
Abstract
Objective: A study to compare the usage of throat swab testing for leukocyte esterase on a test strip(urine dip stick-multi stick) to rapid strep test for rapid diagnosis of Group A Beta hemolytic streptococci in cases of acute pharyngitis in children. Hypothesis: The testing of throat swab for leukocyte esterase on test strip currently used for urine testing may be used to detect throat infection and might be as useful as rapid strep. Methods: All patients who come with a complaint of sore throat and fever were examined clinically for erythema of pharynx, tonsils and also for any exudates. Informed consent was obtained from the parents and assent from the subjects. 3 swabs were taken from pharyngo-tonsillar region, testing for culture, rapid strep & Leukocyte Esterase. Results: Total number is 100. Cultures 9(+); for rapid strep== 84(-) and16 (+); For LE== 80(-) and 20(+) Statistics: From data configuration Rapid Strep versus LE test don’t seem to be a random (independent) assignment but extremely aligned. The Statistical results show rapid and LE show very agreeable results. Calculated Value of Chi Squared Exceeds Tabulated under 1 Degree Of Freedom (P<.0.0001) reject Null Hypothesis and Conclude Alternative Conclusions: Leukocyte esterase on throat swab is as useful as rapid strep test for rapid diagnosis of strep pharyngitis on test strip currently used for urine dip stick causing acute pharyngitis in children.
Background
The typical symptoms of streptococcal pharyngitis are sore throat, fever of greater than 38°C, tonsillar exudates, and enlarged tender cervical lymph nodes. Other symptoms include headache, nausea, vomiting, abdominal pain, muscle ache, scarlatiniform rash, and petechiae on the palate. The diagnosis of strep throat is unlikely with symptoms of red eyes, hoarseness, runny nose, or mouth ulcers. It is also less likely in the absence of fever. The most common bacterial organism causing acute pharyngitis in children is group A β-hemolytic streptococci. Other bacteria such as non–group A β-hemolytic streptococci and Fusobacterium may also cause pharyngitis 1 but is insignificant.
Our study used the modified Centor Criteria, which have been widely accepted in the literature for evaluation and management of acute streptococcal pharyngitis. Each of the criteria was assigned a point. 2
In streptococcal pharyngitis, the local lesions are characterized by edema, hyperemia, and infiltration of polymorphonuclear leukocytes. 3 We used the idea of leukocyte response in the pharyngotonsillar region to screen for the presence of leukocytes by using the leukocyte esterase (LE) test portion of urine multistick. In the leukocyte area of the dipstick, the presence of granulocyte esterases is revealed by change of color to purple. The esterase cleaves a de-revitalized pyrazole amino acid ester to liberate de-revitalized hydroxyl pyrazole. This pyrazole then reacts with dizonium salt to produce a purple color. The test is capable of detecting trace levels as low as l5 WBCs/µL. 4
The aim of this study was to compare the usefulness of the LE test versus the rapid strep in the screening of group A streptococcal pharyngotonsillitis.
Methods
After obtaining the signed informed consent from the parents and/or assent forms from the subjects, 3 swabs were used for each subject. The first throat swab was used for the culture, the second swab for rapid reagent strep testing, and the third swab was used for the LE test, smeared over the LE testing area of the multistick test strip. No patient was given any antibiotic on the first day till the culture result was obtained. The patients were advised to use saline gurgles and analgesics. All the patients with positive cultures were called back for antibiotics. None of the patients developed any suppurative complications such as peritonsilar abscess, and on follow-up none of the patients had rheumatic fever.
Results
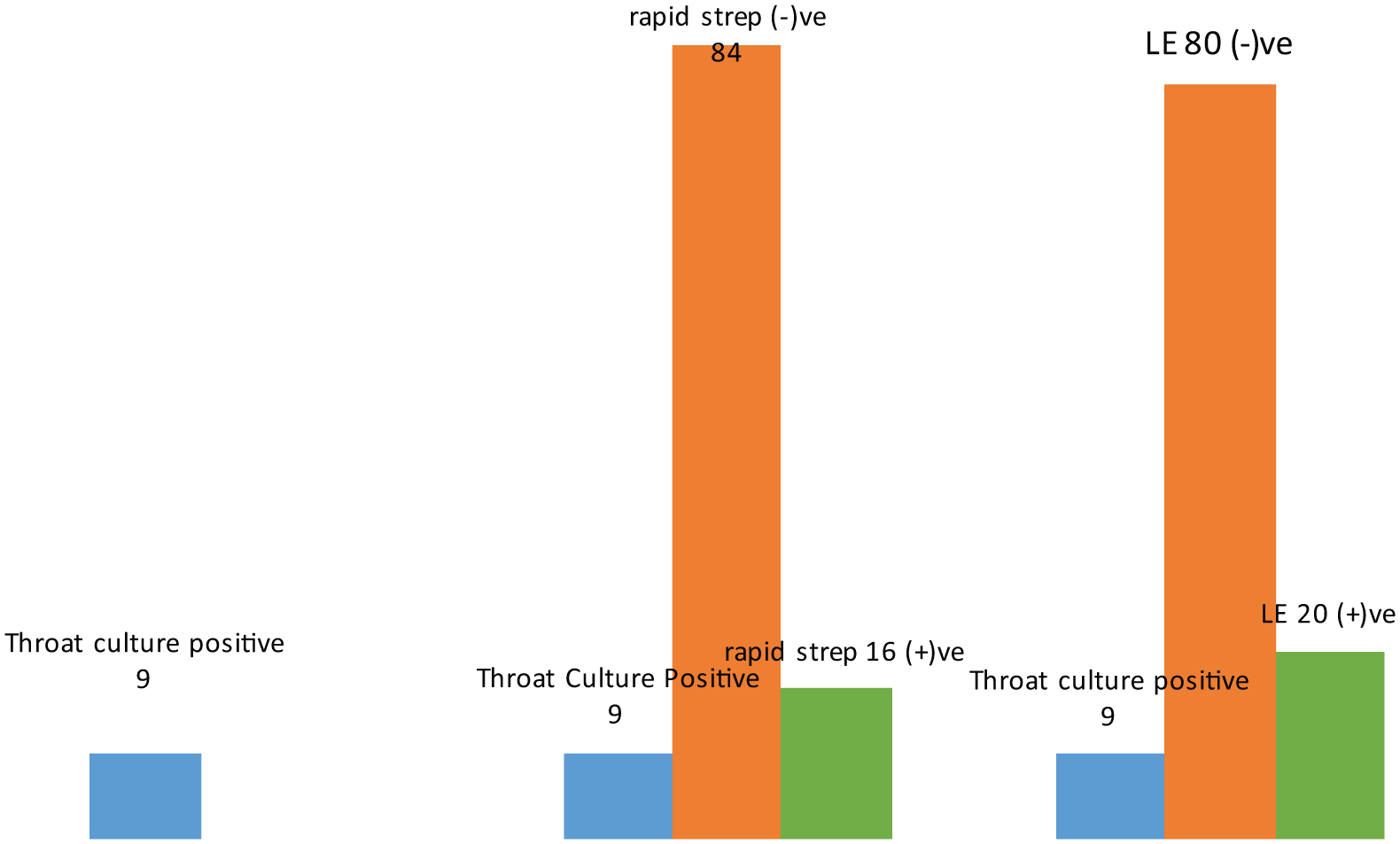
This is an institutional review board–approved prospective study. The sample size was 100, of which 9 had cultures positive for group A β-hemolytic strep. Among those for whom the rapid reagent strep test done, 84 out of 100 were negative and 16 were positive. For the LE test, 80 out of 100 were negative and 20 tested positive (see Table 1 and Figure 1).
The Results Obtained.

Abbreviation: LE, leukocyte esterase
The test results.
Statistics
Rapid Versus LE Test
The contingency table is presented below. It is seen that data configuration does not seem to be random (independent) assignment but extremely aligned.
Contingency Table (Rapid Versus LE).

Metrics of Interest
Keeping outcome as the “event” to occur, “rapid” results are the original “true” event results and the LE results are the matching event results. Thus, rapid being positive and LE being positive is the “True Positive” (TP) event for LE; rapid being positive and LE being negative is the “False Negative” (FN) event for LE; the rapid being negative and LE being negative is the “True Negative” (TN) for LE; and rapid being negative and LE being positive is the “False Positive” (FP) event for LE.
Under this context,
Sensitivity = TP/(TP + FN) = 13/(13 + 3) = 81.25%
Specificity = TN/(TN + FP) = 76/(76 + 8) = 90.48%
Positive Predictive Value = TP/(TP + FP) = 13/(13 + 8) = 61.90%
Negative Predictive Value = TN/(TN + FN) = 76/(76 + 3) = 96.2
Odds Ratio = (TP/FP)/(FN/TN) = (13/8)/(3/76) = 41.166 = High value formulation
Null Hypothesis = Outcomes under rapid and LE are independent (not correlated)
Alternate Hypothesis = Outcomes under rapid and LE are not uncorrelated
Test Statistic = Under null hypothesis sum across all the cells of (Observed frequency − Expected frequency)**2/(Expected frequency).
The statistical results show rapid and LE show very agreeable results. Calculated value of χ2 exceeds tabulated under 1 degree of freedom (P < .0001); reject null hypothesis and conclude alternative.
Discussion
Modified diagnostic criteria have been widely used for the evaluation and management of strep pharyngitis. The modified Centor criteria are listed below. One point is assigned to each when present. 2
Absence of cough
Swollen and tender cervical lymph nodes
Temperature >23°C
Tonsillar exudate or swelling
Age less than 15 years (3-14 years).
In our study, we included all the Centor criteria. We have also observed for other signs and symptoms, such as erythematous tonsils or pharynx, palatal hemorrhages, abdominal pain, and skin rash. We have noticed that only 7 out of 20 patients who had exudates had throat culture positive for strep. Of those patients who had palatal hemorrhages, 6 out of 8 had strep positive. Acute bacterial pharyngitis in children is most commonly caused by group A β-hemolytic streptococcus. Other bacteria such as non–group A β-hemolytic streptococci and Fusobacterium may also cause pharyngitis. The rationale behind treating strep is to prevent rheumatic fever and local suppurative complications. Acute pharyngitis of viral etiology is more common than bacterial infections in children. Viral throat infections in addition to sore throat present with other symptoms and signs such as cough, nasal discharge, diarrhea, and fever. Laboratory testing remains the mainstay for diagnosis of strep throat. A throat culture is the gold standard for the diagnosis of strep pharyngitis. A rapid strep test is also considered to be sufficient to establish the diagnosis of strep pharyngitis.
Shaikh and his colleagues, 5 after reviewing 15 articles, say that no individual symptoms or signs were effective in confirming streptococcal pharyngitis. They suggest symptoms and signs either individually or combined into predictive indicators cannot be used to definitely diagnose or rule out streptococcal pharyngitis.
Laboratory testing such as throat culture and rapid strep testing remain the mainstay of diagnosis and management of acute strep pharyngitis. Maltezou et al 6 studied the usefulness of the rapid antigen detection test (RADT) in the diagnosis of streptococcal pharyngitis in children and its impact on antibiotic prescription. They found that the RADT will provide appropriate guidance to treat strep throat infections and reduce unnecessary cultures and usage of antibiotics. Bryars et al 7 found increased usage of antibiotics where RADTs were used. They compared this observation to centers with decreased usage of antibiotics, where RADTs were not available for cases of acute pharyngitis. Anderson and his group, 8 in their multicenter study, studied the usage of streptococcus DNA amplification assay for detection of group A strep from pharyngeal swabs. They found that illumigene group A strep DNA amplification assay was useful with a sensitivity of 99.0% and specificity of 99.6%. Again, the ESCMID Group 9 has updated guidelines to diagnose and treat patients with strep throat. They suggested the usage of Centor scoring and rapid antigen test and recommended not to use antibiotics with Centor score of 0 to 2. They have also suggested that the usage of antibiotics is unnecessary as suppurative complications are infrequent with these scores.
Some conflicting studies have emerged regarding usage of antigens in adults. Nakhoul and Hickner 10 have questioned the benefit of routine DNA probe backup testing in adults because of its cost. They found a high rate of inappropriate antibiotic administration. Similarly, Forward and his group 11 studied a comparison between the strep A rapid test device and conventional culture for the diagnosis of strep pharyngitis. They found that in cases of strep pharyngitis the rapid strep test has a sensitivity of 72% only, as compared to previously quoted studies. 8 Shulman and colleagues 12 do not agree with routine antibiotic treatment. Antibiotics are recommended only after appropriate positive testing.
Strep pharyngitis is treated with antibiotics. The usual antibiotics are penicillin or amoxicillin or IM benzathine penicillin G. For patients allergic to penicillin, erythromycin and other macrolides or clindamycin are recommended. Treatment of carriers is not recommended. If pharyngitis occurs more than 3 times in a year, surgical intervention such as tonsillectomy is recommended. 13
In streptococcal pharyngitis, the local lesions are characterized by edema, hyperemia, and infiltration of polymorphonuclear leukocytes. 3 This leukocytic response is detected by using an LE strip, thus providing an initial screening tool. In the leukocyte area of the dipstick, presence of granulocyte esterases is revealed by a change of color to purple. The esterase cleaves a de-revitalized pyrazole amino acid ester to liberate de-revitalized hydroxyl pyrazole. This pyrazole then reacts with dizonium salt to produce a purple color. The test is capable of detecting trace levels as low as l5 WBCs/µL. 4
Joshi and his group 14 conducted a study to determine the usage of urine reagent strip for semiquantitative assessment of protein, glucose, and presence of LE in cerebrospinal fluid. They conclude that the existing reagent strip can be used to diagnose meningitis in low-resource settings. Another study by Farahmand and his colleagues 15 studied the effectiveness of dipstick (LE and nitrite) for the diagnosis of bacterial peritonitis in cirrhotic patients. They found that the sensitivity, specificity, and positive and negative predictive values of LE reagent may prove to be a rapid bedside diagnostic test for the diagnosis of spontaneous bacterial peritonitis in cirrhotic patients. Kelly and her colleagues 16 also studied the usage of LE in rapid diagnosis of septic arthritis and found that the LE test is very useful for rapid diagnosis of septic arthritis.
Our study has utilized the LE test as a rapid screening test similar to the rapid strep test. In streptococcal pharyngitis, an early polymorphonuclear response happens in the pharyngotonsillar region. 3 We used this idea of leukocyte response in the pharyngotonsillar region to screen for the presence of leukocytes, by using the LE test in urine multistick test strip. The goal of our study was to compare the efficacy of the LE test with the rapid strep test in the screening of group A strep pharyngotonsillitis. The swab as described earlier is smeared onto the leukocyte portion of the multistick to detect the presence of leukocytes. Our study confirms that the LE test may be as useful a screening test as the RADT. Ours is the first study evaluating the usefulness of the LE test as a screening test for group A strep pharyngitis. It has a definite cost advantage over the rapid strep test. Hence, the LE test may be considered as a preferred screening test for rapid diagnosis.
Conclusions
The throat swab testing for LE on the test strip currently used for urine dipstick may be as useful as the reagent strep test in screening for group A β-hemolytic streptococcal infections causing acute pharyngitis in children. In terms of cost-effectiveness, the LE test performed with a throat swab may be more cost-saving as it costs only 10 cents for a multistick strip compared to $4 or $5 for a single rapid strep test for rapid diagnosis of strep pharyngitis.
Footnotes
Acknowledgements
Statistical help was obtained from P. J. Krishnan, PhD, statistics.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.