
Abstract
Objectives:
It remains uncertain whether nonconvulsive seizures and nonconvulsive status epilepticus in pediatric traumatic brain injury are deleterious to the brain and/or impact the recovery from injury. Consequently, optimal electroencephalographic surveillance and management is unknown. We aimed to determine specialists’ opinion regarding the detection and treatment of nonconvulsive seizures or nonconvulsive status epilepticus in pediatric traumatic brain injury, regardless of their practice.
Methods:
In 2012, 183 surveys were sent to all 93 neurologists, 27 neurosurgeons, and 63 intensivists in the14 tertiary pediatric hospitals across Canada. The survey included an initial scenario of pediatric TBI that evolved into three further scenarios. Each scenario had required responses and an embedded branching logic algorithm ascertaining clinical management. The survey instrument assimilated data about the importance of nonconvulsive status epilepticus and nonconvulsive seizures detection and treatment, and whether they are a cause of brain injury that adversely affects neurologic outcomes.
Results:
Of the 79 specialists who replied (43% response rate), 68%–78% elected to order an electroencephalographic across all four scenarios, and one-third (31%–36%; scenario dependent) would request an urgent electroencephalographic (within the hour) in the comatose pediatric traumatic brain injury patient. In the absence of pharmacologic paralysis or intracranial pressure spikes, half-hour electroencephalographic (41%–55%) was preferred over ⩾24-h continuous electroencephalographic monitoring (29%–40%). Finally, nonconvulsive status epilepticus (81%–87%) and nonconvulsive seizures (61%–73%) were considered to be a cause of poor neurologic outcomes warranting aggressive pharmacologic management.
Conclusion:
The Canadian specialists’ opinion is that nonconvulsive seizures and nonconvulsive status epilepticus are biomarkers of brain injury and contribute to worsened outcomes. This suggests the urgency of future outcome-oriented research in the identification and management of nonconvulsive seizures or nonconvulsive status epilepticus.
Introduction
Current Brain Trauma Foundation practice guidelines for both adult 1 and pediatric 2 severe traumatic brain injury (TBI) do not recommend electroencephalography (EEG) for the detection of nonconvulsive status epilepticus (NCSE) or nonconvulsive seizures (NCS). In contrast, 53% of surveyed North American pediatric neurologists recently responded that TBI was an indication of EEG monitoring. 3 Furthermore, the European Society of Intensive Care Medicine, based on low quality of evidence, weakly recommended EEG monitoring to rule out NCS in severe TBI. 4 Similarly, the Neurocritical Care Society Status Epilepticus Guideline Writing Committee reported that continuous EEG (cEEG) is indicated with intracranial hemorrhage and TBI until cessation of NCS. 5
In adults, NCS have been found in 0%–29%6–11 of moderate to severe TBI patients often receiving a broad range of antiseizure prophylaxis. In pediatric TBI, NCS have been reported in 16%–43%12–15 of patients and may be associated with younger age, abusive head trauma, and intra-axial bleed. 15 However, in these studies, cEEG was not uniformly obtained in the acute phases of brain injury.
It remains controversial whether NCS or NCSE is deleterious to the brain and/or impacts the recovery from TBI. The presence of seizures may simply be a marker associated with the severity of the originating brain injury. While morbidity and mortality appear to be high in adults16–20 and children13,15,21–26 with serious acute neurologic diagnoses and NCS or NCSE, the paucity of large prospective follow-up studies do not allow for conclusions to be made about long-term sequelae in survivors. Nevertheless, emerging evidence suggests associations between NCS and prolonged elevations in intracranial pressures, 27 adverse brain tissue metabolic changes, 27 hippocampal atrophy, 7 elevations of neuron-specific enolase,28–30 excitotoxicity,31,32 and expanding intracerebral hemorrhage with mass effect and shift.19,33
The aim of our survey was to determine the opinions (not necessarily the practice) of Canadian pediatric intensivists, neurologists, and neurosurgeons on the use of EEG for detection and management of NCSE and/or NCS in severe pediatric TBI and the causal importance of detected NCSE and/or NCS on adverse outcomes. In Canada, it is typically the intensivist and neurosurgeon who are managing the patient with TBI, and neurologists are involved when consulted for EEG or clinical questions.
Methods
Questionnaire development
We searched PubMed using the keywords “seizures” and “traumatic brain injury” and limited to “children” for the most recent 3 years. Original studies reporting in their title or abstract on EEG monitoring of children after TBI in a pediatric intensive care unit (PICU) were retrieved, and their reference list was reviewed. The search was later expanded by removing the keyword “children” and the 3-year time limitation. Relevant articles (n = 45) were reviewed by two authors (G.H., A.R.J.) to determine important questions for the survey.
Following a review of the relevant articles, we identified six major domains relevant to pediatric TBI: threshold to utilize EEG for NCSE or NCS diagnosis, duration of EEG monitoring for diagnosis, treatment targets or goals, pharmacologic treatments utilized, rationale for treating NCSE or NCS, and association of NCS or NCSE with outcomes. The preliminary item list consisted of questions that targeted these domains, repeated in four slightly different clinical scenarios. To ensure clarity, face validity, and ease of completion, three accredited neurologists completed the pilot testing. The pilot was followed by a semistructured interview utilizing a clinical sensibility testing tool, 34 to address potential redundancy and omission of crucial issues, leading questions, ease of the survey, and if our outlined objectives were addressed. A few modifications ensued, and a final survey draft was proposed and approved by the Health Research Ethics Board from the University of Alberta.
Questionnaire administration
Contact information from the pediatric subspecialists at all 14 tertiary children’s hospitals with a PICU was gathered from university and hospital directories and local sources. In 2012, 183 surveys were sent to all 93 neurologists, 27 neurosurgeons, and 63 intensivists. Each staff physician was emailed a cover letter that briefly outlined the content and rationale of the survey. The cover letter stated, “we want to sample the opinions of pediatric neurologists, intensivists and neurosurgeons across Canada about the role of EEG for the diagnosis of NCS/NCSE and their subsequent management in severe pediatric TBI.” This was followed by another email that contained a link to the survey created through REDCap, a web-based application designed to support data capture for research studies and that ensures secure web authentication, secure layer encryption, and anonymous participant responses. 35 A second-, third-, and fourth-reminder email was sent to nonresponders at approximately 3-week intervals. No incentive was provided for the survey respondents.
Survey
The survey (Table 1) included an initial scenario of a 13-year-old pedestrian or motor vehicle collision with TBI. This basic scenario evolved into three further scenarios that included spikes in intracranial pressure (ICP), paralysis for targeted temperature management with cooling, and finally a witnessed generalized seizure once the paralysis was stopped. For each scenario, required responses addressed the opinions about urgency of EEG monitoring and whether NCS or NCSE caused poor neurologic outcomes. An embedded branching logic algorithm ascertained what the respondent “would” do for further clinical management.
Description of the survey instrument.

MVC: motor vehicle collision; GCS: Glasgow Coma Scale; SDH: subdural hematoma; BP: blood pressure; CT: computed tomography; ICP: intracranial pressure; EEG: electroencephalography; cEEG: continuous electroencephalography; NCS: nonconvulsive seizures; NCSE: nonconvulsive status epilepticus.
Definitions
Definitions were provided with the survey. NCS were defined as an abnormal paroxysmal event that was different from the background lasting longer than 10 s with temporal–spatial evolution in morphology, frequency, and amplitude and with a plausible electric field together with little or no motor movements. 12
NCSE was defined as a 30-min electroencephalographic seizure or a series of recurrent independent electroencephalographic seizures totaling more than 30 min in any 1-h period (50% seizure burden), with little or no motor movements. 12 cEEG was defined as an EEG for at least 24-h duration.
Data management and statistics
Data were collected and managed using REDCap. 35 Anonymous data were exported into a password-protected computer database (SPSS version 15) in a locked office at the University of Alberta Hospital. Responses were analyzed using standard tabulations. Variables expressed as percentages document the proportion of respondents with different answers. We made comparisons of responses between two pre-specified subgroups: by cEEG availability and by specialty. Comparisons were by chi-square or Fisher’s exact test as appropriate. With Bonferroni correction, with 16 questions per scenario, a p-value of <0.003 was required for statistical significance. We identified one post hoc subgroup question analyzed with chi-square statistic are those that request an EEG in each scenario more likely to believe NCS or NCSE cause adverse outcome.
Results
Demographics of respondents
A total of 79 of 183 (43%) survey responses were returned from 46 of 63 (73%) intensivists, 26 of 93 (28%) neurologists, and 7 of 27 (26%) neurosurgeons. All physicians practiced in an academic or tertiary center, and most practiced exclusively in pediatrics (74 of 79, 94%). Routine EEG was available at all times for 21 (27%), weekday hours with exceptional weekends for 50 (64%), and only standard weekday hours for 7 (9%) respondents. cEEG was available at all times for 32 (42%), weekday hours with exceptional weekends for 40 (52%), and only standard weekday hours for 5 (7%) respondents. At their institutions, <1, 1–5, 6–10, and >10 patients have cEEG each month for 26 (33%), 40 (51%), 8 (10%), and 4 (5%) respondents.
Survey responses
The results from the three main questions and subsequent embedded logic algorithm questions are summarized in Tables 2–4.
Responses to the first question in four TBI scenarios: would you ask for an EEG?.
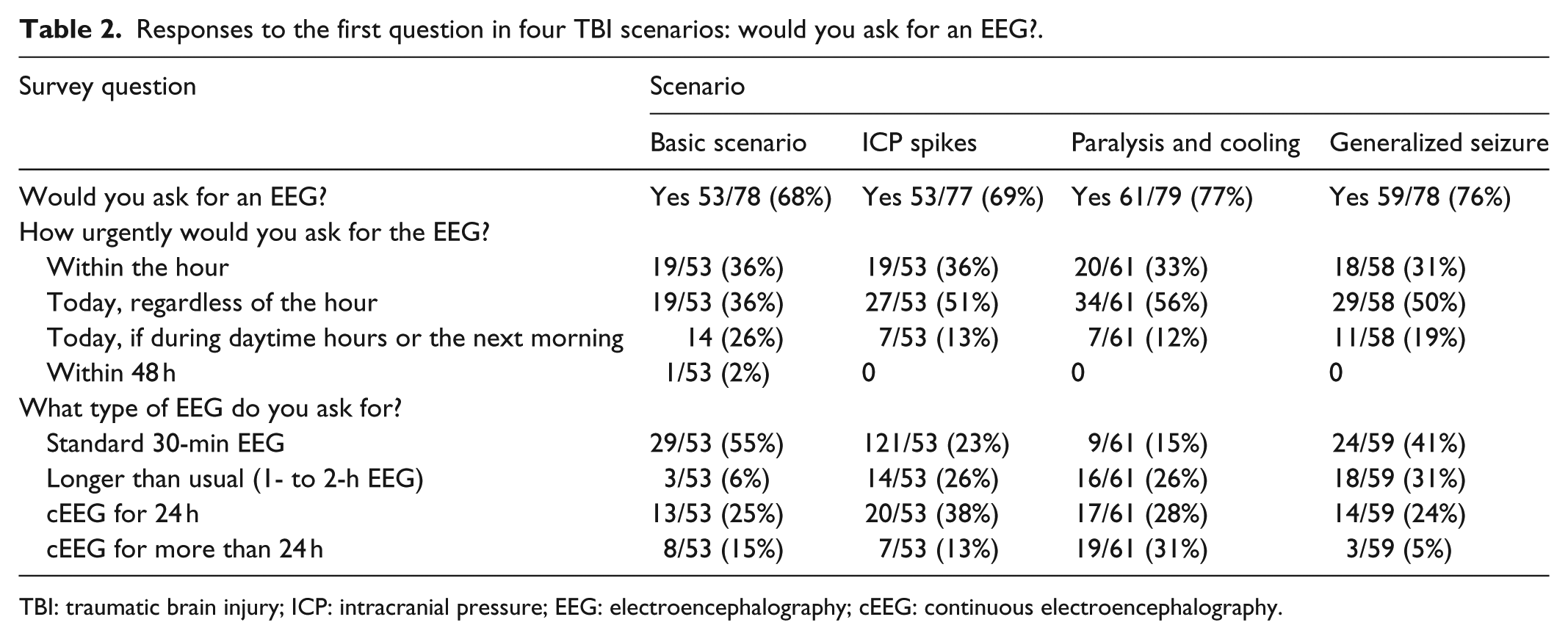
TBI: traumatic brain injury; ICP: intracranial pressure; EEG: electroencephalography; cEEG: continuous electroencephalography.
Responses to the second question in four TBI scenarios: NCS are detected on the EEG, when would you decide to treat these NCS?.

TBI: traumatic brain injury; NCS: nonconvulsive seizures; ICP: intracranial pressure; EEG: electroencephalography.
Responses to the third question in four TBI scenarios: NCSE is detected on the EEG; would you treat this NCSE?.
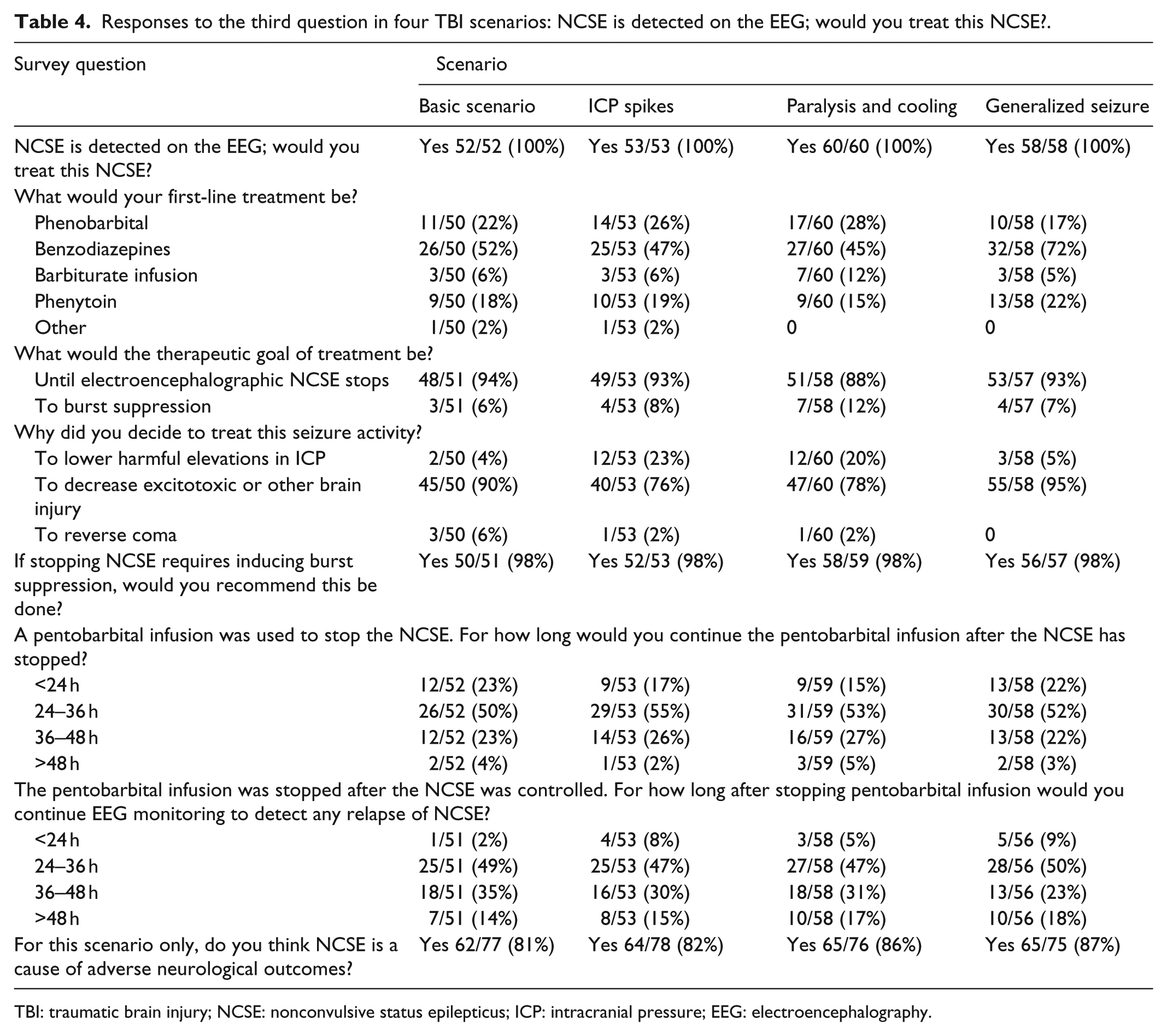
TBI: traumatic brain injury; NCSE: nonconvulsive status epilepticus; ICP: intracranial pressure; EEG: electroencephalography.
Would you ask for an EEG?
Across all four scenarios (Table 2), a range of 68%–77% of specialists elected to order an EEG, with the highest percentage corresponding to the only scenario involving pharmacologic paralysis. An urgent EEG within the hour was requested by 31%–36% of respondents, with 29%–59% advocating for a cEEG of at least 24 h.
When would you treat NCS?
If any NCS were detected (Table 3), 63%–70% of specialists would treat these seizures. The therapeutic goal of stopping all NCS was stated by 66%–76% of respondents, in attempts to either decrease excitotoxic or other brain injury (59%–97%) or lower harmful elevations of ICP (24%–40%). NCS were thought to be a cause of adverse neurologic outcomes by 61%–73% of specialists.
When would you treat NCSE?
If NCSE were detected on EEG (Table 4), 100% of physicians would treat these NCSE to either decrease excitotoxic or other brain injury (76%–95%) or lower harmful elevations of ICP (20%–23%). Poor neurologic outcomes were causally attributed to NCSE by 81%–87% of respondents.
Subgroup analyses
The only statistically significant difference between respondents according to availability of cEEG at their institution was for the question, “Why did you decide to treat this [NCS] activity?” Those with cEEG available at all times, on weekday hours with exceptional weekends, and only standard weekday hours decided to treat NCS to reverse coma in 2 of 26, 0 of 22, and 2 of 3, respectively (p = 0.001).
The only statistically significant differences in responses between pediatric intensivists and neurologists were in scenarios 1 and 4, for the question, “A pentobarbital infusion was used to stop the NCSE. For how long would you continue the pentobarbital infusion after the NCSE has stopped?” Intensivists were more likely to respond “<24 h” (10 of 32 in baseline scenario and 11 of 28 in generalized scenario) than neurologists (2 of 21 in baseline scenario and 1 of 21 in generalized seizure scenario) (p < 0.001). We did not include neurosurgeons in these subgroup analyses due to their low response rate. Physicians who requested an EEG were more likely to respond that NCS and NCSE cause adverse neurologic outcomes, in all four scenarios (Table 5).
Post hoc subgroup analysis to determine whether asking for an EEG is associated with the opinion that NCS or NCSE cause adverse neurological outcome.

EEG: electroencephalography; NCS: nonconvulsive seizures; NCSE: nonconvulsive status epilepticus; ICP: intracranial pressure.
Discussion
In our survey of Canadian pediatric intensivists, neurologists, and neurosurgeons, we found that more than two-thirds would order an EEG across all four scenarios. Only one-third would request an urgent EEG for the evaluation of NCS and NCSE in the setting of severe TBI with coma. Second, in the absence of pharmacologic paralysis and ICP spikes, standard or 1- to 2-h EEG was preferred over ⩾24-h cEEG monitoring, although a significant minority did ask for cEEG. Finally, NCS and NCSE were considered to be a cause of poor neurologic outcomes, and their management was directed at mitigating brain damage for the large majority of respondents.
Despite the absence of EEG monitoring in TBI management guidelines,1,2 the majority of respondents would request an EEG with all of the severe pediatric TBI scenarios. This is similar to two other surveys3,36 that reported 53%–96% of physicians requesting EEG with TBI and altered mental status. The highest request rate for our respondents was not surprisingly observed with pharmacologic paralysis as the neurologic examination would be severely limited.
There was variation among respondents in regard to the level of urgency for the EEG. For most respondents, a non-urgent EEG was sufficient. No further questions addressing the rationale for the chosen urgency were asked. This is in contrast to an older survey in which 79% of respondents asked for an immediate EEG if NCS were suspected. 37 Although resource allocation was not addressed in our survey, specialists may be balancing the high infrastructure costs and need for timely yet inconvenient EEG interpretations with perceptions of clinical usefulness or clinician’s increasing EEG “addictions.” 38 Another consideration may be differing opinions on how aggressively NCS or NCSE cessation should be managed.
Standard or extended 1- to 2-h EEG was preferred over cEEG (⩾24 h), particularly in the generalized seizure scenario (only 29% desired cEEG). Our findings are similar to another survey that reported 68% of respondents not asking for cEEG if NCS were suspected. 37 These observations, however, are not consistent with studies that demonstrated only 38.5%–50% of NCS detection occurring within the first hour of monitoring critically ill children, and 80%–100% detection occurring with 24-h monitoring.8,12,13,39 Strong evidence also suggests that clinical seizures are a major risk factor for NCS or NCSE.23,39,40
Canadian specialists who requested an EEG were more likely to believe that NCS and NCSE were causally associated with adverse neurological outcomes and described a low threshold to treat both NCS and NCSE. Although researchers have found it difficult to separate confounding co-morbidity with subsequent outcome of NCS or NCSE, 41 and health-care providers may question whether EEG monitoring changes outcomes, 38 our study suggests Canadian specialists accept the causal pathologic role of NCS or NCSE in adverse clinical outcomes. This is compatible with a recent review based on three pediatric studies (not limited to TBI) that found an association between a high NCS seizure burden and worsened outcome even after adjustment for potential confounders. 42
With NCS, 66%–76% of respondents stated that their goal of treatment was to stop all NCS. Whether this is the correct strategy is not known, as it may prolong duration of coma and intubation. Poor neurologic outcomes may be also associated with prolonging ventilation, length of intensive care unit (ICU) admission, and protracted exposure to benzodiazepine infusions, and consequently a rational approach that considers these multiple factors needs to be tested. 28 Clinical trials will be necessary to determine the efficacy and outcomes of treating NCS. 28
The survey has several potential limitations. Although our total response rate was 79 of 183 (43%), the risk of sampling bias with neurologists (28% response rate) and neurosurgeons (26% response rate) should not be overlooked. Hence, conclusions on specialist subgroup analyses were not emphasized in our discussion. Furthermore, despite our efforts to avoid leading questions in our pilot testing, our data may also reflect response biases due to the nature of the scenario progression. As this study addresses an emerging area that harbors a considerable array of opinions, voluntary response biases may overrepresent specialists with strong opinions. We cannot be certain whether responses reflect actual practice (i.e. what the respondent actually “would” do) or ideal practice (i.e. what the respondent “would” do given adequate resources); however, at a minimum, the responses reflect what clinicians believe is optimal patient management in the given scenarios. We cannot determine institutional preferences, as responses were automatically anonymize by the REDCap system. Finally, whether the findings here generalize to other countries cannot be answered.
Nevertheless, our study has several strengths. We have determined the stated opinions of a relatively large group of specialists that manage pediatric TBI patients in intensive care in Canada, with a reasonable response rate and with consistent findings between scenarios.
Conclusion
Our most important finding is that the large majority of Canadian specialists consider NCS and NCSE in the setting of pediatric TBI important to detect and treat and a cause of brain injury that adversely affects neurological outcomes. Standard or extended 1- to 2-h EEG studies were preferred over ⩾24-h cEEG monitoring for many respondents. Given the resource implications of frequent cEEG monitoring in severe pediatric TBI, and the opinion that NCS and NCSE are biomarkers of brain injury independently contributing to worsened outcome, urgent study is required to determine whether identification and management of NCS or NCSE improves outcomes.
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to disclose.
Funding
The authors do not have financial relationships relevant to this article to disclose.