
Abstract
There is an epidemic of pediatric obesity in the United States. In most cases, there is an excess in the amount of calories consumed, compared with the amount of calories expended. Numerous body systems are affected by pediatric obesity, with complications varying between boys and girls. Behavioral, genetic, and environmental factors affect the ability of children to avoid becoming obese. Primary care physicians should screen for obesity in children as much as possible. Associated risk factors for obesity should be uncovered. Methods of preventing obesity should be discussed routinely with children and their families. Healthy dietary habits are key, and so are family-oriented interventions, such as eating together at dinnertime. One hour of moderate to vigorous activity daily is recommended for children and adolescents. While pediatric bariatric surgery is an option, there are also numerous nonpharmacological and pharmacological measures available as management for pediatric obesity. Family-based approaches, such as reducing screen time, have been very successful. Non–weight-bearing exercises also help children and adolescents expend calories without causing injury to themselves. Family availability, activity preference, and developmental levels should all be considerations when managing pediatric obesity. Motivational interviewing may also be helpful, especially when customized for each specific patient and family. Clinicians will play an increasing role in terms of identifying, treating, and preventing pediatric obesity; measures that can be done in the clinic should be considered more and more.
Keywords
Introduction
The rate of pediatric obesity has been on the rise for many years. As a result of pediatric obesity trends that have prevailed for years, there has been an increase in complications associated with pediatric obesity, prompting numerous studies on interventions to treat and prevent obesity in children. Most of these studies are of small sample size and short follow-up, emphasizing the need for large randomized controlled trials with extended follow-up. Despite their limitations, these studies do provide useful recommendations on interventions for obesity in children. 1
Background
Obesity is a state of having excess body fat because of more calories consumed than calories utilized.2,3 The national consensus for the definition of overweight is a body mass index (BMI) ≥85th percentile and below the 95th percentile for sex and age. Obesity is defined as a BMI ≥95th percentile for sex and age, and severe obesity is defined as a BMI ≥99th percentile.4-7 Internationally, there is no consensus on the categorization of overweight and obese. Other definitions in use include 110% and 120% of ideal weight and height, respectively; weight-for-height z scores of >1 and >2; and 85th, 90th, 95th, and 97th percentile for BMI. 1
Pediatric obesity can affect numerous systems (Figure 1).1,8,9 Some children are affected by hypertension and diabetes. Although cardiovascular events are rare in children, most obese children remain obese throughout adulthood and may then experience myocardial infarctions and strokes; the atherosclerotic process appears to accelerate in obese children.1,10 Other children are more frequently affected by obstructive sleep apnea and reactive airway disease.1,11 Although obese children may have asthma, it is often misdiagnosed, as there may be weight-related respiratory restrictions.1,12 Musculoskeletal complaints, including fractures, discomfort, difficulty with ambulation, and lower extremity misalignment, may be more common in obese children.1,13 More serious musculoskeletal complications include adolescent bowing of the legs1,14 and slipped capital femoral epiphysis.1,15
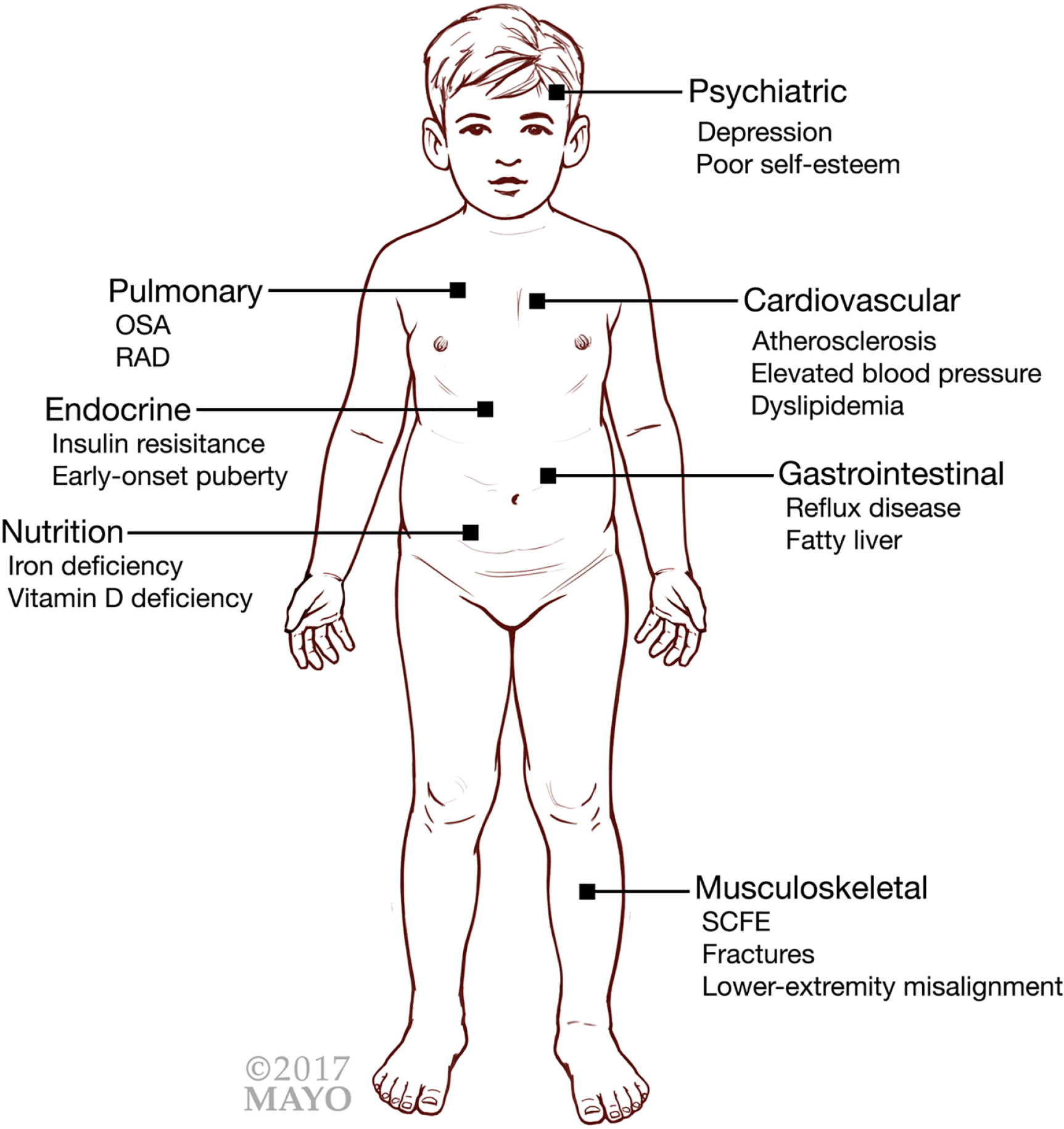
Complications associated with childhood obesity.
Other complications seen in obese children include a more rapid onset of menarche in girls1,16,17 and pubertal maturation in boys.1,18 Nutritional deficiencies, such as lower levels of vitamin D1,19 and iron deficiency,19-21 tend to also be present in obese children. On a more positive note, the greater fat mass in obese children appears to lead to increased bone mineral content.1,22 Unfortunately, the complications associated with pediatric obesity outweigh any benefits.
Obesity is affected by many environmental, genetic, and behavioral factors. Of these factors, behavior, such as activity level, is the most susceptible to change.2,23 A clinical approach is crucial for primary care providers in getting this generation’s children to move and engage in more physical activity.
Epidemiology
Although the statistics for pediatric obesity differ depending on sex, age, and racial group, obesity within the United States continues to be a significant problem. The rate of childhood obesity has more than doubled in children and tripled in adolescents in the past 30 years. From 1980 to 2010, obesity increased from 7% to 18% in children ages 6 to 11 years and from 5% to 18% in adolescents ages 12 to 19 years.24,25 In 2010, more than 30% of children and adolescents were overweight or obese.1,24,25
Screening for Obesity in the Clinic
Screening for obesity should be a standard of care for primary care physicians. It is endorsed by both the US Preventive Services Task Force (USPSTF) and the American Academy of Pediatrics (AAP). However, whereas the USPSTF recommends screening in children ages 6 years and older, the AAP recommends screening to begin at age 2 years. Both entities agree that screening should be done by measuring BMI. 26 The recommendation statement of the USPSTF reports that there is no clear evidence to guide for the correct screening interval for obesity, but height and weight, which are used to calculate BMI, should be measured during health maintenance visits.
Obesity screening should include an evaluation of associated risk factors. The history and physical exam should direct the evaluation. A history of early-onset obesity, developmental delays, or dysmorphic features on exam may suggest genetic defects or syndromes such as a defect in the leptin signaling pathway, Prader-Willi syndrome, fragile X syndrome, or WAGR syndrome (a syndrome in which affected children are inclined to develop Wilms tumor, aniridia, genitourinary anomalies, and mental retardation).1,27,28 Children who continue to have increasing weight and no significant increase in height should be evaluated for endocrine-related dysfunctions, including hypothyroidism, Cushing syndrome, and growth hormone deficiencies. Medications should be reviewed for any that may lead to weight gain, including insulin, insulin secretagogues, glucocorticoids, hormonal contraceptives, and antihistamines. Antihypertensives such as clonidine and propranolol and anticonvulsants including gabapentin, carbamazepine, and valproic acid have also been associated with weight gain. In addition, tricyclic antidepressants including amitriptyline, imipramine, and nortriptyline and selective serotonin reuptake inhibitors like paroxetine and mirtazapine may also lead to weight gain. Providers should beware of antipsychotics such as clozapine, olanzapine, and risperidone and mood stabilizers such as lithium because unintended weight gain is a common adverse effect for them as well.1,27,28 Alternative means of treatment should be considered for obese children on medications that may cause weight gain. However, although it is important to investigate for other disorders associated with obesity, most patients will not have any identifiable disorders.
Obesity screening should also include obesity-specific education about the definition of obesity, its causes, risk factors, complications, treatments, and perhaps, most important, methods of prevention.
Recommendations on Advice and Interventions
Prevention is a powerful means of addressing the current public health problem of obesity. Patients should be counselled on healthy preventative habits. There is evidence to suggest that obesity prevention should occur during preconception, because maternal BMI before pregnancy and gestational weight gain are associated with adiposity in offspring and childhood obesity. As such, pregnant women should follow recommended weight gain throughout pregnancy to prevent possible obesity in their children.29,30 In the postpartum period, breastfeeding is believed to have some protective effects on the development of childhood obesity and should be encouraged.31,32 Dietary habits that help prevent childhood obesity include limiting eating at restaurants, reducing portion sizes, and limiting the consumption of sugar-sweetened drinks, including juice. Eating together as a family at a dinner table without distractions and a diet with ample servings of fruits and vegetables are other healthy dietary habits that should be encouraged.33-35
Active lifestyles also prevent childhood obesity; thus, moderate to vigorous activity should be encouraged for at least 1 hour daily. Furthermore, families should establish regular activities such as walks or other outdoor exercise. Finally, the amount of screen time, especially watching television, should be no more than 2 hours daily starting at the age of 2 years. Children under 2 years of age should have no screen time.35-37 These are counselling points that pediatric patients, especially those who are overweight or obese, should discuss during doctor’s office visits.
There are numerous pharmacological and nonpharmacological interventions proposed for the treatment of pediatric obesity with an increasing role for pediatric bariatric surgery for medically complicated obesity in children. The basis of all treatments remains a goal of energy expenditure that surpasses energy consumption. Physical activity is an effective means of energy expenditure. An assessment of physical activity or lack thereof is important in getting children to move. A primary care provider should evaluate the amount of screen time (which includes time spent watching television, playing video games, texting, time spent on the computer, tablet, or other electronic device), quality of physical activity, both structured and unstructured, 3 and social and environmental factors that may pose barriers to activity. This would include the availability space and facilities near the home that could be utilized for physical activity as well as the parent’s perceived level of safety within this space. This assessment will help set intervention goals and provide a baseline from which further interventions and behavior modifications would begin.
Family-Based Approach
The family-based approach is a method for treating obese children that has been successfully applied since the 1970s. Obesity tends to run in families, and research shows efficacy in targeting activity change in both the parents and the children. 38 In the family-based approach, a parent’s BMI is considered an independent predictor of an obese child’s BMI. Weight change in a child has been positively related to parent weight changes when both parents and children were targeted. 38 However, in studies where children were treated alone, results showed that children and parent weight change were negatively related. 39 The family-based approach motivates parents to make behavior changes in their activity habits similar to the changes their children make. As a result, the parents themselves lose weight and can be role models for the behavior of their children. 39 Children may benefit tremendously from weight loss through physical activity when the family-based approach is applied.
Reduced Screen Time
Efforts to help overweight or obese pediatric patients lose weight should be aimed indirectly at reducing sedentary behaviors and directly at incorporating or increasing physical activity. For the most part, in developed countries such as the United States, sedentary activity is in the form of screen time. As previously mentioned, current recommendations limit daily screen time to 2 hours a day for children ages of 2 to 19 years and discourage it altogether for children under 2 years of age.40-42 For children who are watching television in excess of the recommend hours, a gradual decrease in time is recommended to avoid discouragement. Some ways to decrease excess screen time include not putting a television in children’s rooms and not allowing viewing during meals. Decreasing screen time is important because not only does it free up time that could potentially be used for physical activities, but it also helps reduce caloric intake.40-42
Daily Physical Activity
It is recommended that children have at least 60 minutes of physical activity a day. The AAP recommends at least 30 minutes of structured activity during the school day. 43 However, children who are not physically active to begin with can start with as little as 2 minutes a day and increase this daily, weekly, or on other agreed-upon increments. 43
There is a great deal of physical difficulty that some obese children may encounter when engaging in new physical activities. Some of that difficulty is related to the complications of pediatric obesity (eg, respiratory difficulty, musculoskeletal complaints/complications). As such, it may be good to advice children to start with non–weight-bearing activities such as swimming or biking.
When discussing activities, a child’s developmental level, activity preference, and family availability should be considered. Younger children may be more engaged in nonstructured activities that would involve other peers and family members, such as playground play, active video games, or other leisurely activities. Older children may prefer structured activities, such as team-based organized sports or even individual sports. Other creative physical activities that do not necessitate fees or memberships include dancing, jumping rope, using aerobic videos, biking, or hiking. Oftentimes, for lifestyle modifications including diet, a holiday is allowed, usually on the weekends or special celebrations during which the child is allowed bigger servings or calorie-dense foods. However, there should be no holiday from exercising because children should engage in physical activities every day. An important aspect of this intervention is the need for a reward system agreed upon by the child and parent. Reward systems reinforce positive behaviors such as exercise. 42 Food should not be used as a reward. Once a reward is earned, it should not be taken away as punishment.
Motivational Interviewing
The growing trend of patient-centered care suggests that motivational interviewing is a viable alternative to the standard intervention approach. 44 Motivational interviewing is a technique in which the clinician becomes a helper in the change process and expresses acceptance of the patient. The therapeutic relationship is a democratic partnership, meaning that the goal is to elicit self-motivational statements and behavioral change from the patient himself/herself and to enhance motivation for positive change.45,46 Basically, motivational interviewing activates the capability for beneficial change that all patients have. 46 The clinician, when bringing up interventions to address preventing or turning back obesity, should
Express empathy with the child/adolescent through reflective listening
Develop discrepancies between the patient’s goals or values and his/her current behavior
Avoid arguments and direct confrontation
Adjust to patients’ resistance rather than opposing it directly
Support self-efficacy and optimism
Motivational interviewing is customized for the specific patient or family situation and is directed by their input. It promotes patient autonomy and assesses readiness and motivation to change. It also acknowledges barriers and ambivalence and supports a self-directed approach in a nonjudgmental way. This intervention is different from the standard method where targets are prescribed. The standard method, in which consistent evidence-based goals are reinforced, assumes that parents and children are capable of using prescribed skills to meet prescribed goals, and it expects parents and children to follow the standard program. A motivational interview approach may work better with family-based interventions to increase physical activity in children because it helps set specific and realistic self-directed goals (eg, “We will take a family walk 3 times a week before dinner” vs “We will exercise more”). To prevent discouragement, goals may initially be easy and can be modified over time. The standard approach remains effective; still, a motivational approach for the management of childhood obesity through increased physical activity is presumably more acceptable to patients because it promotes autonomy. 44 It should be stressed that the motivational approach is just one of the possible approaches that can be taken; there appears to be no distinct advantage to a motivational approach over a standard prescriptive approach. 44
Conclusion
The rate of pediatric obesity has been on the rise for many years and has just recently shown signs of slightly decreasing. As a result of the multiple associated comorbidities, research on interventions and treatments is ongoing. Many environmental, genetic, and behavioral factors affect pediatric obesity; however, the majority of cases are because of ingesting more calories than one expends and not because of genetics, adverse reactions, or metabolism. Primary care providers should encourage practical and feasible lifestyle interventions to get this generation’s children to move and engage in more physical activity with focus on reducing screen time and interventions involving the entire family.
Author Contributions
GGAP: Contributed to conception; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
IA: Contributed to conception; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MJT: Contributed to conception; contributed to acquisition; drafted manuscript; critically revised manuscript; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ROW: Contributed to conception; contributed to acquisition; drafted manuscript; critically revised manuscript; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ARG: Contributed to conception; contributed to acquisition; drafted manuscript; critically revised manuscript.
Footnotes
Acknowledgements
Ms Alison Dowdell for all her assistance, including, but not limited to, formatting, proofreading, and submitting this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.