
Abstract
Objective. To characterize children with non–malarial fever at risk of nonrecovery or worsening in rural Malawi. Methods. This is a subgroup analysis of patients ≤14 years of age from a prospective cohort study in non–malarial fever subjects (temperature ≥37.5°C, or fever within 48 hours, and malaria negative) in southern Malawi cared for at a mobile clinic during the 2016 dry (August to September) or wet (November to December) season. Data collection included chart review and questionnaires; 14-day follow-up was conducted. We conducted univariate descriptive statistics on cohort characteristics, bivariate analyses to examine associations between characteristics and outcomes, and multivariate logistic regressions to explore factors associated with nonrecovery. Results. A total of 2893 patients were screened, 401 were enrolled, 286 of these were children, and 280 children completed follow-up. Eighty-seven percent reported symptom resolution, 12.9% reported no improvement, and there were no deaths or hospitalizations. No improvement was associated with dry season presentation (42.6% vs 75.0%, P < .0003), >2 days of symptoms (51.6% vs 72.2%, P = .03), and food insecurity (62.3% vs 86.1%, P = .007). Dry season subjects had a 4.35 times greater likelihood of nonimprovement (95% confidence interval [CI] = 1.96-11.11). Household food insecurity and being >2 hours from a permanent clinic were associated with no improvement (adjusted odds ratio [AOR] = 4.61, 95% CI = 1.81-14.29; and AOR = 2.38, 95% CI = 1.11-5.36, respectively). Conclusion. Outcomes were generally excellent in this rural, outpatient pediatric cohort, though risk factors for nonrecovery included food insecurity, access to a standing clinic, and seasonality. Ideally, this study will inform clinic- and policy-level changes aimed at ameliorating the modifiable risk factors in Malawi and throughout rural Africa.
Introduction
While malaria accounted for more than half a million deaths globally in children and adolescents in 2015, non–malarial fever (NMF), which includes lower respiratory tract infections, sepsis, diarrheal disease, meningitis, HIV, and other infectious diseases, was responsible for more than 2 million global deaths. 1 Malawi is a malaria-endemic, low-income country in sub-Saharan Africa (SSA), with 64 per 100 000 under age 5 deaths in 2015. 2 Because of improved malaria diagnostic tests and increased availability of oral antimalarial regimens that make it possible to easily treat uncomplicated cases with excellent reductions in mortality,3,4 less than 10% of the under age 5 deaths in Malawi are attributed to malaria. 2 Among children under age 5 in Malawi, an estimated 67% of those seeking medical care have had a fever within the last 2 weeks 5 ; however, the prevalence of malaria in this population is 37%, signifying that NMF is an important consideration even in malaria-endemic regions. 6
The Global AIDS Interfaith Alliance (GAIA) of Malawi is a nongovernmental organization established in 2000 and initially focused on mitigating the devastation caused by the HIV epidemic. Funded by the Elizabeth Taylor AIDS Foundation, GAIA began using a mobile health clinic model in 2008 to reach the rural underserved. GAIA’s 7 mobile clinics staffed by clinical officers, registered nurses, and nurse midwifery technicians now care for 15 000 to 20 000 patients per month, 50% of whom are children under the age of 15 years. Patients present with a wide variety of illnesses, with fever as one of the most frequent chief complaints; 50% to 90% (season-dependent) of patients have NMF.
Because of the development of the malaria rapid diagnostic test (mRDT), malaria is now quickly and reliably diagnosed in resource-limited settings 3 such as Malawi, and the overall prevalence is significantly decreasing given massive preventative campaigns.2,5 Far less is known about the prevalence and patient outcomes associated with pediatric NMF, however. We therefore aimed to characterize NMF in a rural, outpatient pediatric population, determine patient outcomes, and identify children at greatest risk of needing follow-up and/or referral to a higher level of care.
Methods
This is a subgroup analysis of exclusively pediatric data (≤14 years) from a larger prospective cohort study including adults and children with NMF in the rural districts of southern Malawi who sought care at the Muloza (Phalombe District) or Nkanda (Mulanje District) GAIA mobile clinics during either the dry (August to September, 2016) or wet (November to December, 2016) season (Figure 1). Patients met inclusion criteria if they had an axillary temperature of 37.5°C or higher or a history of fever within 48 hours and underwent mRDT testing (Paracheck-Pf) with a negative test result. Patients in extremis or obtunded were excluded, as were patients already enrolled and presenting for a subsequent visit, known to be unavailable or unreachable for follow-up, who did not speak English or Chichewa fluently, or who did not provide consent. Specifically, in the case of children, those whose guardians did not speak English or Chichewa fluently or were unavailable to consent (eg, a child being supervised at the clinic by a minor) were also excluded. At the initial clinic visit, we used both medical chart review and direct guardian questionnaires to collect demographic data, socioeconomic status indicators, chief complaint, diagnosis, treatment prescribed, referral status, and assess care seeking practices and food insecurity. Separate patient logbooks detailing HIV and tuberculosis status were unavailable to research staff during the period of the study.
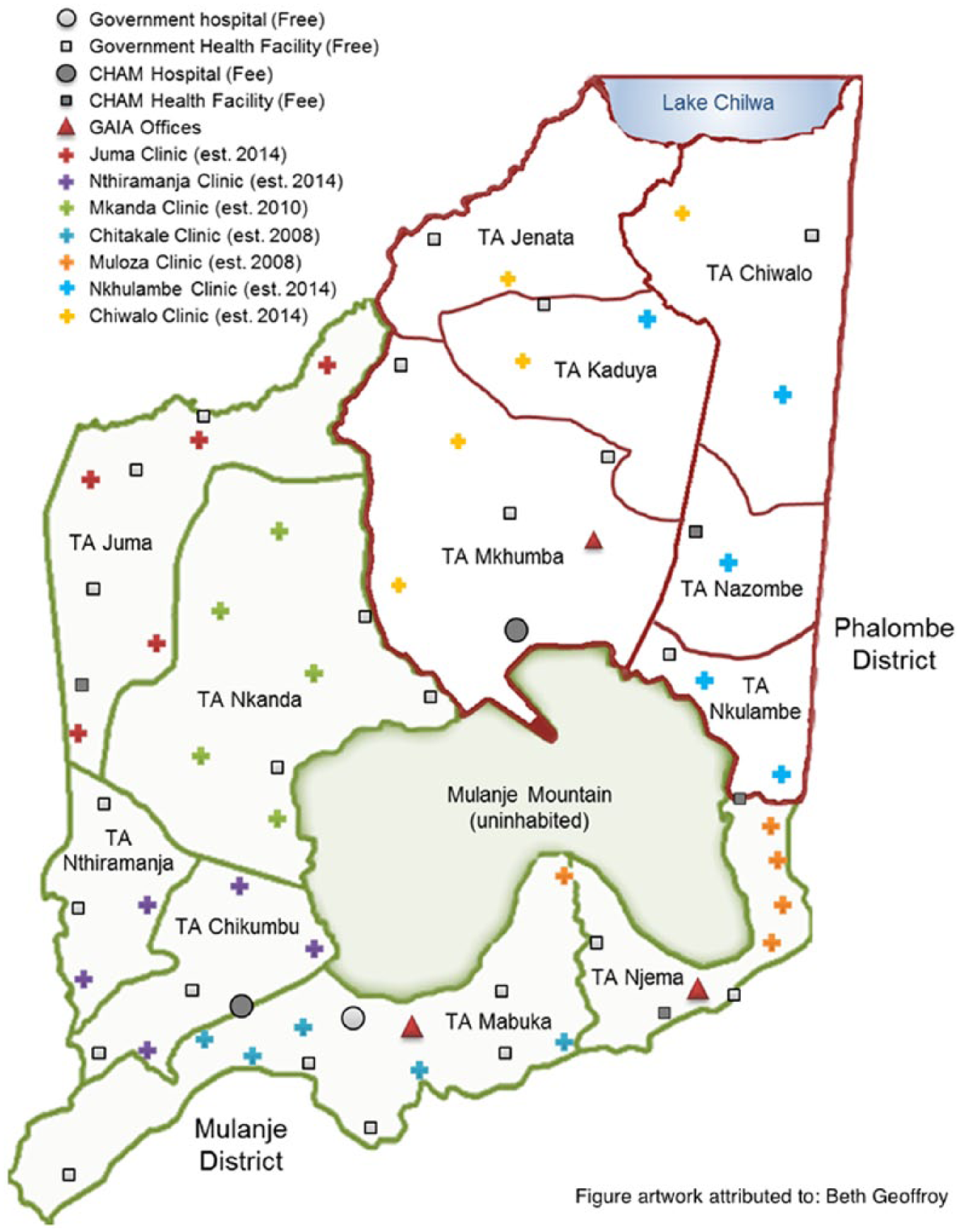
GAIA (Global AIDS Interfaith Alliance) Elizabeth Taylor mobile health clinic sites, government facilities, and Christian Health Association of Malawi (CHAM) facilities in the Mulanje and Phalombe districts of southern Malawi.
A trained, field research team conducted an in-person, follow-up questionnaire at 14 (±2) days after the clinic visit. We determined the patient’s vital status, illness resolution or worsening, and if the patient was hospitalized, referred to another medical facility, lost to follow-up, or withdrawn from the study (Table 1).
Patient Outcome at Follow-up Including Outcome Definition.

The final diagnosis and treatment course were determined by the medical provider and extracted from the clinic logbook. Data were collected on individual diagnoses and medications prescribed and later collapsed into representative categories for ease of reporting. HIV status was ascertained by self-report and was not included in the final logistic regression models given the low reported prevalence. Food insecurity was defined as any member of the household having been hungry and had to skip a meal in the last week. Medication compliance was also self-reported by guardians at follow-up; all medication administration–related questions needed to support compliance to be categorized as compliant.
Because of the focus of this study on patient outcomes, data analysis was restricted to all eligible participants who presented at the clinic and were available for follow-up. Initial data analysis began with univariate descriptive statistics on cohort-level characteristics. Next, bivariate analyses examined the association between patient characteristics and outcomes at follow-up. Continuous exposure variables were compared with t tests or Wilcoxon rank-sum tests where appropriate, and categorical variables were compared with χ2 tests and Fisher’s exact test when observed and expected cell counts merited. A probability < .05 was considered statistically significant. Finally, a descriptive, multivariate logistic regression was fit to explore factors associated with a worsening or unchanged symptom status compared with resolution of symptoms at follow-up. Variables were chosen for inclusion in the multivariate model first based on their empirical significance from the literature (age, sex, and season) and second based on their significance in the data set at the bivariate level to account for cohort-specific variation (household food insecurity, time to a standing clinic, total medication number prescribed, and symptom duration). The inclusion of symptom duration and number of medications prescribed did not significantly improve model fit and were, therefore, not included in the final model. We report odds ratios (ORs) and 95% confidence intervals (CIs) measuring the direction and strength of association for included variables. The final model of best fit was evaluated through goodness-of-fit tests for nested models and Bayesian information criterion for nonnested models. All data analyses were completed using the R statistical package (R Foundation for Statistical Computing, Vienna, Austria, version 3.2.4).
This study was approved by the University of California San Francisco Human Research Protection Program (Approval #16-19187) and the Malawi National Health Sciences Research Committee (Protocol #16/5/1594).
Results
Baseline Characteristics
During the study period, 2893 patients (adults and children) were screened (Figure 2), 489 met inclusion criteria, and 401 were enrolled. Of the enrolled subjects, 286 (67.9%) were children under the age of 14 years, 131 (46.8%) in the dry season and 149 (53.2%) in the wet season. Follow-up was completed in a total of 280 of the 286 (97.9%) children. There were no statistically significant differences seen in the baseline characteristics between the 6 participants who were lost to follow-up and those who remained in the study.
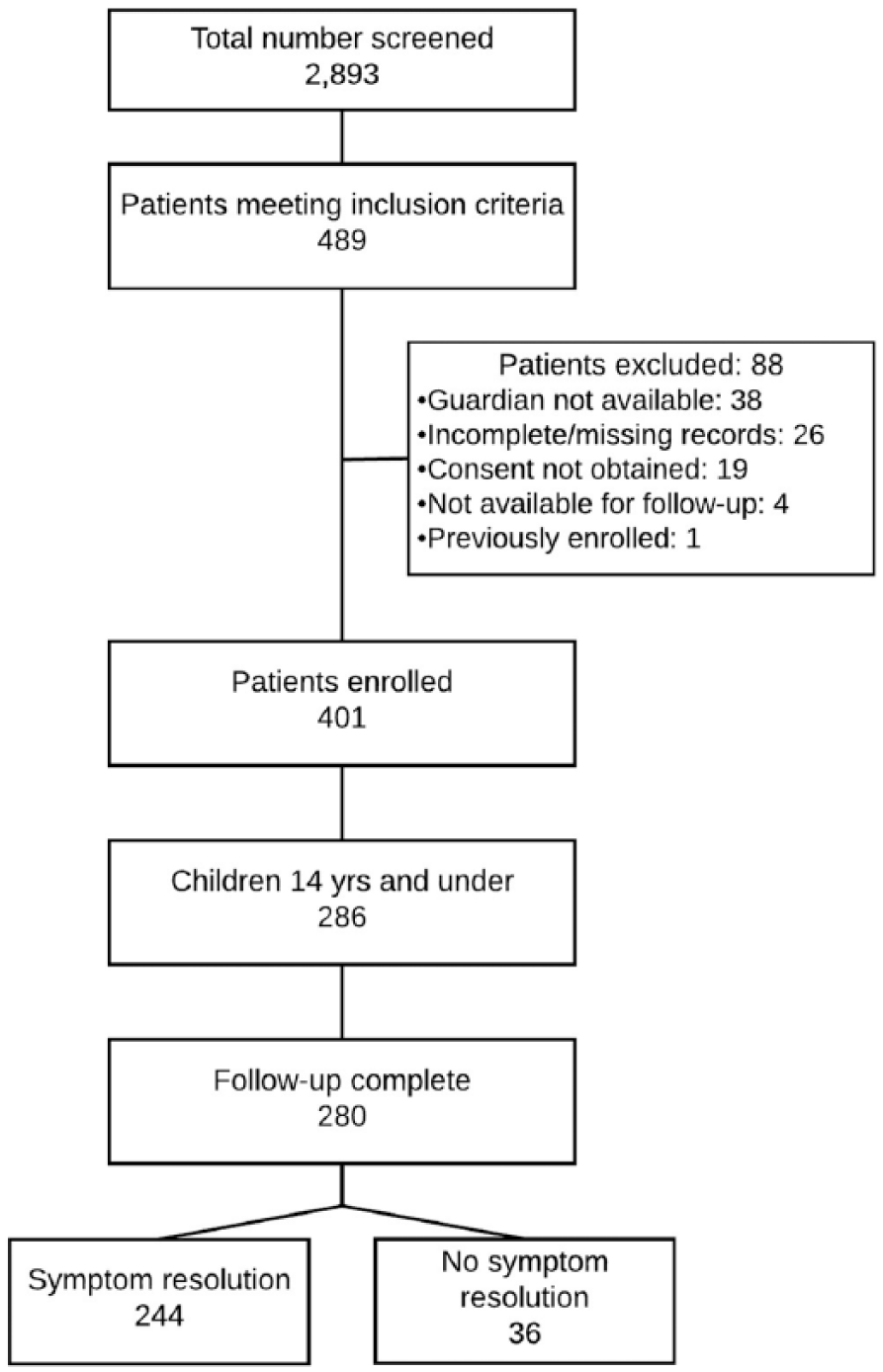
Patient Enrollment Flowchart.
The majority of pediatric patients (n = 177, 61.8%) were under age 5 years and 57.9% (n = 162) were female (Table 2). Ninety-four percent of parental respondents had a primary education level or less (n = 263) and 73% (n = 205) of households relied on manual labor (casual labor or farming) as the primary source of income. More than 65% (n = 183) of families reported some degree of food insecurity in the household, and the majority (n = 171, 61.1%) of households had 5 or more people living in the home. HIV status was reported positive in 1 child, while 257 (91.8%) reported that the status was unknown. Self-reported bednet use was high in this cohort (n = 240, 85.7%).
Baseline Patient Characteristics in Children 14 Years of Age and Under by Outcome.

Abbreviations: IQR, interquartile range; HIV, human immunodeficiency virus; GAIA, Global AIDS Interfaith Alliance; CHAM, Christian Health Association of Malawi.
Almost 95% of patients (n = 265) reported being able to reach a GAIA mobile clinic site in less than 2 hours, while only 54% of patients could reach a standing, permanent clinic (government or Christian Health Association of Malawi clinic [CHAM]) in less than 2 hours. Nearly a quarter of patients (n = 67, 23.9%) reported that they had intentionally delayed seeking care until a GAIA mobile clinic was present, and 113 respondents (40.4%) identified GAIA as their primary care clinic.
Symptoms, Diagnoses, and Treatments
Fever was by far the most common presenting patient complaint (n = 248, 88.6%), followed by cough (n = 108, 38.6%), headache (n = 67, 23.9%), and vomiting (n = 61, 21.8%; Table 3). The most common diagnoses were upper respiratory tract infection (n = 141, 50.3%), fever without a source (n = 66, 23.6%), and gastroenteritis (n = 26, 9.3%).
Differences in Presenting Complaint, Diagnosis, and Treatment in Children 14 Years and Under by Outcome Status.

Abbreviations: URI, upper respiratory tract infection; UTI, urinary tract infection; ORS, oral rehydration solution.
Sum >280 because of multiple complaints.
A majority (90.4%) of participants received a single diagnosis ascribed to their presenting complaint, with only one participant receiving no official diagnosis and the remaining 9.3% receiving 2 diagnoses. The most commonly prescribed medications included the following: analgesics/antipyretics (n = 274, 97.9%), antibiotics (n = 110, 39.3%), topical cream (n = 24, 8.6%), and oral rehydration solution (n = 23, 8.2%). All 280 children received at least one medication, and the vast majority received 2 or more (n = 261, 93.2%). More than three quarters (77.1%) of guardians reported high medication compliance (completed full course, doses given on time, no missed doses).
Outcomes
The majority of participants (n = 244, 87.1%) reported that their child’s symptoms had resolved, while 12.9% (n = 36) reported no resolution and none reported worsening symptoms (Table 1). Of the children who completed follow-up, none died or were hospitalized during and only one child was referred to a higher level of care during the study period. Six patients were lost to follow-up and none withdrew consent. Compared with subjects whose symptoms resolved, those who reported no symptom resolution were significantly more likely to have presented during the dry season (42.6% vs 75.0%, P < .0003), had 2 or more days of symptoms (51.6% vs 72.2%, P = .03), and experienced household food insecurity (62.3% vs 86.1%, P = .007; Table 2). Interestingly, those without symptom resolution were significantly more likely to live 2 or more hours away from a standing clinic (43.0% vs 66.7%, P = .011), but greater time to a GAIA mobile clinic did not affect symptom resolution (4.9% vs 8.3%, P = .42).
There was no statistically significant difference in outcome based on presenting complaint or diagnosis (Table 3). Interestingly, though most guardians believed the diagnosis assigned by the GAIA provider (n = 257, 91.8%), there was a statistically significant difference between those who believed the diagnosis and those that did not and the outcome; those who believed the diagnosis were more likely to improve (95.1% vs 69.4%, P < .0001). Of the medications prescribed, only antihelminthic therapy was statistically significant in regard to outcome, with those receiving treatment more likely to report no resolution (1.6% vs 8.3%, P = .048). Regardless of outcome, there was no significant difference in additional care seeking behavior or medication compliance between subjects with and without symptom resolution (13.1% vs 16.7%, P = .6, and 78.7% vs 66.7%, P = .19, respectively).
Multivariate Logistic Regressions
To better understand the at-risk patient profile, we conducted a multivariate logistic regression; Table 4 shows the unadjusted and adjusted odds ratios (AOR) and corresponding 95% CI. Of the a priori variables, the final model with the best fit showed no significant difference in outcome based on participant sex or age; however, subjects that presented in the dry season had a 4.35 times greater likelihood of having no symptom resolution as compared with subjects who presented during the wet season (95% CI = 1.96-11.11). Household food insecurity and being greater than 2 hours from a permanent clinic were also significantly associated with no improvement in symptoms (AOR = 4.61, 95% CI = 1.81-14.29; and AOR = 2.38, 95% CI = 1.11-5.36, respectively).
Unadjusted and Adjusted Odds Ratio and 95% Confidence Intervals for Odds of Having No Resolution or Worsening of Symptoms Compared With Symptom Resolution in Children ≤14 Years of Age.
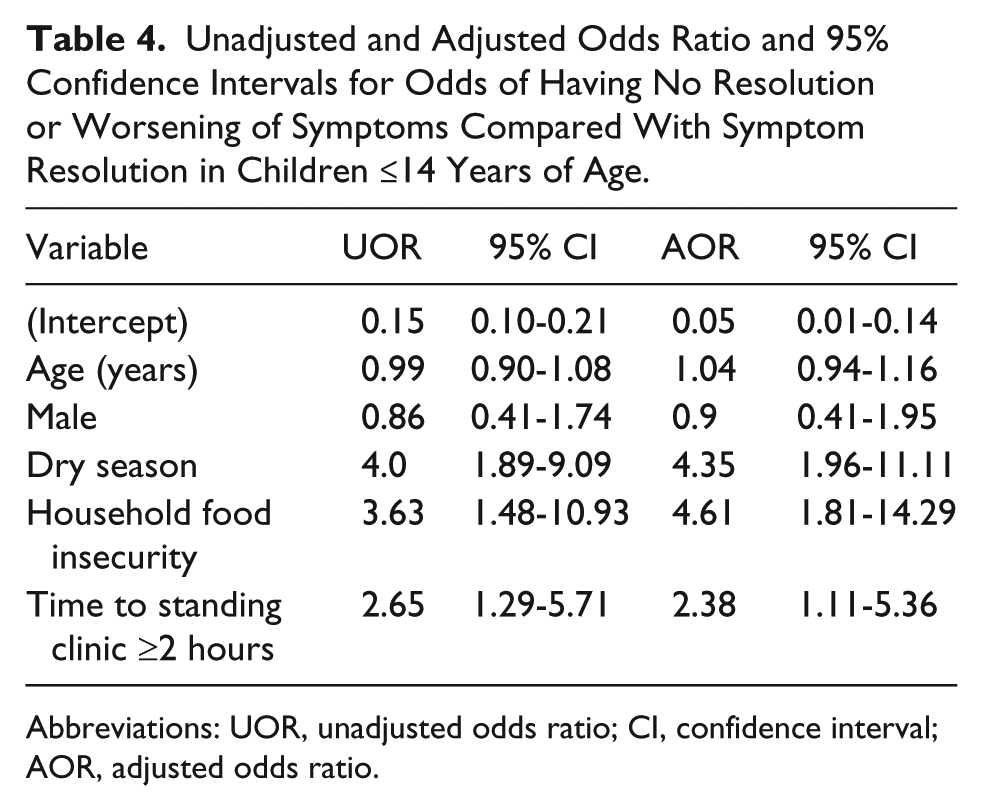
Abbreviations: UOR, unadjusted odds ratio; CI, confidence interval; AOR, adjusted odds ratio.
Discussion
In general, outcomes were excellent in this rural, outpatient pediatric cohort, with no cases of child mortality or hospitalization and 87% of subjects improving. We did identify several key risk factors for nonrecovery, namely, longer time to a standing clinic, food insecurity in the home, and seasonality. The first 2 variables are modifiable; longer time to a standing clinic reflects access to care, and food insecurity relates to socioeconomic status.
Many subjects had to travel more than 2 hours to reach a non-GAIA medical clinic; such limited access can result in delays to definitive care when the mobile clinics are not present. Nearly a quarter of guardians reported delaying care until a mobile clinic was in the area, and in the bivariate analysis, we found that longer symptom duration prior to presentation was associated with a worse outcome. Delays to definitive care have been associated with worse pediatric outcomes in other low-income country settings,7,8 while health system strengthening and improved access to care are associated with improved outcomes.9,10 This finding illustrates not only the critical role GAIA clinics play in the community, but also the need to increase access to care, either by increasing GAIA’s presence and/or increasing the number and accessibility of permanent clinics to minimize delays to care. Further exploration of the reasoning behind guardian-imposed delays in seeking care is critical to better understand the interplay between health seeking behaviors and access to care in this setting.
Food insecurity and malnutrition are common in Malawi under normal conditions, with 37% of children under 5 suffering from stunting. 11 In 2016, during the study period, El Niño–related drought followed by flood resulted in a severe food shortage crisis throughout Malawi that affected more than 40% of the population, requiring the largest emergency food relief operation in Malawi’s history. 12 Food insecurity occurred frequently in the study population, and we observed a strong association between symptom improvement and a lack of food insecurity in the home. This is despite national World Food Programme relief and ongoing, local food supplementation by GAIA during the study period. This finding signifies not only the importance of nutrition to overall health, but also likely reflects lower socioeconomic status and decreased household resource availability in general.13-17 In high-risk populations, such as this cohort, clinics may want to incorporate ongoing nutritional assistance in the medical treatment plan as a reduction in household food insecurity has been shown to improve outcomes in SSA settings.18-20 Food insecurity, health care utilization, and health outcomes are inextricably linked 17 ; a highly effective intervention would need to address not only food resource availability but also economic disparities to improve long-term health outcomes.
Season is an interesting risk factor; patients in this cohort were less likely to improve in the dry season, which is also the coldest season in Malawi. Both pneumonia and influenza prevalence increases during the dry season,21,22 likely because people are indoors and in close contact more often, which increases the spread of respiratory infections and exposure to indoor air pollution. Additional research identifying the etiology of NMF month-by-month is needed to explore this further.
Fever without a source was the second most common diagnosis in this cohort, which draws attention to the lack of diagnostic tools in this rural outpatient setting. Providers are able to quickly and accurately diagnose malaria with mRDTs, but face a difficult diagnostic dilemma when the mRDT result is negative, having very few diagnostic resources apart from the history and physical to determine the cause of an NMF. Despite the diagnostic challenges, providers frequently (39.3%) prescribed antibiotics to febrile children in this study. Without improved diagnostic capabilities, providers are unable to reliably determine which children have viral infections and are likely to improve without antibiotics as compared to children with bacterial infections that require antimicrobial therapy. This is especially important given the global crisis in antimicrobial resistance we are currently facing. 23
There are several limitations to this study. First, HIV status was determined by self-report in this cohort. This cohort had slightly lower HIV rates (0.4%) than the general pediatric (ages 0-14 years) population prevalence in Malawi of 1%,24-26 though 92% reported unknown HIV status. We may have failed to capture a few positive children because of inadequate screening and/or HIV-related stigma that limited the guardian’s willingness to disclose. Second, malnutrition is a known risk factor for poor pediatric outcomes,27-29 but in this observational study we relied on medical documentation for diagnosis and comorbid conditions and did not independently collect anthropometric data to capture the true prevalence of malnutrition in this population. It is possible that children who failed to recover had higher rates of one or both of these comorbid conditions compared with those who recovered; however, overall this cohort had good outcomes regardless of HIV status or malnutrition.
Given the prevalence of NMF in this population and the challenge providers face when deciding how to manage NMF with limited diagnostic tools, future studies should focus on the implementation of cost-effective, high-impact diagnostic tools in resource-limited settings. Similarly, though antibiotics are widely prescribed in this setting, there are extensive surveillance and monitoring limitations, making the true rate of antimicrobial resistance difficult to measure. 23 Further characterization of antimicrobial resistance patterns is desperately needed.
The at-risk pediatric patient profile in rural Malawi includes food insecurity and limited access to care, especially during the dry season, none of which are unique to this setting or country. The results of this study can help guide local medical providers to identify children at risk of not improving and target these patients for follow-up and possibly early referral. Additionally, interventions in the clinical setting that screen for and address household food insecurity could greatly affect child health outcomes. Ideally, these results will inform policy-level changes aimed at addressing these key, modifiable risk factors, not only in Malawi but also throughout rural areas of SSA. Health is a complex interaction of acute illness, socioeconomic factors, access to care, and comorbid conditions. Effective, sustainable health interventions must focus on all aspects to truly make a lasting impact on outcomes.
Footnotes
Acknowledgements
The authors would like to thank the research team at ENANDY, the District Health Officers in the Mulanje and Phalombe Districts for their support, and the GAIA health providers and patients for providing valuable insights and access for this work.
Author Contributions
TBK: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AB: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ES: Contributed to conception and design; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
GB: Contributed to conception and design; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ES: Contributed to conception and design; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SR: Contributed to conception and design; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
KB: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AM: Contributed to acquisition, analysis, and interpretation; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was supported by funds from the University of California, San Francisco, School of Nursing and Resource Allocation Program.