
Abstract
Disease knowledge, illness perceptions, and quality of life (QOL) were examined in 150 adolescents (mean age = 16.1 years, SD = 1.9; 49.3% males) with sickle cell disease (SCD). Females had higher knowledge (P = .004), lower QOL (P = .02), and perceived their illness to be more unpredictable (P = .03). Those with more severe disease perceived their illness to be unpredictable with worse outcomes. Those with higher knowledge scores perceived their illness to be chronic, made more sense of their illness, and perceived greater personal and treatment control. Final hierarchical regression model showed that secondary education as compared to primary education level (P < .001) was positively correlated whereas disease severity (P < .001), perceived unpredictability (P = .024), and negative emotions (P < .001) were negatively correlated with QOL. Health practitioners should assess adolescents’ illness perceptions and encouraging continuing schooling and addressing emotional/psychological problems could improve their QOL.
Introduction
As persons are faced with the diagnosis of an illness or experience a health condition, they will seek to make sense of and then manage this illness by using their own past knowledge, experiences, and beliefs, and also including those of others in their communities of home, work, and other social places. 1 The patients’ cognitive and emotional representations of their illness are their illness perceptions. The common sense model (CSM) of self-regulation framework describes the theory that illness perceptions could mediate patients’ coping strategies and affect psychological outcomes such as anxiety, depression, and quality of life (QOL)2,3 and even behavioral and physical outcomes such as medication adherence4,5 and glycemic control. 6 Illness perceptions are modelled based on 5 dimensions: identity, consequences, timelines, control/cure, and cause.3,7 This model has been used to describe illness perceptions across a range of ailments such as arthritis, cancer, psoriasis, pulmonary diseases, and diabetes.2,6,8-10
These illness perceptions continue to develop and adjust as the patient undergoes daily experiences living with his/her illness, especially a chronic illness. Patients may have vastly different perceptions of the same illness and therefore respond with different behaviors that will in turn lead to different outcomes. 1 Despite this understanding, patients’ own perceptions are seldom sought during consultations and the result can be the doctor’s own understanding of the patient’s illness experience being limited and hence poorer outcomes for the patient. Indeed, modifying patients’ negative illness perceptions early in the disease course could lead to quicker recovery. 11
Illness perceptions of adolescents with chronic illnesses are not as well understood. As adolescents develop and mature cognitively and socioemotionally and become more involved in managing their condition, 6 their illness perceptions may change and will play a greater role in disease control.12,13 In a few earlier studies, adolescents’ beliefs have been found to be predictors of HBA1c levels 14 as well as psychosocial well-being. 15
The Adolescent With Sickle Cell Disease
Sickle cell disease (SCD) is one of the most common genetic disorders worldwide. It is a chronic, lifelong disorder characterized by multiple physical and psychosocial complications for those afflicted but also presents many challenges for families, communities, and health care systems. 16
The child with SCD entering adolescence not only needs to navigate the usual challenges facing all adolescents at this time-,such as identity formation, physical and social explorations, and increased risk-taking behaviours,17-19 but also the numerous other problems that their illness exposes them to. Typically, SCD can cause school absenteeism and at times lower academic performance,20,21 and delays in physical growth and sexual maturation, 22 with consequent effects on body image.23,24 Adolescents with SCD continually engage in risky behaviors such as alcohol use and unprotected sexual activity,25,26 even though the effects of these risky behaviors can be more severe due to the presence of their chronic illness. 27 They face multiple psychosocial problems such as depression, poorer QOL, social isolation, and maladjustments.28-33 This is the time when they face challenges as they transition their health care from pediatric to adult care and become more independent in managing their disease.34-37
How these adolescents perceive and therefore respond to their illness is critical to facilitate positive outcomes. With more positive illness perceptions, persons are better able to self-manage,14,38,39 and studies have shown the benefits of self-management: when patients are responsible for managing their own illness, their clinical outcomes and QOL improve and they become less dependent on health care services.39,40
SCD Disease Knowledge
Knowledge of disease may also be beneficial for patient outcomes, and effects of SCD knowledge has been explored previously in a few studies. Patients have described using means to increase their knowledge to allow them better control and awareness of their illness. 41 Patients with higher motivation state that they see the need for more knowledge, which enable them especially in negotiating for hospital care. 42 Studies with adolescents and children have shown that when their caregivers have greater understanding of their disease there is association with more positive disease outcomes and improved adaptive coping and disease management in the children.30,43,44 Even though we have identified gaps in knowledge of our adolescents with SCD, 45 our study reported that those with higher knowledge had more positive health beliefs. Studies describing the effects of disease knowledge on patients’ QOL are however inconsistent,46-48 and in fact disease knowledge offers but a fraction of what will constitute self-management skills of a person living with a chronic disease. 49 Information on the relationship between illness perceptions and disease knowledge is scant, but they might have an additive effect on disease outcomes. 50
Little is known either about the illness perceptions among adolescents with SCD and their effect on disease outcomes or about the relationship between their disease knowledge and illness perceptions. This article examines the relationships between sociodemographic variables, disease severity, disease knowledge, illness perceptions, and QOL in adolescents with SCD. We hypothesize that sociodemographics, higher disease knowledge, and positive illness perceptions will be positively associated with QOL and higher disease severity will be associated with poorer QOL.
Methods
Study Design and Procedures
This article reports on baseline data from a completed randomized controlled trial that assessed the effects of an education and counselling intervention on disease knowledge (the “Know-IT study” registered at www.clinicaltrials.gov with the trial registration identifier number NCT01945073) in a cohort of adolescents with SCD. The study was granted ethical approval by the University of the West Indies Ethics Committee.
Between August 2013 and January 2014, adolescents attending the Sickle Cell Unit (SCU) in Jamaica were recruited if they were presenting for routine, well visits and had no history of a neurological disorder, for example, past stroke. A study coordinator, who was not involved in any way directly with clinical care of persons with SCD, approached adolescents and their parent/caregiver in clinic and the objectives of the study were explained. Written informed consent (with parental consent and child’s assent as appropriate for those less than 16 years of age) was obtained from all participants.
Each participant independently completed an interviewer-administered questionnaire in a private, quiet room at the SCU, which included information on sociodemographics, SCD severity, knowledge of SCD, the Revised Illness Perception Questionnaire (IPQ-R), and the Pediatric Quality of Life Inventory Sickle Cell Disease Module (PedsQL-SCD–Teen Modules). The questionnaires had been piloted prior to use in the study.
Measures
Sociodemographic Variables
Crowding was defined as the ratio of number of persons living in the home and number of rooms in the home (excluding kitchen and bathrooms). Household possessions were calculated as a sum of main items available in the home such as television, car, computer, washing machine, and so on. Both crowding and household possessions indices were used as proxy measures for socioeconomic status. Other variables included genotype, sex, age, and educational attainment.
SCD Severity Assessment
A composite severity score was calculated based on responses to 3 questions: frequency of pain events, hospital admissions for SCD-related complications, and clinic attendance. Each item was scored on a 5-point Likert-type scale, and higher scores indicate greater severity of disease.
SCD Knowledge Questionnaire
The 24-item SCD knowledge questionnaire used was a slightly modified version of the one that has been developed for use among adolescents at our unit, based mainly on expert opinion. 45 It includes items that focus on adolescents’ understanding of genetics and inheritance of SCD, clinical manifestations and complications of the disease, fertility issues, and pathological mechanisms. Higher scores imply greater disease knowledge. Cronbach’s α reporting internal consistency reliability for the 24-item knowledge questionnaire was .85.
Pediatric Quality of Life Inventory Sickle Cell Disease Module
The 43-item PedsQL Sickle Cell Disease Module (teen form for ages 13-18 years) was used to assess QOL in this study. It is shown to have excellent feasibility and reliabilities on both the teen and parent-proxy forms. The items are rated on a 5-point Likert-type scale from “Never” to “Almost always” and scored into 9 dimensions. Total scores for each subscale can be calculated by summing all item responses and dividing by the number of items answered. 51 A total score is calculated by summing all the items over the number of items answered on all scales.
The PedsQL SCD Module has been validated for use in our population of adolescents with SCD, 52 and the teen form has a Cronbach’s α of .96, with subscale reliabilities ranging from .70 to .93.
Illness Perception Questionnaire–Revised
The IPQ-R is divided into 3 subsections. 53 The first section consists of questions related to 14 common symptoms and forms the “identity” (number of symptoms attributed to the illness) subscale. The second section has 38 items and is scored on a 5-point Likert-type scale. These are collated to produce 7 subscales, labelled timeline acute/chronic (the perception that his/her illness is chronic/long lasting), timeline cyclical (the perception that their illness is of a cyclical nature, ie, it fluctuates in its symptoms and varies over time), consequences (the perception that his/her illness will have serious negative effects/consequences on his/her life), personal control (the degree to which a person feels able to control his/her illness and its effects), treatment control (perceptions of how effective treatment or medical personnel may be in controlling his/her illness), illness coherence (the extent to which a person understands his/her illness), and emotional representations (the extent to which the person has feelings of anger, anxiety, or depression resulting from his/her illness).53,54 The identity, consequences, timeline acute/chronic, and timeline cyclical dimensions are considered “negative” beliefs of illness perceptions, whereas high scores on the illness coherence, personal, and treatment control dimensions represent “positive” beliefs or illness perceptions of an individual regarding his/her illness. Higher scores on emotional representations dimension imply a greater psychological burden.
The third section has 18 causal items that on factor analysis load into 4 factors: psychological attributions, risk factors, immunity, and accident/chance. The internal reliability coefficients range from .79 for the timeline cyclical domain to .89 for the timeline (acute/chronic) domain. 53
The scale has been validated in our population also 52 and has robust psychometric properties. Cronbach’s αs range from .56 to .79 (except .34 for treatment control), and the causal items yielded a 3-factor structure explaining 52.1% of the total variance.
Statistical Analyses
All analyses were performed using the statistical software STATA 14.0. Descriptive statistics (means ± SD, median and interquartile ranges, and frequencies as appropriate) were used to describe the study sample with regard to baseline characteristics, stratified by sex. Pearson’s correlations were performed to estimate the relationships between key variables.
Hierarchical regression analysis was performed to determine if clinical disease severity, disease knowledge, and illness perceptions through its dimensions contribute to QOL of adolescents with SCD. The demographic predictor variables, age, gender, and educational status were block entered in step 1, disease knowledge in step 2, clinical disease severity score in step 3, and all illness perception dimensions were entered in step 4. All variance inflation factors were noted to be <2, indicating that multicollinearity was not a bias for the regression models. Statistical significance was set at P value <.05.
Results
A total of 150 adolescents were recruited. Overall, the mean age was 16.1 years (SD = 1.9) and 74 (49.3%) were males. One hundred and fifteen (76.7%) had homozygous hemoglobin SS disease and 30 (20%) had the heterozygous hemoglobin SC disease. Two thirds (68%) were living in urban areas and 125 (83.3%) were currently in school. The mean knowledge score was 14.3 ± 4.3 (range = 5-23), the mean severity score was 5.7 ± 1.7 (range = 3-14), and the mean QOL score was 73.6 ± 19.0 (range = 26.7-100). Table 1 reports on sociodemographics and main explanatory and outcome variables by sex. Females were significantly older (16.4 ± 0.20 vs 15.7 ± 0.23; P = .04), had higher knowledge scores (15.3 ± 4.2 vs 13.3 ± 4.2; P = .004), lower QOL score (70.1 ± 19.6 vs 77.2 ± 17.8; P = .02) and perceived their illness to have a more cyclical timeline (21.5 ± 4.7 vs 19.9 ± 4.9; P = .03). There were no other significant differences in sociodemographics, disease severity, or illness perception dimensions between the 2 sexes.
Basic Characteristics by Sex.
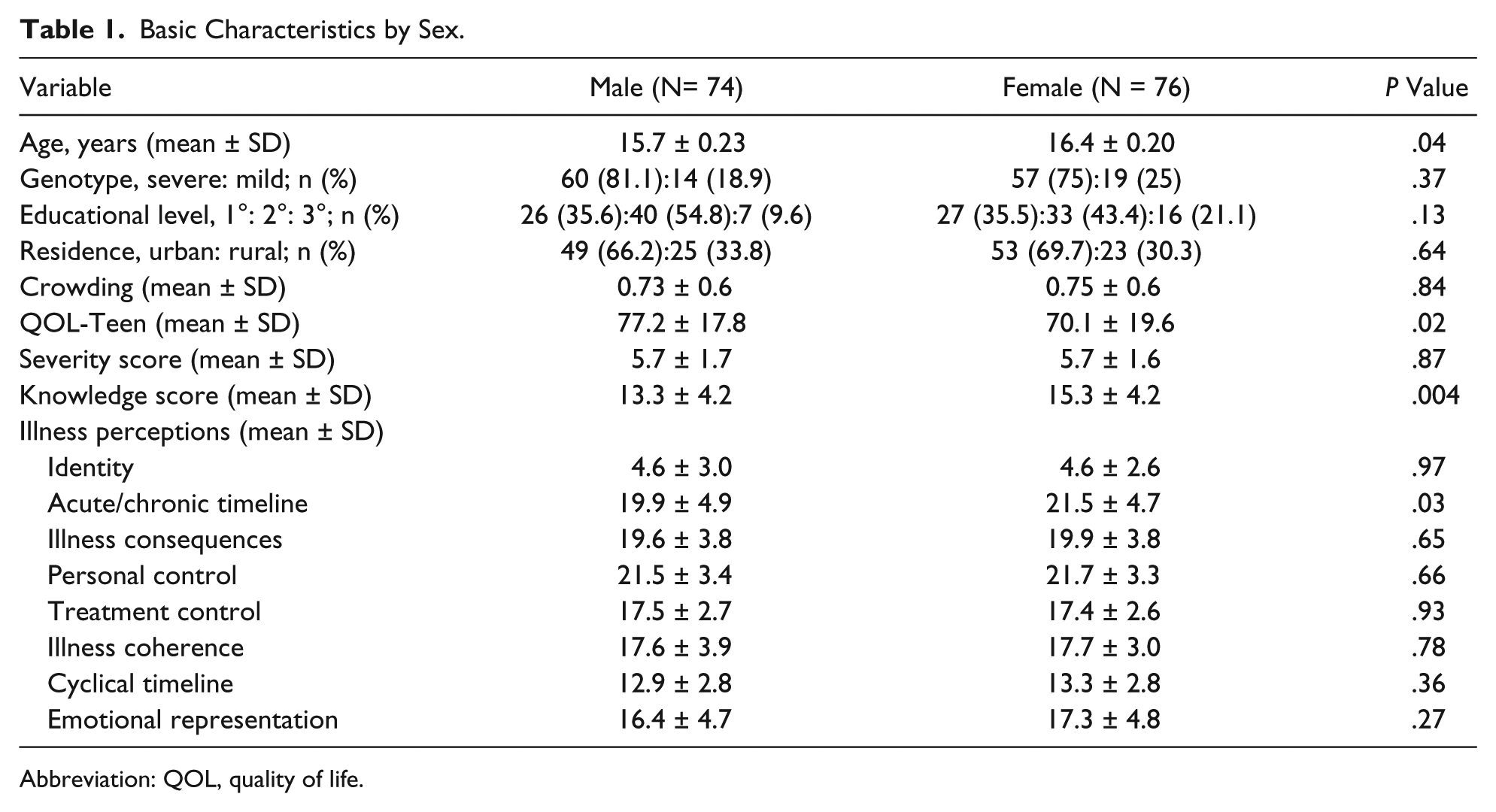
Abbreviation: QOL, quality of life.
Pearson’s Correlations Between Key Variables
Table 2 reports on the pairwise Pearson’s correlation coefficients between all key study variables including sociodemographic variables, disease severity, disease knowledge, illness perception dimensions, and QOL. The teens’ QOL showed significant negative correlations with disease severity, higher symptoms burden (Identity), greater consequences perceived, cyclical timeline, and emotional representation dimensions and positive correlation with illness coherence. Significant associations were seen with sociodemographic indicators. Older age correlated with higher knowledge, higher perceptions of illness being chronic in nature, greater illness coherence, and higher perceived personal and treatment control. Those living in more crowded homes perceived their illness to have more severe consequences and perceived lower personal control over their illness. Those with higher numbers of household possessions had higher knowledge scores and perceived higher personal and treatment control over their illness.
Correlations Between Key Study Variables a .
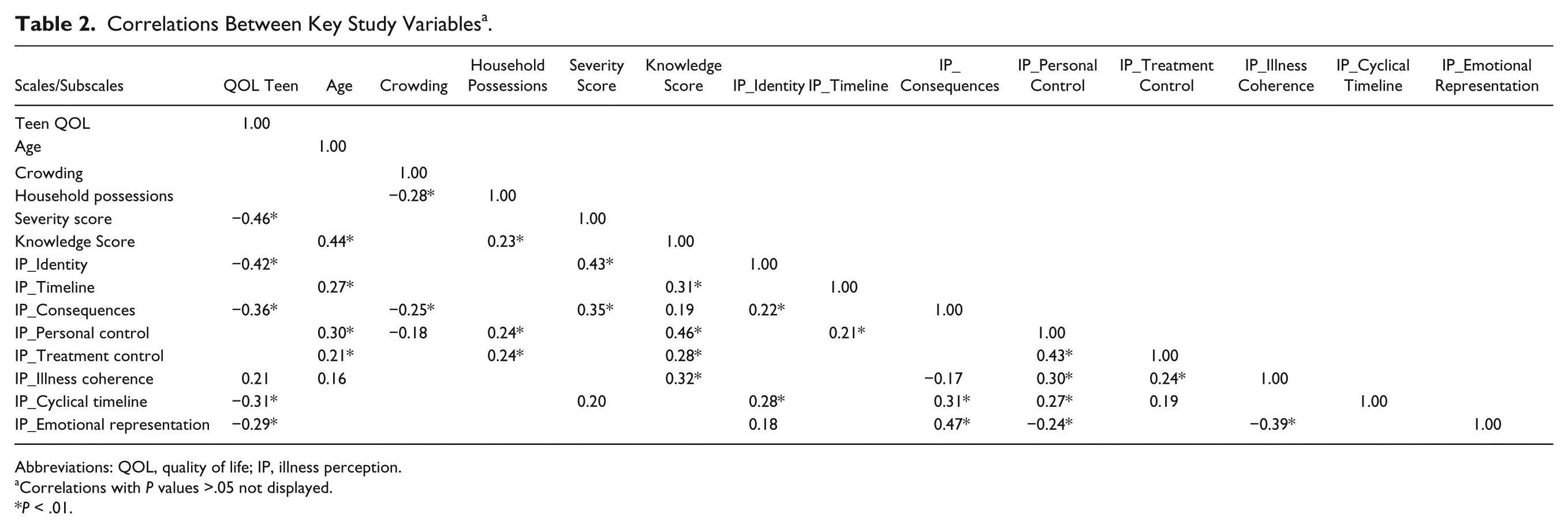
Abbreviations: QOL, quality of life; IP, illness perception.
Correlations with P values >.05 not displayed.
P < .01.
Higher disease severity scores were positively correlated with higher symptom burden, higher perceptions of greater consequences of the illness, and the perception that the illness timeline was cyclical. Higher knowledge scores correlated positively with higher perceptions of the illness having an acute/chronic timeline, greater consequences, greater illness coherence, and greater personal and treatment control.
Of note, emotional representations showed the only significant correlation with QOL, and no correlations with sociodemographic indicators, disease severity, or disease knowledge.
Hierarchical Regression Analysis
The results of the hierarchical regression predicting adolescent’s QOL are reported in Table 3. The results of step 1 indicated that the variance accounted for by the demographic predictors (age, gender, and educational status) equaled 0.14 (adjusted R2 = .11), which was significantly different from zero (F[4,143] = 5.73, P = .0003). In the next step, when knowledge score was added to the model, the change of variance was .015, which was not a statistically significant change over model 1 (ΔF[1,142] = 2.49, P = .117). In step 3, the entry of the variable “severity score” increased the variance of the model by 0.186, which was a statistically significant change (ΔF[1,141] = 39.54, P < .001). The final model, with the addition of all illness perception dimensions, also increased the variance by a change of 0.121, which was again statistically significant (ΔF[7,134] = 4.27, P < .001).
Hierarchical Regression Analysis Evaluating Predictors of Quality of Life of Adolescents With SCD a .

Abbreviation: SCD, sickle cell disease; df, degrees of freedom.
Betas reported are those from the step at which the variable was entered into the model.
Reference category is “Male Sex.”
Reference category is “Primary Education.”
P < .001. *P < .05.
The final model accounted for a total variance of 0.46 (adjusted R2 = 0.41). In the final model, secondary education as compared to primary education level (β = 15.2; confidence interval [CI] = 8.0 to 22.4; P < .001) had significant positive association with QOL, whereas disease severity (β = −4.9; CI = −6.5 to −3.4; P < .001), cyclical timeline perceptions (β = −1.13; CI = −2.11 to −0.15; P = .024), and emotional representations (β = −0.65; CI = −1.24 to −0.06; P < .001) all had significant negative associations with QOL.
Discussion
The current study is one of the very few that report on the illness perceptions among persons with SCD and explores the relationships of QOL with illness perceptions. We have reported that QOL of adolescents with SCD is lower in those with more severe disease and is associated with their illness perceptions; that is, it is lower in those who perceive their illness to have a cyclical or unpredictable timeline and those who perceive a higher emotional burden from their disease. Perceptions of consequences and identity (symptom burden) dimensions have also shown negative correlations and perceived illness coherence has shown positive correlations with QOL. A recent meta-analysis 2 has similarly reported that the perceptions of consequences an illness may have and emotional representations dimensions have the strongest relationships with psychological outcomes, including QOL, across a wide range of illnesses such as cancer, epilepsy, heart failure, rheumatoid arthritis, and pulmonary diseases. In SCD, the illness can be devastating with multiple hospitalizations and possibility of life-threatening complications. Patients can be emotionally affected by seeing negative outcomes among their peers. The illness can be quite unpredictable, and it is yet difficult to predict an individual’s life course with the illness. The most common clinical presentation is “painful crises,” which tends to be unpredictable and is a source of stress for the patients as well as families. 55
The CSM has been applied to youth with diabetes mellitus and SCD, and in qualitative assessments, SCD youth have similarly described the uncontrollability and chronic nature of the illness, yet many express hope for a cure. 12 They report many emotional disturbances such as being distressed by others’ perceptions of their illness, feeling embarrassed, and socially excluded. Ramondt et al 56 have used drawing to determine patients’ perceptions and report that patients feel their illness is chronic and severe, and those drawing more abnormal cells have poorly perceived personal control and greater emotional distress, which is associated with poor control of their illness. Use of drawings may be an important tool to assess patient perceptions and needs further work in this particular population.
In the present study, higher educational levels, and not older age per se, were found to be positively associated with better QOL, and this relationship may be mediated through more positive illness perceptions. Higher educational achievement has been shown in various studies to have more positive outcomes, such as lower disease prevalence, higher prevalence of risk factors for chronic disease, longer life expectancy, greater self-care, and general health status.57-59 Past studies in our adolescents have reported that being in school seems to be a resiliency factor and appears to be protective against risky behaviors and depressive symptoms.25,29 As adolescents become adults, higher educational attainment will also afford them better employment opportunities and hence improve their self-management capabilities. 57
Disease knowledge has shown no effect on QOL in our final regression model or on correlational analysis; however, it is positively correlated with many illness perceptions, especially positive perceptions such as how coherent they are of their illness, and their perceptions of controllability of their illness. It also correlates significantly with the perception of chronicity of their illness and the many consequences their illness have. Even though these are negative perceptions, it is important to note that they are accurate perceptions with respect to this particular disease and maybe useful in preparing the individual to face his/her illness challenges. Furthermore, our study also supports more recent understanding that disease knowledge alone is not sufficient for outcomes in chronic illness but there is a role to improving disease knowledge 60 as it may positively influence patient perceptions.
Severity of disease showed the strongest association with QOL, contributing 18.6% of the total variance, but illness perceptions were also closely associated to QOL, contributing an additional 12.1% of the variance in the model. Disease severity itself was significantly correlated to perceptions of symptom burden, cyclical timeline, and higher consequences. This is not congruent with all studies as others have reported that severity does not affect adjustment issues such as IQ, self-esteem, social and personal adjustment, behavioral problems, 44 or psychological adaptation. 30 Our studies in adults with SCD have shown significant associations of higher burden of disease, especially frequent pain crises and leg ulcers with depression and loneliness 61 but not with QOL.62,63 Interestingly there was no difference in illness perceptions between persons of different genotypes (data not shown), as anecdotally in Jamaica, persons with the heterozygous SC genotype often think themselves to carry “sickle cell trait” and so might perceive their illness to be less serious.
The CSM originally operationalized the role of coping strategies as a mediator between illness perceptions and QOL and other psychological distress outcomes, but more recent works have been conflicting as to the precise role of coping. The current work has not explored coping as a determinant of QOL, but the role of illness perceptions in affecting QOL in our sample of adolescents with SCD is clear. Even though this study was conducted only in a clinic-based sample, the SCU does provide service to affected persons all around the island 64 and so our sample is at least moderately representative. This work continues to develop our understanding of especially psychosocial issues in young persons with SCD who are at a conflicting period of development and becoming independent, yet a period where they still require a large amount of support from families, communities, and health care systems to successfully negotiate this phase. Further studies will need to develop interventions that are targeted more specifically toward improving issues that are being identified.
In conclusion, illness perceptions and severity of disease have shown strong associations with QOL of adolescents with SCD. Even though disease knowledge shows no association, it is strongly correlated with many positive illness perceptions that these adolescents develop and may likely mediate their effect on quality of life.
Footnotes
Authors’ Note
The Principal’s office (the funding agency) had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Trial Registration
Author Contributions
MRA: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ABG: Contributed to design; contributed to acquisition and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MG: Contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JKM: Contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Principal’s New Initiative Grant, The University of the West Indies, Kingston, Jamaica.