
Abstract
Introduction
The aberrant right subclavian artery (ARSA) was first described by Hunauld in 1735, with the clinical symptom of the so-called “dysphagia lusoria” or “difficulty in swallowing due to a quirk of nature,” as described by David Bayford in 1787. 1 In Bayford’s words, the symptoms “may be called lusoria, from Lusus Naturae that gives rise to it.” 2 It is also known as arteria lusoria as suggested by Arkin. 3 ARSA is one of the most common intrathoracic vascular anomalies. The majority of ARSA involves the subclavian artery passing posterior to the esophagus and rarely, if ever, passing in front of the esophagus. 4 To our knowledge, this is the first case of ARSA with imaging correlation of a course anterior to the esophagus, interposing between the trachea and esophagus in a living patient. We discuss the available literature on epidemiology, embryology, diagnosis, and possible management of this rare vascular anomaly, in addition to the vascular anomalies associated with repair of esophageal atresia (EA) and tracheoesophageal fistula (TEF).
Case Report
A 13-year-old male with a past medical history of premature birth at 34 weeks estimated gestational age, asthma, seasonal allergic rhinitis, and repair of upper EA and distal TEF with primary anastomosis as a neonate consulted pediatric pulmonology for evaluation of recurrent pneumonia and chronic cough. The patient also has a history of failure to thrive with gastrostomy tube requirement and esophageal dilation twice prior to 4 years of age.
The patient’s cough is described as dry and honking, occurring up to 5 nights a week. He was treated with fluticasone-salmeterol for several years for his previous diagnosis of asthma, but had not used inhaled corticosteroids in the last year. There are 18documented episodes of treatments for pneumonia. Despite this history, he had not required prolonged hospitalization. A sweat chloride test was negative. Quantitative immunoglobulins including immunoglobulin E and quantitative T/B lymphocyte counts were normal. There is no family history of immunodeficiency or underlying genetic disorders.
The patient has a history of poor weight gain since birth, requiring gastrostomy tube placement and Nissen fundoplication twice early in life. He presented with dysphagia, difficulty swallowing solids more than liquids, and reports taking small bites, often coughing with meals. Bowel movements have been regular and there was no history of constipation or diarrhea.
Pulmonary function testing showed a mixed restrictive and obstructive lung disease pattern. An upper gastrointestinal study demonstrated persistent distension in the proximal and mid-esophagus with supine positioning, with smooth tapering. This raised concern for external compression of the mid-esophagus (Figure 1). Flexible bronchoscopy showed a normal tracheal anatomical contour, as well as a blind mucosal pouch from previous TEF repair. Prominent pulsations were observed on both the anterior mid-tracheal wall and on the posterior tracheal wall.
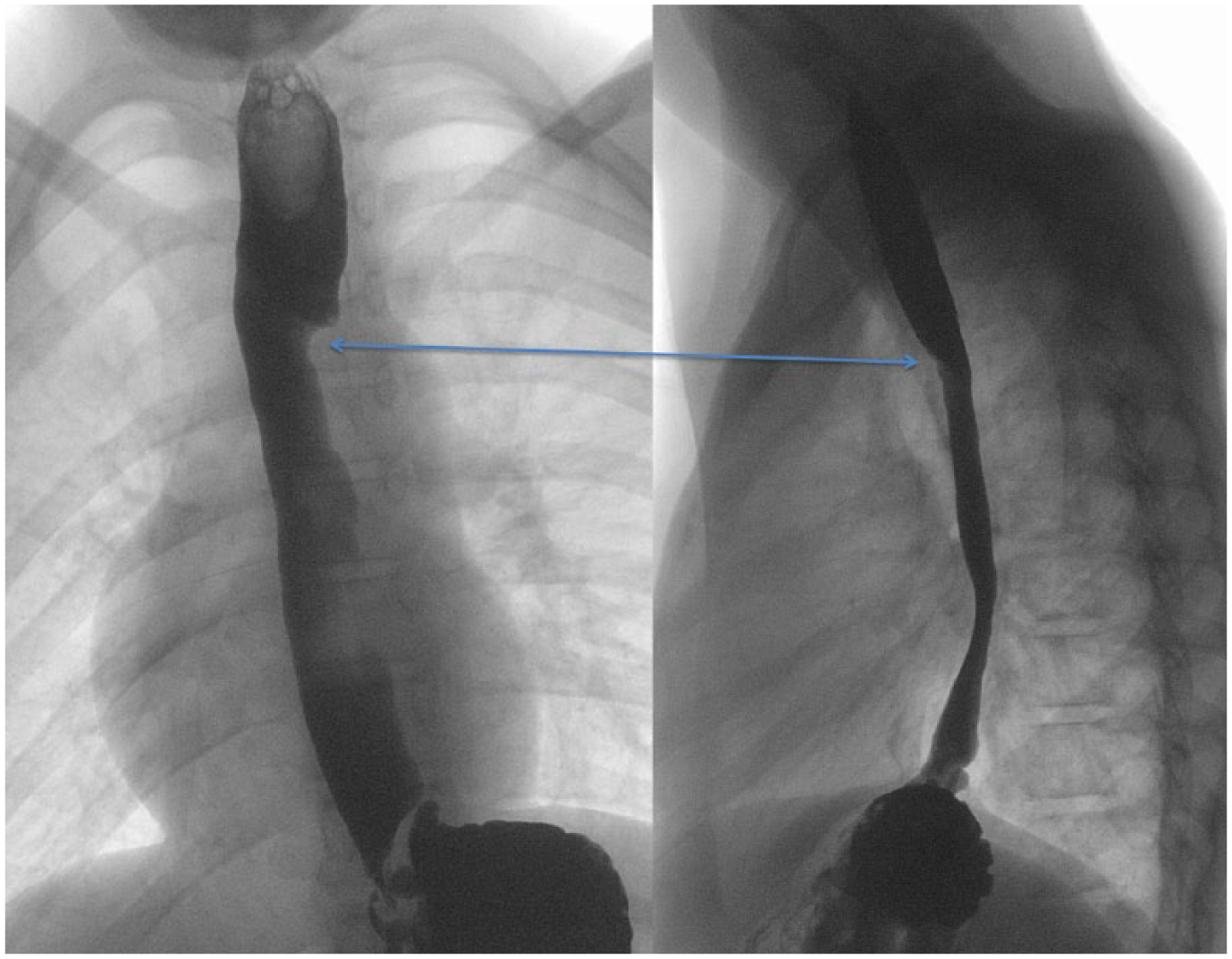
Upper gastrointestinal series fluoroscopy of a 13-year-old patient with persistent cough and multiple previous episodes of pneumonia. The anteroposterior view demonstrates a smooth indentation of the left wall of the esophagus. The lateral view confirms the indentation, which now appears to be compressing the anterior wall of the esophagus. The upper third of the esophagus is dilated, which is most apparent on the lateral view. The smooth indentation is marked by a blue double-sided arrow.
Chest computed tomography (CT) with intravenous contrast confirmed a left-sided aortic arch with an ARSA passing atypically between the trachea and the esophagus, causing flattening of the posterior tracheal contour and mass effect on the anterior esophagus (Figures 2 and 3).
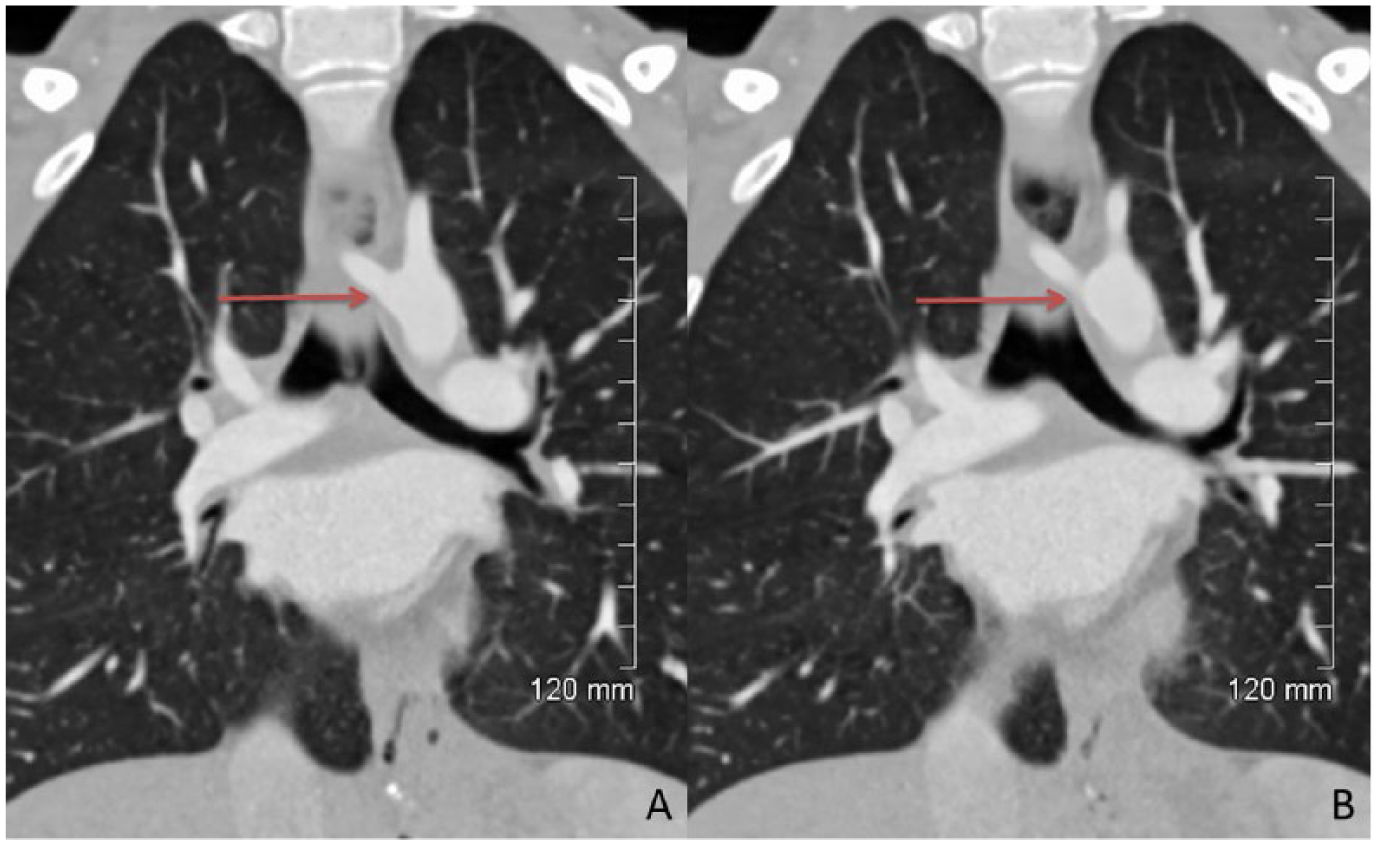
Follow-up computed tomography with intravenous contrast of the same patient with persistent cough and multiple previous episodes of pneumonia. Two consecutive coronal reformatted images of the chest at the level of the carina showing the origin of the retrotracheal aberrant right subclavian artery (red arrows).

Follow-up computed tomography with intravenous contrast of the same patient with persistent cough and multiple previous episodes of pneumonia. The axial and sagittal reformatted images (A and B, respectively) from the same imaging study as Figure 2 again demonstrates the rare retrotracheal course of the aberrant right subclavian artery (green and blue arrows in A and B, respectively). The aberrant right subclavian artery is seen interposed between the trachea (T) and the esophagus (E). Compression on the more malleable esophagus (E) is more readily apparent on the sagittal reformatted image (B).
Discussion
ARSA is one of the most common intrathoracic major arterial anomalies, with a reported incidence between 0.4% and 2% in the general population.4,5 According to Molz and Burri, 6 ARSA predominates in female patients, whereas aberrant left subclavian arteries predominate in male patients.
ARSA may occur as a solitary developmental anomaly, or in association with other vascular anomalies such as coarctation of the aorta, diverticulum of Kommerell, or possibly complete interruption of the aortic arch. ARSA is also seen more commonly in patients with chromosomal anomalies, particularly in trisomy 21, with a reported incidence between 19% and 36%.7-9 ARSA occurs with slightly higher incidence in patients with congenital cardiac anomalies at 2.9%, with conotruncal anomalies being the most commonly associated congenital cardiac anomaly. 10 Given these cardiac associations and the more frequent occurrence in female patients, it is suggested that ARSA is a developmental error rather than a normal variant. 4
In our literature search, we found mention of retrotracheal course of ARSA in the original description of this anomaly, which cites 12.7% to 25% of ARSA with retrotracheal course. 11 This figure likely originates from the historical paper by Holzapfel. 12 However, further literature search did not substantiate this figure, with almost all available reports of ARSA describing a retroesophageal in location. A small cadaveric study published recently identified 6 patients with ARSA, one of which demonstrated a retrotracheal course. 13 Two additional cadaveric case reports were also identified.14,15 We believe that there is no clear consensus on the epidemiology of this rare variant.
Developmentally, the aortic arch gives rise to 3 branches: the brachiocephalic trunk, the left common carotid artery, and the left subclavian artery, in order of proximal to distal. The brachiocephalic trunk extends a short distance superiorly, before branching into the right common carotid artery and the right subclavian artery. Detailed description of the embryology of the right subclavian artery is beyond the scope of this article. Briefly, the development of the aortic arch begins in the third week of gestation, with the proximal part of the right subclavian artery originates from the remnant of a mostly regressed fourth aortic arch. The distal portion of the right subclavian originates from the seventh intersegmental artery.16,17
In ARSA, the right subclavian artery instead arises as the most distal, fourth branch of the aortic arch where the right aortic arch is thought to regress between, instead of distal to, the common and right subclavian arteries. 18 This disrupts their fusion to form the brachiocephalic trunk, resulting in a left aortic arch with 4 great vessels.19,20 We have not found any proposed hypothesis on how the aberrant subclavian artery is able to interpose between the trachea and esophagus.
Alternatively, our presentation may represent a rare postsurgical complication, with transposition of the ARSA to a retrotracheal location. This rare complication also has not been reported in our literature search for postsurgical complications of TEF repair. An analysis of post-TEF repair spanning 2 decades found the most common complication was symptomatic stricture, without report of a transposed ARSA. 21 Two other studies examining 104 and 445 patients with EA and TEF repair also did not report any cases of transposed ARSA.22,23 Despite this, we may conclude that the retrotracheal course of the subclavian artery in this case may have been the result of repositioning during the TEF repair and esophageal anastomosis.
Due to the rarity of a retrotracheal course of the ARSA, whether it be congenital or acquired, there is no clearly established common presentation of this anomaly. Majority of retroesophageal ARSA cases are also clinically silent, with symptoms in 10% to 33% of cases, which may either be due to abnormal course of the anomalous vessel or due to the presence of a diverticulum of Kommerell.13,24 Specifically, the symptoms of ARSA occur at separate lifetime extremities with different manifestations. Infants typically present with stridor, wheeze, or increased frequency of pulmonary infections secondary to a more distensible trachea. Dysphagia and tracheal obstruction are common in children. 25 Adults have a completely formed cartilaginous trachea, so respiratory symptoms are rare, but they may exhibit the aforementioned “dysphagia lusoria.” 26
We postulate that the symptoms with a retrotracheal ARSA would be similar to that of a vascular sling by an aberrant right pulmonary artery, the most common of which is stridor from tracheal stenosis.24,27,28 In our patient, there was stridor as well as significantly increased frequency of pulmonary infections. Despite his advanced age, the patient continued to have pulmonary symptoms from the retrotracheal course of the ARSA, similar to cases of right pulmonary artery sling.
The diagnosis of ARSA can be established noninvasively via imaging. A contrasted upper gastrointestinal series or esophagram using barium or water-soluble contrast will demonstrate indentation of the esophagram on posteroanterior projection (Figure 1). 29 Unlike in cases of retroesophageal ARSA, a retrotracheal ARSA would be expected to show anterior indentation of the esophagus, as in our case (Figure 1). CT or CT angiography will allow for more precise delineation of the aberrant anatomy, as well as the relationship of the vessel to adjacent structures. Multidetector row CT with 3-dimensional volume rendering and CT angiography have been shown to be effective in vascular imaging. 30
The current available literature for the treatment of ARSA are restricted to treatment of the symptomatic retroesophageal variant. In such events that surgical intervention is advised, there are several approaches including sternotomy, left lateral thoracotomy, and/or right supraclavicular cervicotomy. If symptomatic with aneurysmal formation, an Right Subclavian Artery (RSCA) ligature is recommended. If symptomatic without an aneurysm, previous reports suggest a right supraclavicular approach for ligature close to the aortic arch to prevent complications of right upper extremity claudication. 31 However, given the unique positioning of a retrotracheal ARSA, proper identification and communication with the treatment team is critical for surgical planning.
In summary, a retrotracheal ARSA is an uncommon entity. It is very rarely reported in cadaveric studies, and currently we believe we presented the first case with imaging diagnosis in a living patient. Alternatively, our case presentation may also be due to a possible postsurgical complication in TEF repair; again, we did not identify any previous reports of a similar case. While the etiology of this case may either be congenital or postsurgical, the clinical presentation resembles that of a pulmonary arterial sling. Given the rarity of this condition, it is unclear what would be the optimal medical management, which could be a future area of further research.
Footnotes
Author Contributions
GGS: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SL: Contributed to conception and design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MW: Contributed to conception; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
LW: Contributed to conception; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
PS: Contributed to conception; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.