
Abstract
Objective. Consequences of mild head injury for behavioral adjustment have not been well researched, and little is known about the long-term effects of mild head injury for attention-deficit hyperactivity disorder (ADHD). Methods. In this longitudinal study of 418 children in Jintan City, China, parents reported children’s history of head injury at age 6 years, and the Child Behavior Checklist was used to measure child iDSM-IV-oriented ADHD at ages 6 (Wave I) and 12 years (Wave II). Regression models were used to calculate the long-term (Wave II) effect of mild head injury on diagnosed ADHD, while controlling for diagnosed ADHD in Wave I. Results. Fifty-seven children (13.6%) had a single injury and 42 (10.0%) had multiple injuries before the age of 6 years. The long-term effect of multiple mild injury on ADHD at age 12 years was significant (R2 = 0.103, P < .05), even after controlling for ADHD at age 6 years. Conclusions. Multiple, but not single, mild head injuries before the age of 6 years had a significant long-term effect on ADHD. Thus, injuries traditionally overlooked and underreported still pose significant risks to children’s long-term behavioral development.
Introduction
Childhood head injuries have gained increasing attention for their significant associations with long-term behavioral and psychosocial consequences.1-3 Attention problems are among the most prevalent behavioral symptoms reported after brain injury,1,2,4 with approximately 30% to 50% of children developing symptoms of attention-deficit hyperactivity disorder (ADHD) soon after traumatic brain injury (TBI)4-7 and secondary ADHD diagnosed 3 times more in children sustaining head injuries than in their uninjured peers. 4 ADHD is among the most common neurodevelopmental disorders of childhood, characterized by a pattern of inattention, hyperactivity, and impulsivity that interferes with functioning and development, pervades across settings, and often persists until adulthood (according to the Diagnostic and Statistical Manual of Mental Disorders [DSM], Fifth Edition, and the Centers for Disease Control and Prevention [CDC]).8,9 The CDC estimates that in 2011 approximately 11% of children aged 4 to 17 years—or 6.4 million children—have ever received a diagnosis of ADHD.
While it has been previously thought that children with behavioral problems such as ADHD are more prone to injuries, this belief is largely based on research in postinjury recall of preinjury behavior,10-12 and prospective studies using preinjury behavior assessment have not found behavioral problems to significantly predict head injury events.11,13,14 It is thus critical to recognize that postinjury behavioral deficits such as ADHD may not simply reflect preinjury characteristics or developmental trajectory but instead result from the injury event itself. 15 Indeed, a recent meta-analysis in both pediatric and adult populations, however, showed strong evidence for the association between ADHD and mild TBI (mTBI), with the strength of the relationship indicating that mTBI may be the precursor to ADHD. 16 Experimental models in young rodents have similarly demonstrated that even mild head injury can lead to the development of ADHD symptomatology, including deficits in sustained attention, response inhibition, and impulsivity.17,18
As mTBI accounts for nearly 75% of all TBI cases,19-22 gaining a clearer understanding of the outcomes of childhood mTBI is critical, especially as milder injuries are likely underreported and overlooked by patients and providers. Despite the importance of closely examining mild head injuries and their potential long-term outcomes, the current evidence regarding childhood mTBI and ADHD has been mixed6,23-25 and limited by small sample sizes, 24 relatively short follow-up,26,27 retrospective or cross-sectional design,5,25,28 and findings based only from a handful of cohorts, none of which are from non-Western countries. Moreover, while studies examining ADHD compare children with various severity of brain injury to uninjured cohorts, 2 to our knowledge no study has examined the significance of frequency of head injuries in ADHD.
The present study aims to begin addressing these gaps in the existing literature by longitudinally examining the associations between parent-reported single and multiple mild head injuries—defined by no loss of consciousness (LOC) or hospitalization—in early childhood and development of ADHD in a community-based cohort of Chinese children.
Methods
Participants
The current study was part of a larger population-based community cohort study of 1656 Chinese children (55.5% boys, 44.5% girls) initially recruited between fall 2004 and spring 2005 from Jintan city, located in the southeastern coastal region of mainland China. Detailed sampling and research procedures of this cohort study have been described elsewhere.29,30 Briefly, the China Jintan Child Cohort Study is an ongoing prospective longitudinal study with the main aim of assessing the early health risk factors for the development of child neurobehavioral outcomes. 31 From the original cohort, this analysis involved 418 children who had complete data for both Wave I, collected when children were in their last year of kindergarten at age 6 years, and Wave II, conducted between 2011 and 2013 when children were 12 years old. The remaining data were not available for various reasons (eg, children moved to other schools, did not respond, or refused to participate). There were no significant differences between children with available data and unavailable data. At Wave I, parents were asked to report the history of head injuries. Parents also rated child behavioral outcomes using the Chinese version of the Child Behavior Checklist (CBCL)30,31 both at Waves I and II. Written informed consent was obtained from parents. Institutional review board approval was obtained from both the University of Pennsylvania and the ethical committee for research at Jintan Hospital in China.
History and Operational Definition of Mild Head Injury
At Wave I, when children were 6 years old, parents reported whether their child had a history of head injury (ie, “Has your child ever had a head injury before?” and “How many injuries did he/she have?”), mechanism of injury (ie, slips, falls, traffic, exercise, fighting), age of injury, hospitalization history, and severity of injury (loss of consciousness). Questions were asked in Chinese. Children’s head injury histories were categorized as no head injury, single head injury, and multiple head injuries. The injury mechanism was not included in analysis due to low frequencies. Due to the unavailability of valid medical data, this study could not define head injury using medical diagnoses. Thus, for the purposes of this study, mild head injury was defined as no loss of consciousness and no hospitalization for treatment due to injury.
Child’s ADHD
Parents were asked to rate children’s behavior with the Chinese version of the CBCL,32-34 and at the same time head injury history was collected when children were 6 years old (Wave I) and when children were 12 years old(Wave II). The CBCL is one of the most widely used rating scales for assessing behavioral and emotional problems in children and consists of 99 items dealing with a child’s behavior within the past 12 months. Items were rated on a 3-point scale (0 = Not True, 1 = Sometimes True, or 2 = Often True). 32 Standardized t scores were calculated from raw scores. One of the DSM-IV-oriented factors derived from CBCL, namely ADHD, was commonly used to assess children’s ADHD. In the present study, we used the DSM-IV-oriented ADHD in Wave II as the long-term outcome of mild head injury.
Statistical Analysis
Because this study was focused only on mild head injuries, after excluding 41 children who were reported to have loss of consciousness or hospitalization, a total of 418 children were included in this analysis. A 1-way analysis of variance (ANOVA) and correlation analyses were conducted to evaluate the association of mild head injury and ADHD measured at age 6 years and 12 years, respectively. A general linear model was used to calculate the long-term (Wave II) effect of single mild head injury and multiple injuries (no head injury as reference) on DSM-IV-oriented ADHD, and a logistic regression model was used to test the odds ratio of DSM-IV-oriented ADHD. All analyses were conducted in SPSS, version 22.0 (IBM Corp, Armonk, NY). Potential confounders were controlled in linear regression models and logistic regression. Potential confounders included DSM-IV-oriented ADHD in Wave I, children’s sex, father’s education, and marital status of parents.
Results
Sample Characteristics
Of the 418 children, 57 (13.6%) had a single injury and 42 (10.0%) had multiple injuries. Table 1 compares parental and children’s characteristics of children with and without head injury histories. There were no significant differences in children’s and parental characteristics (all P > .05), expect father’s education level (P < .05).
Characteristics of Children With and Without Mild Head Injury History (N = 418).

Associations of Mild Head Injury and DSM-IV-Oriented ADHD in Wave I and Wave II
The results of the ANOVA indicated that there are significant differences of DSM-IV-oriented ADHD in Wave II among the 3 mild head injury groups (P < .05; Figure 1 and Table 2). DSM-IV-oriented ADHD in Wave I was significantly positively related to DSM-IV-oriented ADHD in Wave II (P < .001).

Early childhood mild head injury and ADHD1 (age 6 years) and ADHD2 (age 12 years).
Associations of Mild Head Injury and DSM-IV-Oriented ADHD in Waves I and II.

Abbreviations: DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; ADHD, attention-deficit hyperactivity disorder; LSD, least significant difference; ADHD1, DSM-IV-oriented attention-deficit hyperactivity disorder in Wave I; ADHD2, DSM-IV-oriented attention-deficit hyperactivity disorder in Wave II.
Differences between ADHD1 and ADHD2.
P < .001.
Association of Mild Head Injury and Long-Term ADHD
In the general linear model, after adjusting for covariates, those with multiple injuries had statistically significant higher t scores for DSM-IV-oriented ADHD in Wave II (Table 3). The logistic regression of children with and without DSM-IV-oriented ADHD showed that children with multiple injuries compared with those with no head injury were more likely to have DSM-IV-oriented ADHD (odds ratio = 2.036, P = .056).
The General Linear Models of DSM-IV-Oriented ADHD (N = 418).
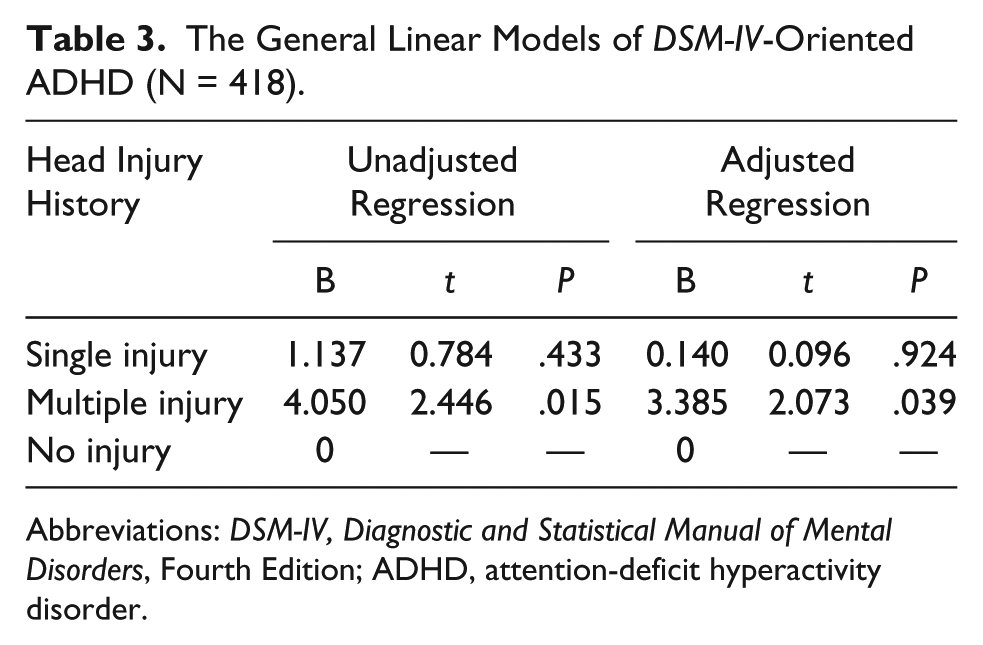
Abbreviations: DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; ADHD, attention-deficit hyperactivity disorder.
Discussion
The present study focused on DSM-IV-oriented ADHD associated with mild head injuries, defined as parent-reported head trauma without loss of consciousness or hospitalization. Among our cohort of 481 children, 99 (23.7%) children were reported by parents to have sustained mild head injuries before the age of 6 years, 42.4% of whom sustained multiple injuries. Our findings demonstrate that compared with children without any history of head injury before the age of 6 years, multiple, but not single, mild head injuries are significantly associated with long-term DSM-IV-oriented ADHD as assessed at the age of 12 years (Wave II), even after controlling for ADHD at 6 years of age and other potential confounding factors.
In this study, neither single nor multiple head injury was associated with ADHD at the age of 6 years (Wave I). This was previously reported in our cohort 35 and highlights the importance of longitudinal follow-up, supporting previous observations that the occurrence of externalizing behaviors may be age-dependent 36 with the emergence of attention problems more noticeable in middle-to-late childhood. Indeed, in their study of preschool mTBI, the emergence of parent-reported attention problems peaked around age 11 to 12 years. 6
New-onset attention problems are among the most common behavioral problems to arise after TBI in children, 2 and animal models have demonstrated that even mild injury can lead to the development of ADHD symptomatology in young rodents.17,18 Imaging studies have further shown that some of the most common areas of white matter injury resulting from mTBI include long-coursing pathways within the corona radiata, such as the default mode network that participates in regulation of attention. 37 In their longitudinal study of a New Zealand cohort of children, McKinlay et al 24 reported that compared with uninjured peers, children hospitalized with mTBI before 5 years of age (n = 19) were significantly more likely than uninjured peers (n = 839) to have ADHD symptoms at ages 14 and 16 years (P < .05). Interestingly, however, children with mTBI who did not require hospitalization (outpatient mTBI; n = 57) did not significantly differ from uninjured peers in later ADHD. The authors thus highlight a severity gradient existing within mTBI, and the challenge of clinical significance for many milder head injuries.
In our current study, only children with mild head injuries not involving LOC or hospitalization were included, essentially classifying these as lower grade mild head injuries. Like McKinlay et al, 24 we found that compared with uninjured children, children with a history of mild head injury without hospitalization were not significantly more likely to develop ADHD symptomatology later in childhood. Importantly, however, we demonstrated that when children sustained multiple of these lower severity injuries, they were significantly more likely than uninjured peers to show later ADHD symptomatology. Given the lower grade of head injuries included in our study, it is plausible that only the aggregate damage caused by repeated injuries manifested as detectable attention problems. Indeed, we have previously reported that multiple, but not single, mild head injuries without LOC or hospitalization are associated with several internalizing and externalizing behaviors as measured by the CBCL at age 6 years. 35 Multiple mTBIs have also been found to cumulatively affect adult 38 and adolescent populations, 39 and in recent years repetitive mTBIs have gained increasing attention from patients, families, researchers, and the public given the emerging relation with neurodegenerative diseases including chronic traumatic encephalopathy, most commonly seen in athletes suffering multiple concussions or military personnel incurring blast trauma. A growing body of research in animal models has identified several histologic, neuropathologic changes occurring with repetitive mTBIs, including cumulative damage to hippocampal cells, 40 ventriculomegaly and cortical thinning, 41 and white matter damage 42 that may significantly mediate behavioral outcomes. 43
Several limitations in this study should be noted. First, mild brain injuries were parent-reported and defined as head injuries not associated with LOC or requiring hospitalization or treatment. They were not obtained through medical data or defined by objective measures such as the Glasgow Coma Scale, 44 commonly used elsewhere in the literature to define TBI severity. While this prevents our ability to utilize terminology that is consistent with the existing literature, our use of parent-reported injuries allowed us to capture head injuries that were mild enough to not be brought to the attention of medical personnel, as relying on objective measures such as hospital records likely causes for underreporting of mild head injuries. Furthermore, with decreasing rates of hospitalization among children with mTBI, 45 future research on the outcomes of these injuries will likely rely on similar parent-reported classifications. Second, despite the longitudinal design of our study, the directionality of our findings may still be challenged. It is plausible, for instance, that children with ADHD are more prone to having more injuries including head trauma at a young age. However, as aforementioned, prospective studies have not found behavioral problems to significantly predict head injury events,11,13,14 and animal studies have modeled head injury events leading to ADHD symptomatology.17,18 Finally, our cohort is from a single county in China, and the generalizability to other Chinese children or children in other countries is unknown.
Despite these limitations, to our knowledge this study is the first to recognize the significant effect of multiple mild head injuries in DSM-IV-oriented ADHD. Our finding that even lower severity head injuries may have lasting behavior outcomes in the developing brain holds important implications. Many cases of mild head injuries, especially those that do not cause LOC, are likely overlooked by both parents and medical professionals. An unknown number of cases are not brought to medical attention, and among those that are, they are frequently underreported. For instance, one study that prospectively interviewed subjects admitted to the emergency department for possible head injuries before looking in their charts found that over half of mTBI cases identified by researchers were absent from emergency department medical records. 46 Furthermore, while algorithms such as the Pediatric Emergency Care Applied Research Network rule have helped clinicians avoid unnecessary imaging of many minor pediatric head injuries, they have also characterized “clinically important” mTBI as having certain features such as hematomas, LOC ≥5 seconds, severe mechanisms of injuries, or immediate behavior changes. 47 However, our findings demonstrate that the cumulative effect of head injuries without characteristics deeming them clinically important may still pose significant risks to children’s behavioral development, especially when multiple insults are incurred. Health care providers should thus be careful to not simply dismiss such head injuries in children. Efforts such as screening questions through intake forms at regular pediatric appointments, for instance, may help identify children who have a history of multiple head injuries and thus may be at risk for developing behavioral problems. As ADHD symptomatology can be hard to detect in young children and may become more noticeable in middle to late childhood, early screening for risk factors such as head injuries can allow for earlier interventions. Moreover, studies have demonstrated that children developing ADHD following TBI have differing patterns of executive control performance than those with preinjury ADHD, suggesting different underlying neural mechanisms between primary and secondary ADHD. Further research into ADHD after TBI will thus be critical for developing and evaluating specifically targeted interventions.
Conclusion
Childhood head injuries are a significant public health concern and associated with development of behavioral sequelae later in life. The present longitudinal study used a large cohort of Chinese children to demonstrate that multiple, but not single, parent-reported mild head injuries before the age of 6 years is significantly associated with DSM-IV-oriented ADHD at the age of 12 years, even after controlling for ADHD at 6 years of age. In this study, mild head injury was defined as not associated with loss of consciousness or hospitalization, categorizing such injuries as lower grade mild head injuries that are more likely assumed as benign. Our findings, however, suggest the cumulative effect of these lower grade injuries may have a significant effect on later ADHD symptomatology. Continued research is necessary to better understand the mechanisms and outcomes of mild head injuries, increase awareness of the risks they pose among both the public and health care profession, and develop effective programs and treatments to minimize the potential lasting, detrimental sequelae they have in childhood development.
Footnotes
Acknowledgements
Thanks are extended to the participating children and their families from Jintan City, and to the Jintan Cohort Study Group. We are grateful to the Jintan city government and the Jintan Hospital for their support and assistance.
Author Contributions
LL: Contributed to interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
YL: Contributed to analysis, acquisition; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
CM: Contributed to conception and design; contributed to interpretation; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JL: Contributed to conception and design; contributed to acquisition, interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Environmental Health Sciences and the National Institutes of Health (R01-ES-018858, K02-ES-019878, and K01-ES015877).