbidity-mortality rates over time. We present a reduced parsimonious model results, therefore variables that were tested but not found significant were not included in the final model.
Variables tested included those related to the mother, such as prenatal care, ethnicity, and prior or multiple births; those related to comorbidities, such as pneumothorax or birth defects; medical procedures at any time during the hospital stay, such as surfactant use and taking the infant’s temperature during the first hour after delivery; and procedures in the delivery room including use of epinephrine, endotracheal tube vent, delivery of oxygen, and face mask ventilator. We estimated the relative odds of the outcome measures to describe the magnitude of risk change, over time as well as in association with the model covariates. All of our analyses were performed using SAS/STATv14.1, and the associations were considered significant at the α level of .05 with trends reported at .1.
Results
Though the clinical data collection started in 2004, the process of observation and implementation after 2008 became continuous and ongoing; changes continue to be made when we observe opportunities for improvement. From 2004 through 2015, ROH documented 52 298 deliveries; 2364 were VLBW infants who were premature and were admitted to the NICU.
The main changes that occurred in the perinatal program are summarized in Table 2. The primary clinical characteristics and differences between the 2 periods are reported in Table 3. Figure 1a-d shows trends over time in clinical measures, proportion of cesarean deliveries, temperature at admission, administration of antenatal steroids and surfactant. From the Pre-Implementation to Post-Implementation time frame, the proportion of cesarean deliveries increased significantly (62.2% to 69.4%; P = .0002). Temperature at admission was not collected in 2004 and 2005. The number of neonates admitted with temperature <36°C decreased from the Pre- to Post-Implementation period (55.2% to 11.8%; P < .0001). The percentage of low-temperature admissions was at its highest peak in 2006 at 59.4%; it dropped to 40.2% in 2009 and sharply to 13.3% in 2010, all the way down to 0.6% in 2015. The administration of antenatal steroids (76.2% to 89.1%; P < .0001) and surfactant administration in the delivery room (17.9% and 49.0%; P < .0001) both increased after 2008, respectively.
Main Characteristics of the Study Population.
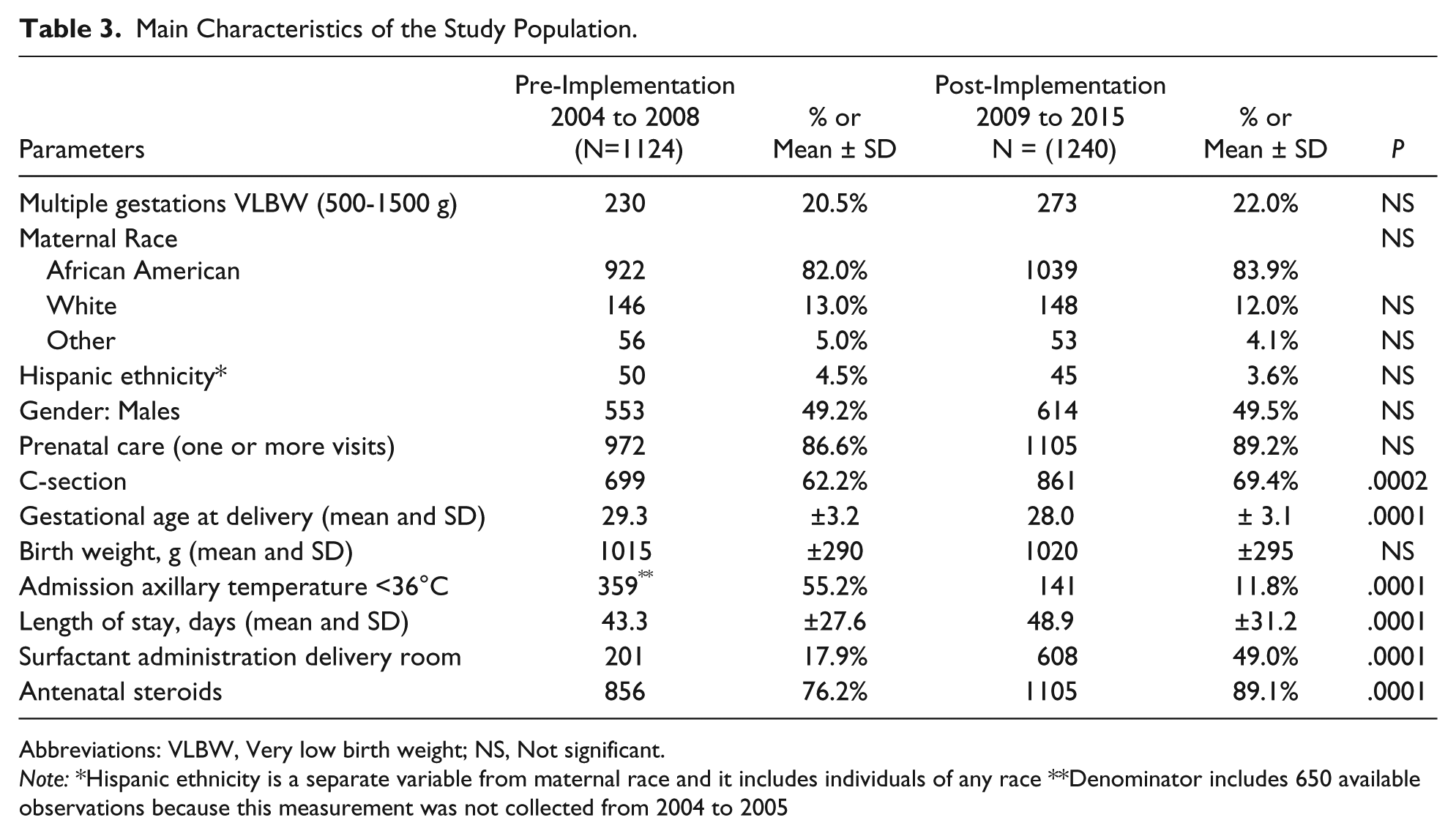
Abbreviations: VLBW, Very low birth weight; NS, Not significant.
Note: *Hispanic ethnicity is a separate variable from maternal race and it includes individuals of any race **Denominator includes 650 available observations because this measurement was not collected from 2004 to 2005
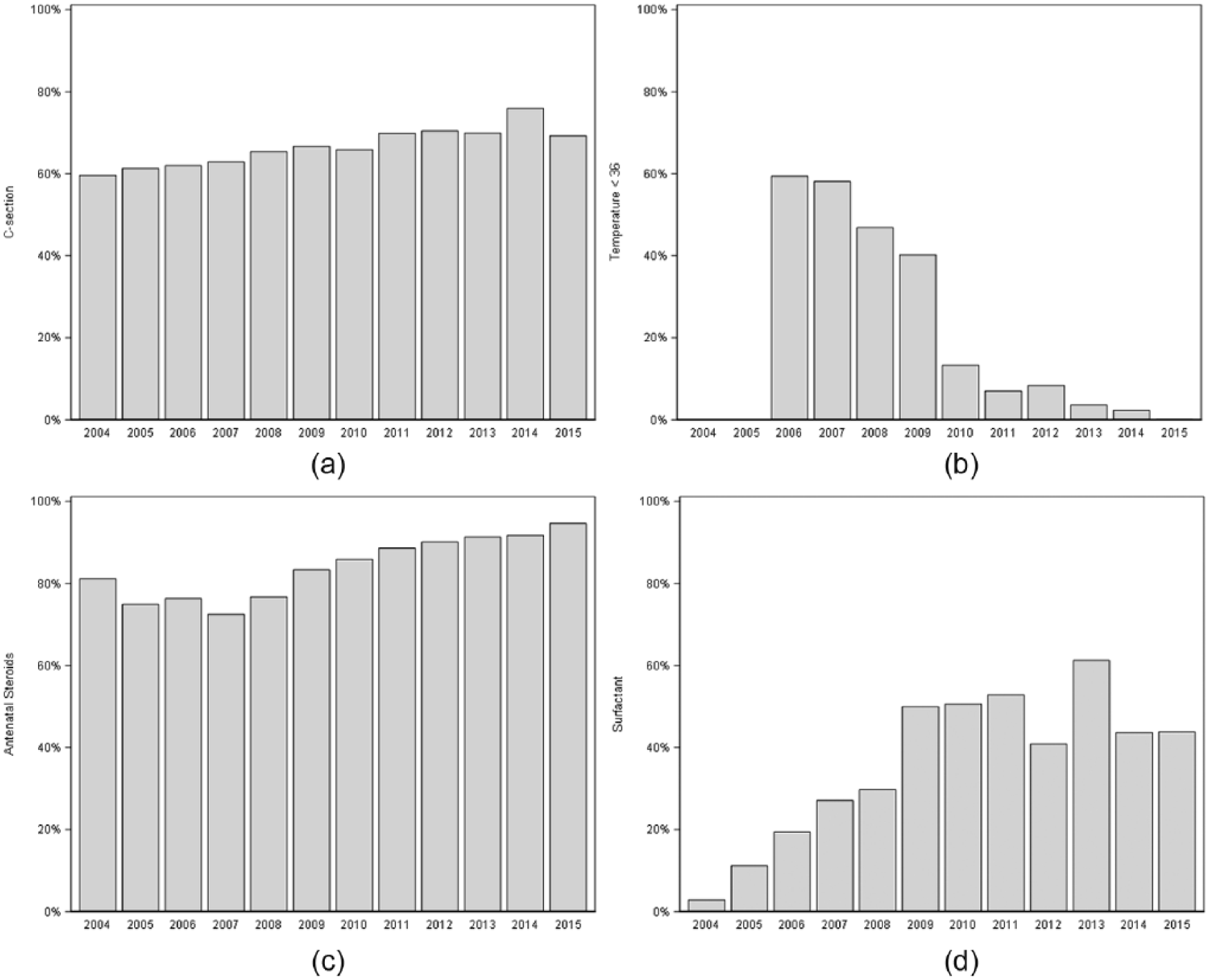
(a) Cesarean deliveries, percentages by year, 2004 to 2015. (b) Low temperature at admissions, less than 36°C; percentages by year, 2006 to 2015. (c) Antenatal steroid use, percentages by year, 2004 to 2015. (d) Surfactant administration in the delivery room, percentages by year, 2004 to 2015.
The IMR and the composite morbidity and mortality rate for the Pre-Implementation and Post-Implementation periods are presented in Table 4. The IMR decreased from 15.5% during Pre-Implementation to 13.1% during Post-Implementation (P = .0933). A test for linear trend over time was borderline significant for infant mortality (P = .0989). The highest rate was observed in 2008 at 16.8%, and the lowest in 2014 at 12%. The composite morbidity and mortality rate significantly decreased from 55.7% to 43.9% (P < .0001) during the same time frame. The linear trend suggests a highly significant decline over time (P < .0001), from the highest rate in 2004 at 61.0% to the lowest in 2014 at 36.8%. Trend comparison over time shows that from 2009 to 2015 odds of infant morbidity-mortality rates decreased as much as 50% or even more relative to 2004 (Figure 2). The percentage of infants who survived and suffered none of the specified morbidities increased from 44.3% in Pre-Implementation to 56.1% in Post-Implementation (P < .0001).
Unadjusted Infant Mortality and Composite Neonatal Outcome (Morbidity + Mortality) rates and odds ratios.

Abbreviations: OR, odds ratio; CI, confidence interval.

Comparison of composite infant morbidity-mortality rates of subsequent years to that in 2004, with confidence intervals. Odds ratios below 1 indicate reduction in odds of infant morbidity-mortality.
The SMR is presented with smoothed 3-year average data. The composite outcome for VLBW infants was 20% above the expected value for the years averaged from 2004 through 2006. The observed value decreased gradually, eventually falling to 20% below the expected value beginning in 2009 to 2011 (P < .0001; Figure 3).

Standard risk adjusted for mortality and composite morbidity ratio (SMR). The dots represent the mean; the bars represent the 95% confidence interval. The number 1 represents the expected mortality and composite morbidity as determined by the Vermont Oxford Network (VON) for our center. The SMR is calculated using a 3-year average.
Multivariate models support several of the univariate findings. Looking at the 2 time frames alone, there was an 18% reduction in odds of infant mortality from the Pre- to the Post-Implementation period though it did not reach traditional statistical significance (odds ratio [OR] = 0.82; 95% confidence interval [CI] = 0.65-1.03; P = .0933; Table 4). After the adjustment for several clinical factors explaining that trend variables strongly associated with a decrease in infant mortality over time include increase in administration of antenatal steroids (OR = 0.48; 95% CI = 0.34-0.67; P < .0001) and cesarean delivery (OR = 0.62; 95% CI = 0.46-0.82; P = .0009), with surfactant at the time of delivery being borderline (OR = 0.78; 95% CI = 0.56-1.07; P = .1244), while controlling for birth weight, child sex, and Apgar score (Figure 4). Ten grams increase in birth weight was associated with 3% decline in odds of mortality (OR = 0.97; 95% CI = 0.96-0.98; P <.0001). Similarly, for the composite morbidity-mortality outcome measure, there was a 38% reduction in odds of morbidity-mortality from the Pre- to the Post-Implementation period (OR = 0.62; 95% CI = 0.53-0.73; P < .0001; Table 4). Even after the adjustment for clinical and demographic covariates, the Post-Implementation period was associated with a significant decrease in odds of composite morbidity-mortality (OR = 0.57; 95% CI = 0.46-0.71; P < .0001). As with mortality alone, variables strongly associated with a decrease in infant morbidity-mortality over time include increase in administration of antenatal steroids (OR = 0.59; 95% CI = 0.44-0.79; P = .0003) and cesarean delivery (OR = 0.49; 95% CI = 0.39-0.61; P < .0001), while controlling for birth weights, child sex, and Apgar score. Surfactant at the time of delivery showed a borderline association (OR = 0.79; 95% CI = 0.62-1.01; P = .0632; Figure 5). Similarly, 10 g increase in birth weight was associated with 4% decline in odds of composite morbidity-mortality (OR = 0.96; 95% CI = 0.96-0.97; P < .0001).

Multivariate logistic regression model showing the association between the covariates of interest and infant mortality over time, with 95% confidence intervals.

Multivariate logistic regression model showing the association between the covariates of interest and composite infant morbidity-mortality over time, with 95% confidence intervals.
Discussion
Main Findings
We observed significant changes in the composite morbidity-mortality for VLBW infants between the 2 periods analyzed in this study. The standardized mortality and morbidity rate for VLBW infants was consistently 20% above the expected value during Pre-Implementation. This rate improved to up to 20% below the expected value in the time period beginning 2009 to 2011, Post-Implementation. Among others, factors associated with these changes include increase in administration of antenatal steroids, cesarean delivery, and perhaps surfactant at the time of delivery.
We targeted our study on the outcomes of VLBW infants for 2 main reasons. These infants are 200 times more likely to die than are full-term infants, and 84% of infant deaths in this group occur during the neonatal period. 5 It is for this group of infants that both the obstetrician and neonatologist play a fundamental role for survival, more than at any other gestational age. The obstetrician should minimize the risk for the fetus, and the neonatologist should have experience in managing VLBW infants. Therefore, the results of a program that starts when the baby is still in utero may be more easily measured in the neonatal period by using the outcome of VLBW infants. The second reason is that ROH is the hospital with the highest number of VLBW infants born in Shelby County. We did not include infants with a birth weight of less than 500 g, because reporting data on those infants may be incomplete and misleading. 15
The composite morbidity-mortality outcome for VLBW infants that we observed in our hospital decreased disproportionately when compared with that observed in many centers participating in VON. If the composite morbidity-mortality rate in our hospital decreased similarly to that of other hospitals in the network, the risk would have remained 20% above the expected rate. The evidence that the rate went from 20% above the expected to 20% below the expected in a few years indicates that the composite morbidity-mortality for VLBW infants in our hospital decreased more than in many other hospitals across the network.
Many factors have played a role in the results that we observed in our hospital. Supported by our data, the increased number of VLBW infants who received both steroids before delivery and surfactant soon after delivery, and the increase in the proportion of cesarean sections contributed significantly to lower morbidity and mortality. Observational studies suggest an improved outcome with the use of cesarean delivery, which is consistent with our findings. 16
The number of infants who were admitted with a temperature below 36°C significantly decreased over time, all the way down to 0.6% in 2015; however, this was not significantly associated with either outcome in our models.
Proportion of multiple gestations in Post-Implementation did not increase significantly. Whether mortality is higher in twin gestations than in singletons is controversial. Some studies show that there is a difference in mortality between twins and singletons that changes with gestational age; our models, however, suggest no association.17,18
We speculate that the following changes might have had additional effects on the outcome improvements, though these are purely observational: (1) improved communication both inside the Department of Obstetrics and Gynecology and with the neonatology team; (2) changes that occurred in the NICU; (3) the development of protocols for specific situations; (4) the emphasis given to our simulation program; (5) the recruitment of a patient safety nurse; (6) the clear expectations for, and accountability from, the staff and doctors both in clinics and on L&D; (7) the changes made in the MFM program with the recruitment of more MFM specialists; (8) and starting an MFM fellowship. This is supported by our morbidity-mortality model results that indicate that there are other factors unaccounted for, that further explain the variability in the outcome rates over time.
The results observed in our hospital have contributed to the decrease of the IMR in Shelby County. Thirty percent of all Shelby County infants and 65% of VLBW infants were delivered at ROH from 2004 through 2015. The IMR of the county decreased from 12.8 per 1000 in 2004 to 8.2 per 1000 in 2015. This decreased mortality is primarily due to a decreased neonatal mortality. Although post-neonatal mortality decreased during this period as well, the changes were not statistically significant.8,19,20
Strengths and Limitations
The strength of our study is that the data were obtained from our own database. We have a dedicated team that works exclusively for the database in perinatology. This has the advantage over data obtained from birth certificates, in which some information is not reported. Our models allow for establishing whether one change was more important than another relative to the magnitude of the effect.
There are some limitations to our study. Eligibility was restricted to infants with a birth weight of 500 to 1500 g. Thus, our inferences are limited to infants in that weight range. We did not define or stratify our study population based on gestational age, because, before 2006, eligibility for the VON database was based on only birth weight. We do control for the birth weight in our models, which is a correlate of gestational age. This study does not have a control group, and some may suggest changes are part of similar temporal trends across the board. The VON standardized rates presented here, however, suggest 20% decrease in outcome measures below the network average.
Conclusion
The program we implemented did not require a large economic investment. We believe the phases of our plan can be disseminated and implemented by other centers with similar issues by delineating a strategic plan. Probably the most crucial aspects for starting a program such as the one here reported are (1) continuous communication among the Division of Neonatology, the Department of Obstetrics and Gynecology, and all other divisions and departments involved with the care of the patients; (2) the standardization of procedures; (3) including physicians and nurses in decision-making with the support of administrators; and, most important, (4) creating an effective team atmosphere.
Footnotes
Acknowledgements
We are grateful to colleagues, fellows, residents, nurses, all personnel in obstetrics/gynecology, neonatology, and to the UTHSC and ROH assistants and administration who have made this project possible. We also wish to acknowledge the State of Tennessee’s Perinatal Grant for partial funding of this project.
Authors’ Note
The State of Tennessee had no role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; nor in the decision to submit the article for publication. No honorarium, grant, or other form of payment was given to anyone to produce the article.
Author Contributions
GM: Contributed to conception and design; contributed to acquisition and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ZB: Contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
PJG: Contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RD: Contributed to conception and design; contributed to acquisition and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Part of this project was supported by the Perinatal Grant, State of Tennessee. No funding was received from any pharmaceutical or other for-profit agency.
Ethical Approval
The University of Tennessee Health Science Center (UTHSC) Institutional Review Board (IRB) approved this study as 14-03205-XP on July 30, 2014.