
Abstract
Objective
This retrospective cohort study aimed to identify perinatal factors associated with umbilical arterial pH in term neonates delivered via cesarean section, using a pH cutoff of 7.20 to define neonatal acidosis.
Methods
We analyzed clinical data from 356 mother–neonate dyads who underwent cesarean delivery at a tertiary hospital between January 2020 and December 2022. Neonates were categorized into two groups based on umbilical arterial pH values (<7.20 vs. ≥7.20). We evaluated maternal and intrapartum factors, including amniotic fluid quality (operationally defined as clear or meconium-stained (grades I–III)), duration of labor, and fetal distress. Statistical analyses included multivariable logistic regression to quantify associations (reported as odds ratios with 95% confidence intervals) and random forest modeling to identify key predictors. Model performance was assessed via receiver operating characteristic curve analysis.
Results
The incidence of acidosis (umbilical arterial pH <7.20) was 51.0% (52/102). Meconium-stained amniotic fluid (adjusted odds ratio: 3.12; 95% confidence interval: 1.75–5.58; p < 0.001) and trial of labor (adjusted odds ratio: 2.45; 95% confidence interval: 1.40–4.30; p = 0.002) were significantly associated with acidosis. The random forest model identified these factors as the top predictors, with an area under the curve of 0.71 (95% confidence interval: 0.68–0.74) based on 10-fold cross-validation.
Conclusion
Meconium-stained amniotic fluid and prolonged labor are strongly associated with acidosis in term cesarean deliveries. Early identification of these factors may aid in risk stratification and perinatal management.
Keywords
Introduction
Umbilical arterial (UA) blood gas analysis is a cornerstone of modern perinatal care, providing an objective measure of fetal metabolic status and oxygenation at the time of birth. First described by James et al. in 1958 as a method to detect intrapartum hypoxia, its clinical value was later formally recognized by the American College of Obstetricians and Gynecologists (ACOG) and detailed in expert consensus guidelines, such as those from the Chinese Perinatal Medicine Society.1,2 For the term neonate, UA pH is a particularly sensitive indicator of the intrauterine environment; deviations from the normal range (typically 7.20–7.20) are strongly associated with fetal distress, neonatal asphyxia, and an increased risk of adverse neurodevelopmental outcomes. 3 The physiological basis for this lies in the unique nature of fetal circulation, where the placenta is the organ of gas exchange. The umbilical artery carries deoxygenated blood and metabolic waste products from the fetus back to the placenta, making its pH a direct reflection of fetal acid–base balance. Compensatory mechanisms can buffer brief episodes of hypoxia, but prolonged oxygen deprivation leads to anaerobic metabolism, lactic acidosis, and a precipitous drop in pH, potentially causing irreversible organ damage. 3
Despite its proven prognostic significance, universal access to immediate UA blood gas analysis remains inconsistent across healthcare settings. This practical limitation underscores the critical need to identify reliable prenatal and intrapartum factors that can predict neonates at the highest risk of acidosis, thereby enabling targeted testing and intervention. Previous research has identified several potential predictors of low UA pH, including nonreassuring fetal heart patterns, meconium-stained amniotic fluid, and the duration of active labor.1–3 However, the existing body of evidence is often derived from mixed populations, including vaginal deliveries, and studies focusing specifically on term neonates delivered via cesarean section are less comprehensive. Furthermore, there is a lack of consensus on the relative importance of these factors and a paucity of studies utilizing advanced predictive modeling to quantify their combined predictive power.
This study aimed to address these gaps by conducting a focused investigation on a well-defined cohort of term neonates delivered via cesarean section. We seek to synthesize and evaluate a comprehensive set of maternal, fetal, and intrapartum variables to determine their independent association with UA pH. By employing both traditional multivariable regression and a machine learning approach (random forest (RF) modeling), we intend to not only identify key predictors but also develop a robust predictive model. The ultimate goal is to provide clinicians with an evidence-based framework for risk stratification, facilitating the timely identification of neonates who would most benefit from mandatory UA blood gas analysis and subsequent tailored perinatal management.
Materials and methods
Study design and setting
This retrospective cohort study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The study was conducted at the Department of Obstetrics and Gynecology, Nanjing First Hospital, affiliated with Nanjing Medical University.
Study aims
The primary aim of this study was to identify perinatal factors associated with UA pH in term neonates delivered via cesarean section.
Eligibility criteria
Inclusion criteria included singleton neonates with a gestational age ≥37 weeks delivered via cesarean section between July 2023 and July 2024.
The exclusion criteria included multiple pregnancies (twins or higher-order multiples), major fetal congenital anomalies, and incomplete medical records. After applying these criteria, 102 mother–infant pairs met the study requirements. The indications for cesarean section are shown in Figure 1.

Indications for cesarean section among 102 study participants.
Data collection
The trained research staff extracted data from electronic medical records using a standardized form. Collected variables included the following:
Maternal characteristics. Age, height, weight, gestational weight gain, prepregnancy body mass index (BMI), BMI at delivery, parity, and gestational age at delivery;
Prenatal factors.
○ Maternal factors. Age ≥35 or ≤18 years, prepregnancy BMI >25 or <18.5 kg/m2, uterine scarring, and obstetric complications including gestational hypertension, intrahepatic cholestasis of pregnancy, heart disease, gestational diabetes mellitus (GDM), anemia, and thrombocytopenia; ○ Fetal factors. Intrauterine fetal distress, fetal growth restriction, macrosomia, low birth weight at term, and abnormal fetal position; ○ Other factors. Elevated systolic/diastolic (S/D) ratio of the umbilical artery, abnormal amniotic fluid volume, umbilical cord abnormalities, premature rupture of membranes (PROM), and acute/chronic chorioamnionitis. Intrapartum management. Trial of labor, use of balloon catheter for induction, and anesthesia type (spinal or general); Neonatal outcomes. Sex, gestational age, weight, length, 1- and 5-min Apgar scores, amniotic fluid characteristics, and UA blood gas analysis values.
UA blood was sampled immediately after delivery using a standardized protocol. A segment of the umbilical cord approximately 15 cm from the placenta was double-clamped before cutting. A 1.0-mL sample was drawn from the umbilical artery using a blood gas needle and analyzed within 10 min using a GEM Premier 3000 blood gas analyzer. Measured parameters included pH, partial pressure of oxygen (PaO2), partial pressure of carbon dioxide (PaCO2), lactate, bicarbonate (
The reporting of this study conforms to the STROBE guidelines. 4 Diagnostic criteria for maternal and fetal conditions were based on the ACOG guidelines.
Operational definitions for key intrapartum outcomes were as follows:
Trial of labor. Defined as the onset of regular, painful uterine contractions (at least three contractions within 10 min) accompanied by cervical dilation of ≥3 cm and effacement of ≥50%, which subsequently ended in a cesarean delivery. Fetal distress. Diagnosed based on the presence of a nonreassuring fetal heart rate (FHR) pattern on continuous cardiotocography (CTG). This included persistent fetal bradycardia (FHR <110 bpm), recurrent late decelerations, prolonged decelerations, or a nonreassuring pattern (e.g. minimal variability with recurrent decelerations) that prompted the obstetrician’s decision to perform a cesarean section for fetal indications.
Statistical analysis
Neonates were categorized into two groups based on UA pH values: <7.20 (acidosis) and ≥7.20 (normal), consistent with widely accepted clinical thresholds.
Continuous variables with a normal distribution were expressed as mean ± SD and compared using independent sample t-tests. Non-normally distributed variables were presented as median with interquartile range and compared using Mann–Whitney U tests. Categorical variables were expressed as frequency and percentage, and group differences were assessed using the chi-squared test or Fisher’s exact test, as appropriate.
Variables with p < 0.2 in univariate analyses were included in a multivariable logistic regression model to identify factors independently associated with UA pH <7.20. Results were reported as adjusted odds ratios (ORs) with 95% confidence intervals (CIs).
An RF model was developed to identify key predictors of low UA pH. The model was trained using 10-fold cross-validation, with hyperparameters set as mtry = 3 and ntree = 500, tuned via out-of-bag error estimation. Variable importance was assessed based on the mean decrease in the Gini index. Model performance was evaluated using the area under the receiver operating characteristic curve (ROC AUC).
All statistical analyses were performed using SPSS version 26.0 (IBM Corp., USA) and R software version 4.1.2 (R Foundation for Statistical Computing, Austria) with the ‘randomForest’ package. A two-sided p-value <0.05 was considered statistically significant.
Results
Maternal clinical data analysis
A total of 102 participants were included in this study and categorized into two groups based on UA blood pH values: pH < 7.20 group (n = 52) and pH ≥ 7.20 group (n = 50). Comparative analysis of baseline characteristics showed no statistically significant differences between the two groups in terms of maternal age, height, weight, gestational weight gain, prepregnancy BMI, or BMI at delivery (all p > 0.05), indicating that the groups were well-balanced and comparable (Table 1).
Analysis of maternal characteristics.

BMI: body mass index.
A comparison of pregnancy outcomes and complications between the two groups is presented in Table 2. The incidence of PROM was significantly higher in the pH < 7.20 group (21.2%) than in the pH ≥ 7.20 group (6.0%) (p < 0.05). No statistically significant differences were observed between the two groups in terms of gestational age at delivery, parity, or the prevalence of gestational hypertension, GDM, anemia, thyroid disease, or abnormal amniotic fluid volume (all p > 0.05) (Table 2).
Analysis of pregnancy characteristics in both groups.

PROM: premature rupture of membranes.
Neonatal clinical data analysis
Comparisons of neonatal outcomes are presented in Table 3. The incidence of fetal distress (38.5% vs. 8.0%) and the overall rate of amniotic fluid pollution (30.8% vs. 8.0%) were significantly higher in the pH < 7.20 group than in the pH ≥ 7.20 group (all p < 0.05). Notably, a higher proportion of grade III amniotic fluid pollution was observed in the pH < 7.20 group (17.3% vs. 0%). No statistically significant differences were found between the two groups in terms of neonatal weight, length, sex, incidence of macrosomia, or umbilical cord abnormalities (all p > 0.05) (Table 3).
Analysis of neonatal clinical data.

Impact of intrapartum management on UA blood pH
A comparison of delivery interventions between the two groups is presented in Table 4. The probability of undergoing a trial of labor was significantly higher in the pH < 7.20 group (50.0%) than in the pH ≥ 7.20 group (16.0%) (p < 0.05). No statistically significant differences were observed between the two groups regarding the use of balloon catheters for induction or the choice of anesthesia (spinal or general) during cesarean section (all p > 0.05) (Table 4).
Analysis of intrapartum management factors in both groups.

Analysis of neonatal assessment indicators
Comparisons of neonatal assessment indicators are presented in Table 5. UA blood gas analysis revealed that the pH < 7.20 group had significantly lower PaO2 and significantly higher PaCO2 and lactate levels than the pH ≥ 7.20 group (all p < 0.05). No statistically significant differences were observed between the two groups in terms of 1-min Apgar score, 5-min Apgar score, BEecf, or
Analysis of neonatal assessment indicators.
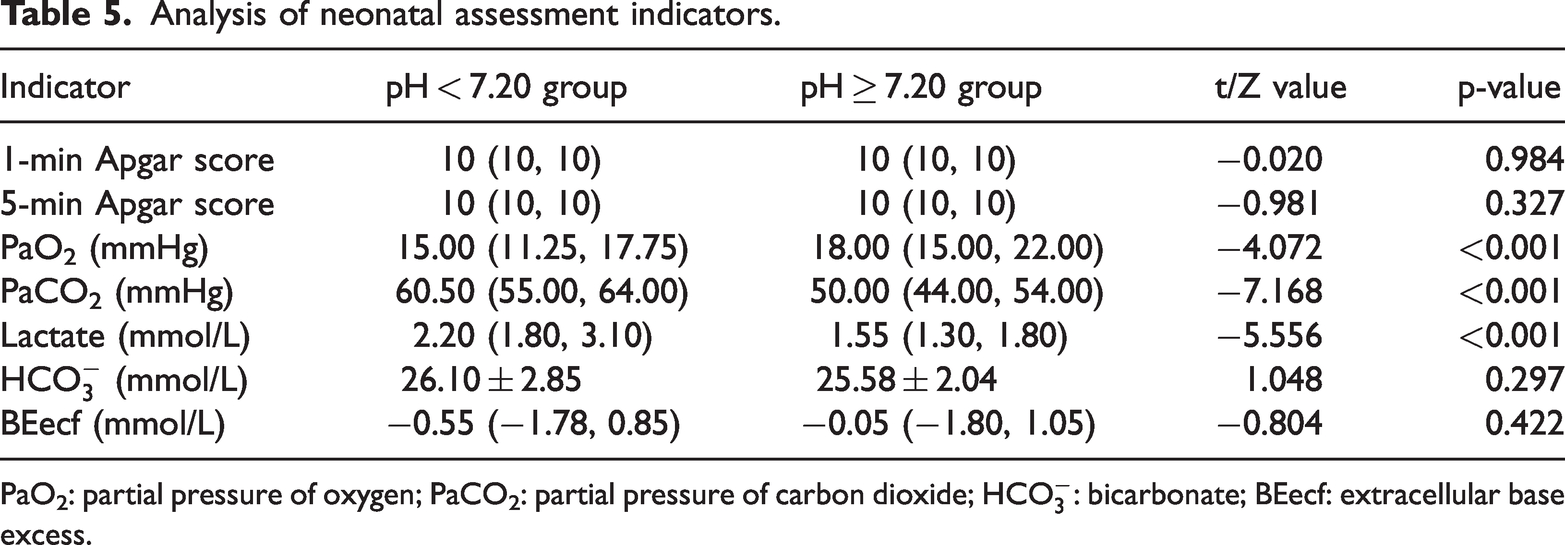
PaO2: partial pressure of oxygen; PaCO2: partial pressure of carbon dioxide;
Association analysis using Cramer’s V for predicting low pH risk
Figure 2 presents an assessment of the strength of association between various variables (e.g. PROM, trial of labor, amniotic fluid quality, and fetal distress) and pH grouping using Cramer’s V coefficient. Cramer’s V measures the strength of association between two categorical variables, ranging from 0 (weak association) to 1 (strong association).

Strength of association between variables and pH group.
The data in Figure 2 reveal that amniotic fluid quality and trial of labor have higher Cramer’s V values with pH grouping, indicating a stronger association with the risk of low pH. In contrast, PROM and fetal distress exhibit lower Cramer’s V values, suggesting a weaker association with pH grouping. This analysis supports the selection of amniotic fluid quality and trial of labor as key predictive variables in modeling low pH risk, potentially improving model performance (Figure 2).
Feature importance analysis in the RF model for predicting pH grouping
Figure 3 illustrates the feature importance within the RF model, which evaluates each variable’s contribution to predicting pH grouping (normal or low pH). Feature importance is determined by the reduction in impurity (e.g. Gini index or information gain) when a variable is used to split nodes in the model, with higher values indicating a stronger impact on model decisions.

Feature importance in random forest model.
In this analysis, amniotic fluid quality and trial of labor received the highest importance scores, indicating that these variables have substantial explanatory power in predicting low pH. The model’s reliance on these two variables for accurate predictions is evident, whereas fetal distress and PROM had lower feature importance, indicating limited influence on model decisions. These findings align with the results of the Cramer’s V analysis, further reinforcing the significance of amniotic fluid quality and trial of labor in predicting pH grouping. This visual analysis aids in identifying key variables that meaningfully contribute to the risk of low pH (Figure 3).
ROC curve analysis of the RF model for pH classification
Figure 4 presents the ROC curve analysis of the RF model for pH classification (normal vs. low pH). The curve illustrates the relationship between the true positive rate (sensitivity, y-axis) and false positive rate (1-specificity, x-axis) across various classification thresholds, evaluating the model’s discriminative performance. The solid blue line represents the model’s ROC curve, while the gray dashed line serves as a reference for random classification.

ROC curve for random forest model. ROC: receiver operating characteristic.
The model demonstrated stable discriminative performance across all classification thresholds, with an AUC of 0.71 (95% CI: 0.68–0.74), indicating moderate classification ability. At the optimal classification threshold, determined by Youden’s index, the model achieved a sensitivity of 0.72 and specificity of 0.65. These results indicate that the model maintains relatively high sensitivity while providing reasonable specificity (Figure 4).
Accuracy distribution of the RF model in 10-fold cross-validation
To comprehensively assess the model’s generalizability, a 10-fold cross-validation procedure was employed. The dataset was randomly partitioned into 10 mutually exclusive subsets, with 9 subsets used for training and the remaining subset for validation in each iteration, repeating this process 10 times.
During training, the model demonstrated strong learning capability, achieving a mean AUC of 0.87 ± 0.02. On the validation sets, the model’s consolidated performance metrics were as follows: mean AUC of 0.71 (95% CI: 0.68–0.74), mean sensitivity of 0.72, mean specificity of 0.65, and mean accuracy of 0.66 ± 0.04. The moderate discrepancy between training and validation performance indicates good generalizability without evidence of severe overfitting.
Figure 5 shows the accuracy distribution across the 10-fold cross-validation. Each blue data point represents the accuracy of a single validation fold, the red dashed line marks the overall mean accuracy (0.66), and the red shaded area indicates the 95% CI (0.56–0.75). This distribution demonstrates the model’s consistent performance across different data subsets, verifying the reliability of the model’s predictions (Figure 5).

Tenfold cross-validation accuracy for random forest model.
The ROC curve and its CIs in Figure 4 demonstrate the model’s significant and stable discriminative ability, while the cross-validation results in Figure 5 further confirm the consistency of this performance across different data subsets. The balance between sensitivity and specificity, along with relatively narrow CIs, indicates that the model possesses both good discriminative power and generalizability for pH classification, making it suitable for practical predictive applications. The model significantly outperformed random classification across all evaluation metrics, demonstrating its potential utility for clinical prediction.
Discussion
Summary of the key findings
This study employed an RF model to identify critical prenatal and intrapartum predictors of UA acid–base status in term neonates. The most influential factors associated with low pH were amniotic fluid quality and trial of labor, both demonstrating significant predictive importance. Other factors, including PROM and fetal distress, showed moderate associations. The model achieved an AUC of 0.71 (95% CI: 0.68–0.74) through 10-fold cross-validation, indicating fair discriminative ability for classifying neonates with acid–base imbalance.
These findings highlight the potential of machine learning approaches to uncover complex, nonlinear relationships between clinical factors and neonatal outcomes. By focusing on readily observable intrapartum variables, this study provides a framework for early risk assessment that may assist in clinical decision-making during perinatal management.
Comparison with existing literature
Our results align with those of previous studies emphasizing the prognostic value of amniotic fluid quality in predicting fetal acid–base status. Meconium-stained amniotic fluid, particularly higher-grade contamination, has been consistently associated with fetal hypoxia and subsequent acidosis, corroborating its role as an indicator of intrauterine compromise.5–7 Similarly, the association between trial of labor and impaired UA pH is supported by previous studies linking prolonged labor and uterine hypercontractility to reduced placental perfusion and fetal oxygen supply.8,9
However, our model assigned comparatively lower importance to PROM and fetal distress, which contrasts with several previous reports identifying these as strong independent risk factors for acidosis.10,11 This discrepancy may stem from differences in study population, outcome definition, or analytical approach. It is also possible that the influence of these factors is mediated through other variables captured in the model,12,13 such as amniotic fluid quality.
Notably, unlike some prior studies incorporating biochemical markers such as lactate or PaCO2, our model relied solely on pre- and intrapartum clinical variables. This design enhances clinical applicability during labor management but may omit pathophysiologically salient information, potentially explaining the model’s moderate performance compared with more comprehensive approaches.
Limitations
Several limitations should be considered when interpreting these results. First, the relatively small sample size (n = 102) limits statistical power and increases the risk of overfitting, despite the use of cross-validation. This may affect the stability and generalizability of the feature importance rankings. Second, the retrospective design introduces the possibility of unmeasured confounding due to variables not recorded in the dataset, such as type of anesthesia, exact duration of labor stages, or detailed contraction patterns. Third, the model’s discriminative capacity—although acceptable—remains modest (AUC = 0.71), indicating that substantial variation in UA pH is not captured by the included predictors. Finally, variable selection was constrained by clinical availability and may have omitted other influential factors, such as maternal BMI, comorbidities, or specific delivery interventions.
These limitations suggest that the current model should be viewed as exploratory rather than clinically definitive. Future prospective studies with larger, multi-center cohorts and expanded feature sets are needed to improve model performance and validate its generalizability.
Clinical implications and future directions
Despite these limitations, the model highlights clinically relevant factors that can be monitored in real time during labor. Amniotic fluid quality and progress of trial of labor—readily observable parameters—may help clinicians identify cases warranting intensified monitoring or early intervention. In particular, severe meconium staining or protracted labor should prompt heightened vigilance for fetal acidosis.14,15
Future research should aim to integrate more granular intrapartum data—such as CTG traces, contraction characteristics, and maternal metabolic parameters—into predictive modeling. Furthermore, combining machine learning with interpretable model forms may help bridge the gap between prediction and physiological explanation. Ultimately, such efforts could contribute to individualized labor management strategies aimed at reducing the incidence of neonatal acidosis.
Conclusion
This study analyzed the effects of factors such as PROM, trial of labor, amniotic fluid quality, and fetal distress on neonatal UA blood pH, identifying amniotic fluid quality and trial of labor as key predictors of low pH. Feature importance analysis from the RF model indicated that these variables could significantly impact fetal oxygen supply during labor, with extended trial of labor and amniotic fluid contamination notably associated with an increased risk of low pH. These findings provide scientific support for clinical practice, highlighting the need to focus on high-risk factors in perinatal management and mitigate the risk of neonatal acidosis through real-time monitoring and individualized intervention. Future research should explore dynamic factors within trial of labor to develop more precise predictive models, ultimately enhancing neonatal outcomes.
Footnotes
Acknowledgments
We would like to thank the medical staff of the Department of Obstetrics and Gynecology at Nanjing First Hospital for their assistance.
Author contributions
Linlin Tang and Jian Chen, as co-first authors, contributed equally to the study’s conceptualization, experimental design, data collection, data analysis, and manuscript preparation. Mingming Xu contributed to data analysis, provided technical support, and assisted with data interpretation and discussion of results. Yinan Wu took primary responsibility for technical support in the experiments and assisted in data collection for specific experimental tasks. Youdi Xu supported the development of experimental methods and helped revise the manuscript. Yaping Wang, as the corresponding author, guided and supervised the overall research direction, reviewed and approved the final manuscript for submission, and handled responses to peer review feedback.
Consent for publication
All authors consent to publication.
Data availability statement
The dataset is available from corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no competing interests.
Funding
This study was supported by the Jiangsu Maternal and Child Health Association Scientific Research Project (Grant No. FYX202215), titled “Predictive Value of Combined Serum NLRP3 and IL-1Ra Detection for Postpartum Transition to Type 2 Diabetes in Women with Gestational Diabetes Mellitus.” The grant also covered experimental costs and publication fees.
Institutional review board statement
This study was approved by the Institutional Review Board of Nanjing First Hospital.
Informed consent statement
Informed consent was obtained from all participating pregnant women.