
Abstract
Objectives:
Exercise physiology is a branch of physiology that studies how physical activity and exercise alter the structure and function of living organisms. Knowledge of exercise physiology is crucial to improve athletic performance, improve people’s ability to cope with extreme circumstances and approach chronic diseases. This research aimed to evaluate the knowledge of future healthcare professionals, namely, the medical students in Jordan regarding exercise physiology.
Methods:
Responses were collected from 524 undergraduate medical students enrolled in clinical clerkship. An online survey that evaluated participants’ basic understanding of various physiological concepts related to physical exercises, such as respiratory exchange ratio, physical fitness, V̇O2 max and exercise at high altitudes was employed in the study.
Results:
63.2% of participants had a poor level of exercise physiology knowledge. Misconceptions regarding V̇O2 max definition (93.3%), application (46.4%), significance (35.6%) and related physiological factors (48.7%) were observed. Students had misconceptions about physical fitness evaluation questions (52.5%, 39%, and 41.8%, respectively). Student proportions of 37%, 41%, 80.3% and 73.1% showed misconceptions about muscle groups and energy systems during training, training prescription variables, respiratory exchange ratio, and high-altitude performance, respectively. Significant differences in knowledge levels were found based on respondent characteristics (p < 0.05).
Conclusions:
Knowledge of exercise physiology is more than desirable for medical professionals. Therefore, efforts must be made to increase awareness and improve knowledge about basic physiological fundamentals related to exercise physiology among medical students in Jordan, as they represent the backbone of healthcare professionals of the future who will deal with medical conditions related to physical activity and exercise.
Introduction
Physiology is the science that deals with the function of living organisms by understanding the function of their components, including biomolecules, cells, tissues and organ systems. It also deals with the effect of external environmental stimuli on the function of living organisms. Exercise physiology is a branch of physiology that studies how acute or training exercise and physical activity alter the structure and function of living organisms. 1 Understanding the science of exercise has developed from simple mechanistic studies based on observation in the field to complex mechanistic studies incorporating physiology, biochemistry and molecular biology. 2 Physical activity is any skeletal muscle-driven action of the body that requires a net energy (Adenosine triphosphate, ATP) expenditure. Exercise is a sort of physical activity that is repetitive, planned and structured to develop or preserve one or more of physical fitness-related aspects. 3 Physiological alterations taking place during physical activity include adjustments of the metabolism and function of many body organs, such as the heart, lungs and muscles, as well as structural alterations to the cells themselves. 4 Exercise physiology also evaluates the impact of extreme environmental factors on living creatures’ capacity to react and acclimatise to physical activity. 1 Therefore, exercise science has substantially helped in the understanding of human physiology and body coping mechanisms for different types of training. The development of exercise science has led to the emergence of many specialists in this field, including exercise physiologists. 5
Regular physical exercise is an important practice to improve physical fitness, physiological function and overall human health. Chronic physical exercise is associated with a lower prevalence of many chronic diseases such as heart disease, high blood pressure, cancer and diabetes. 6 Moreover, it is well established that physical exercise is vital for preventing systemic inflammation and reducing communicable diseases. The immune system function is significantly impacted by physical activity. Exercise with moderate intensity enhances cellular immunity while vigorous exercise may negatively affect the immune system function and increase the possibility of contracting infectious diseases. 7 To elucidate the fundamental mechanisms that are involved in exercise-related health benefits, several previous studies have been conducted. These studies revealed that physical exercise is associated with the activation of interconnecting molecular and cellular pathways, generating an adequate response to overcome exercise-related changes in body homeostasis. This physiological adaptation to physical exercise is associated with persistent modifications in body organ systems, resulting in health promotion. 8
Medical doctors have the power to significantly impact their patients’ lifestyle choices through advising and encouraging their patients to commit to healthier practices. They are able to inspire their patients to avoid practising unhealthy habits, and patients often value and respect their medical doctors’ advice. 9 Additionally, having a thorough understanding of exercise physiology will enhance the way doctors counsel their patients, which will benefit their patients. Nevertheless, many doctors face a number of challenges that prevent them from providing physical activity counselling and therapy. Unfortunately, the lack of awareness about exercise and physical activity is one of these major challenges. 10
Knowledge of exercise physiology has been used to comprehend how exercise can help with the management of numerous chronic diseases, either as a form of treatment or as a preventative measure.1,5,11 Additionally, it has been employed to improve athletic performance, 12 and enhance the ability of people to cope with extreme environmental circumstances such as high altitude. 13 Therefore, the appearance of sports physiology and sports medicine reflects the growing interest in connecting exercise physiology to several practical issues. Misconceptions about sports and exercise science can jeopardise the care given by healthcare professionals, especially in light of the fact that the advantages of regular physical activity are maximised when they are properly prescribed, supervised and guided in both clinical populations and athletes. Inappropriate physical activity can potentially endanger people’s safety and health. 14
Exercise physiology knowledge is crucial not only for clinical advice and exercise prescription but also because it can have a significant impact on medical students’ understanding of normal physiological phenomena and common pathologies. A comprehensive understanding of exercise physiology enables medical students to understand physiological functions of the cardiovascular, respiratory and metabolic systems, thus leading to a deeper understanding of the physiological functions of the body. The further value of this knowledge lies in the fact that it enables medical students to understand common pathological conditions. For example, exercise physiology sheds light on how physical activity modulates cardiovascular health and how it plays a part in diseases like hypertension and coronary artery disease. Therefore, a thorough understanding of exercise physiology not only helps aspiring physicians assist patients in leading better lifestyles, but also improves their ability to diagnose and treat a wide range of medical issues.
The fact that earlier research has shown that American nursing and biology undergraduates 15 as well as British sports science undergraduates 16 have misconceptions about human physiology makes it reasonable to assume that Doctor of Medicine (MD) students also have these misconceptions about topics related to exercise and sport, such as metabolism, biochemistry and physiology. Moreover, although the number of studies highlighting the importance of physical exercise in promoting human health has increased substantially, 17 and the critical role that medical doctors play in influencing their patients to practice physical activity to manage and/or prevent different types of chronic medical diseases, the number of studies evaluating the level of awareness and understanding of medical doctor students (and subsequently future health professionals) about exercise physiology is very limited. Therefore, this study was designed to evaluate the knowledge of future healthcare professionals in Jordan regarding exercise physiology. To the best of our knowledge, no similar previous research was conducted on these topics in the Jordanian contexts, and this is the first study investigating the misconceptions regarding exercise physiology knowledge among undergraduate MD students; hence, the purpose of our study is to determine whether future healthcare professionals have any misconceptions regarding some aspects of exercise physiology.
Methods
Participants
This descriptive cross-sectional study was conducted in Jordan between September 2022 and January 2023. Participants who were eligible to participate in the study were: (1) Undergraduate medical students during their clinical clerkship training (i.e. 4th, 5th and 6th year medical students) in medical schools in Jordan. (2) Aged 18 years or older. Participants, who were younger than 18 years and were non-undergraduate medical students during their clinical clerkship training, were not eligible to take part in the study. The estimated sample size to be included in this study was calculated using the online sample size calculator Raosoft 18 with an accepted margin of error of 5%, a confidence interval of 95%, and a response distribution of 50%. The estimated number of undergraduate medical students during clinical clerkships in Jordan is approximately 7485 students. 19 The minimal sample size calculated was 366 participants, and the current study employed more than 500 students.
Study design and preparation of questionnaire
The survey was in English and had multiple sections. Section A provided a brief overview of the study topic and aims, and stated that engagement in the study is entirely anonymous and voluntary. It also included a consent form to take part in the study and publish the study findings. Section B gathered socio-demographic information about the participants, including age, sex, marital status and place of residence, along with academic information and questions regarding the participant’s beliefs towards physical exercise. Additionally, this section investigated some variables that could predict or impact the participant’s academic achievement and knowledge of exercise physiology, such as cumulative grade point average (GPA) in all basic medical years, preparation approach for medical exams during basic medical sciences years, student failure in any medical courses during basic medical years (years 1–3). Section C of the questionnaire was adapted from a study by Leal et al. 20 and included 11 multiple-choice quiz questions that had been previously developed to evaluate participants’ basic understanding of exercise physiology. 20 Each quiz question is a multiple-choice question with one correct answer and a choice of ‘I do not know’ to discourage guessing and random answer selection. The quiz questions aimed to assess the participants’ knowledge of various physiological concepts related to physical exercises, such as the respiratory exchange ratio (RER), physical fitness and maximal oxygen consumption (V̇O2 max), as well as their practical uses.
Validity and reliability of the questionnaire
The questionnaire was pilot-tested on 30 students (5.7% of the population). The responses from the pilot study were not included in the final analysis. The questionnaire’s Cronbach alpha reliability coefficient value was 0.89.
Data collection procedure
To collect the data, a web-based survey was utilised. Google Forms were used to build the online questionnaire. The questionnaire was distributed to the students through teaching platforms directed at medical students during their clinical clerkship, along with social media platforms such as Facebook, WhatsApp and Telegram. No incentives were offered to the participants to encourage them to respond.
Statistical analysis
To assess the students’ level of physiology knowledge, a scoring system was employed, where a score of 0 was given for an incorrect or ‘I don’t know’ response and a score of 1 was awarded for a correct response. 21 Each student’s total knowledge score was then converted to a percentage, ranging from 0 to 100%. The knowledge percentages were then categorised into three groups: Poor knowledge category (⩽60%), moderate knowledge category (60.01–80%) and good knowledge category (⩾80.01%). 21
Descriptive statistics such as mean, frequency (N) and percentages (%) were employed to summarise the data. Chi-square (χ2) test was used to identify the existence of statistically significant dependence between the respondents’ knowledge level and each of their sociodemographics, beliefs towards physical exercise and predictors of academic achievement. A statistically significant difference was considered when p ⩽ 0.05. Version 26 of the Statistical Package of Social Sciences software (SPSS, IBM Corporation, Armonk, NY, USA) was used for statistical analysis.
Ethics approval
This study was approved by the Hashemite University Institutional Review Board (IRB) Committee (No. 26/2/2022/2023). Additionally, written informed consent was obtained from all subjects before the study.
Results
The study participants’ socio-demographic features are shown in Table 1. A total of 524 MD students who enrolled in their undergraduate clinical clerkship participated in the current study. The average participant age was 22.16 years. Among these students, more than 50% were female, and more than 95% were unmarried students. The vast majority of recipients (88.7%) resided in urban areas. There were 166 (31.7%) students from the fourth medical year, 240 (45.8%) students from the fifth medical year, and 118 (22.5%) students from the sixth medical year. The distribution of students participating in clinical rotations at the time of the survey was as follows: Internal medicine made up 114 (21.8%) of the students completing their clinical rotations, followed by surgery with 96 (18.3%) students, paediatrics with 68 (13.0%) students, obstetrics and gynaecology with 55 (10.5%) students, emergency room (ER) with 9 (1.7%) students, and other clinical rotations with 182 (34.7%) students.
Sociodemographics, beliefs towards physical exercise and predictors of academic achievement of the study participants.
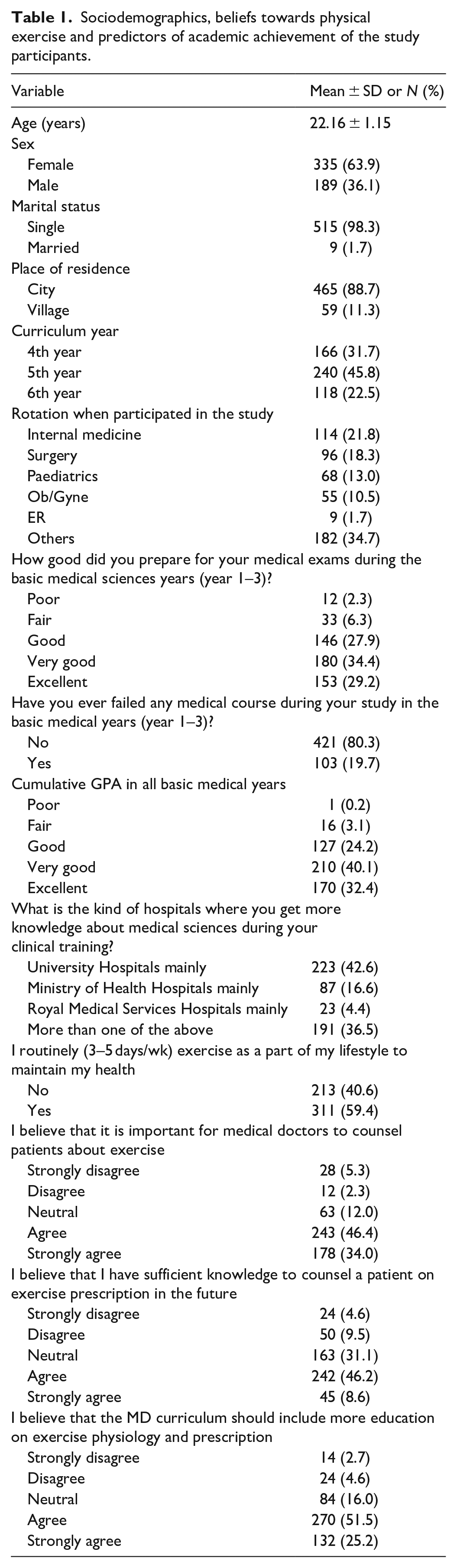
The MD students were asked to reflect on their personal study routines over the first 3 years of their education in order to prepare for their MD tests as well as their academic performance. Only a small minority (8.6%) of MD students who took part in the study reported fair to poor preparation, while the majority of MD students (63.6%) indicated that they prepared for their MD exams in a very good to excellent manner. Moreover, a large percentage of participants (80.3%) never failed any medical courses during their first 3 years of MD study. Furthermore, over 95% of students achieved a cumulative GPA of good to excellent in all basic medical courses. Regarding the participants’ beliefs towards physical exercise knowledge, the majority of students acknowledged the significance of doctors advising patients about exercise and felt that the MD curriculum should provide more education on exercise physiology.
The exercise physiology knowledge questionnaire included an 11-question quiz designed to assess familiarity with fundamental concepts related to exercise physiology. For each question, five alternatives (a–e) were presented as possible answers. The responses of the medical students to this 11-question quiz are summarised in Table 2. The students’ responses to the various items on the exercise physiology knowledge questionnaire exhibited considerable variation. For instance, 93.3% of the students were unable to define V̇O2 max correctly in question 1. In question 2, 46.4% of the students held misconceptions about the use of V̇O2 max in physical evaluation and exercise prescription. Similarly, in question 3, 48.7% of the students were not familiar with the physiological factors that control V̇O2 max, while 35.6% did not understand the significance of V̇O2 max in physical assessment and exercise prescription in question 4. Out of the 524 participants, 52.5%, 39.3% and 41.8% of the students reported misconceptions about physical fitness evaluation questions 5, 6 and 7, respectively. For question 8, 37% of the students did not know that both muscle groups and energy systems are used during physical training. In question 9, which assessed the knowledge of variables related to training prescription, 41% of the students answered incorrectly, and only 19.7% provided the correct response for question 10 that assessed the students’ knowledge regarding RER. Lastly, 73.1% reported misunderstandings related to physical performance in environments of high altitude in question 11.
Summary of exercise physiology knowledge questionnaire responses.

Indicates correct answer.
Overall, the mean value of students’ knowledge percentages was less than 50%. Among the participants, the majority (63.2%) had a poor level of knowledge, while 22.5% had a moderate knowledge level, and only 14.3% had a good knowledge level (Table 3). In order to investigate if there was a connection between the exercise physiology knowledge category of the participants and their socio-demographic characteristics, academic information, beliefs towards physical exercise, and predictors of academic achievement, a chi-square (χ2) test was employed. The chi-square (χ2) test outcomes are displayed in Table 4. According to the results, there was statistically significant association between knowledge levels and certain respondent characteristics such as marital condition (p = 0.013), residence location (p < 0.001), curriculum year (p = 0.007), preparation approach for medical exams during basic medical sciences years (p = 0.007), and the hospital kind where the students obtained more learning about medical sciences during their clinical training (p = 0.012). The good knowledge category had a higher proportion of married respondents and respondents who resided in villages compared to single respondents and respondents who resided in cities. Compared to respondents who are in their 4th-year studies, a higher proportion of students in their 5th and 6th year of MD studies were found to be in a good knowledge category. Students who had excellent preparation for medical exams during their basic medical sciences years were more likely to be in a good level of knowledge compared to those who had lower levels of exam preparation. Finally, a good level of knowledge was associated with a higher proportion of students who acquired greater knowledge in medical sciences during their clinical training in university hospitals mainly, compared to those who trained in other types of hospitals.
Profile of MD students exercise physiology knowledge categories.

Chi-square (χ2) test of association between socio-demographic characteristics, academic information, beliefs towards physical exercise and predictors of academic achievement with respect to exercise physiology knowledge category.

Discussion
The knowledge of exercise physiology is essential for medical professionals, athletes and enthusiasts of fitness and health. It allows them to create and provide suitable exercise prescriptions for better physical performance, fitness and health outcomes. The current study evaluated the awareness of future healthcare professionals in Jordan regarding exercise physiology. The present study demonstrated that the exercise physiology knowledge of Jordanian undergraduate MD students during their clinical clerkship was insufficient, suggesting the existence of misconceptions and inadequate awareness of key principles in exercise physiology.
Several previous studies were carried out on the knowledge of physical activity recommendations and exercise prescription which have shown deficient knowledge of healthcare providers regarding physical activity knowledge and counselling.9,22 O’Brien et al. 9 reported that doctors’ knowledge, attitudes and application of physical activity counselling are noticeably lacking in Ireland. The survey results also point to a large disparity in the availability of training in physical activity counselling at the graduate and undergraduate levels. 9 Another recent study evaluated the knowledge level regarding physical activity among final-year medical students in the UK and demonstrated that more than 50% of the students involved in the study had a deficient knowledge of physical activity concepts. 22 However, a very limited number of studies have been conducted in the context of physicians’ and medical students’ knowledge regarding exercise physiology. Courses in Jordanian medical school cover topics related to exercise physiology in years 1–3 of the MD programme, including basic physiology, cardiovascular physiology, respiratory physiology, muscle physiology, metabolic pathways and energy systems, endocrine responses, environmental physiology and the application of exercise physiology principles in preventing and managing medical conditions like cardiovascular diseases, diabetes and obesity.
V̇O2 max is an indicator of individual’s capacity to transport and utilise oxygen during physical activity. It is used for the estimation of cardiorespiratory fitness 23 where elevated levels of V̇O2 max are linked with increased life expectancy and better health and vice versa. 24 The findings of the current study suggest that the majority (93.3%) of MD undergraduates incorrectly defined V̇O2 max. A previous study conducted by Leal et al. 20 showed that more than 60% of the respondents incorrectly defined V̇O2 max. Additionally, the study reported that 46.4% and 35.6% of the students held misconceptions regarding the application and importance of V̇O2 max in physical evaluation and exercise prescription, respectively. These findings are in line with the results of the study of Leal et al. 20 which revealed that 50–60% and 20–30% of the participants showed insufficient knowledge regarding the application and importance of V̇O2 max in physical evaluation and exercise prescription, respectively. Moreover, approximately 30% of the participants involved in Leal et al study 20 had inadequate knowledge about the factors that affect V̇O2 max, which is similar to the finding of the present study. To the best of our knowledge, this is the first study reporting that clinical medical students showed insufficient knowledge regarding V̇O2 max, which is a critical parameter employed in aerobic fitness estimation, exercise performance assessment and general health evaluation. Misconceptions about V̇O2 max definition and its application may culminate in several negative consequences. For example, missing the fact that V̇O2 max is an important parameter used in the assessment of aerobic fitness level and measuring of training effectiveness25,26 might result in the application of other fitness evaluation measures, which may not precisely evaluate the aerobic fitness level of individuals when compared to V̇O2 max. Unawareness of V̇O2 max testing procedure or of factors that may control V̇O2 max such as age, genetics, gender, cardiorespiratory function and body fat 27 may contribute to unreasonable expectations or misinterpretation of the test results. Finally, ignorance of V̇O2 max importance and application in health measures may lead to inadequate design of training programmes and exercise prescription that may result in adverse health consequences such as increased physical injuries and reduced physical performance. 14 To sum up, misconceptions regarding V̇O2 max can have several outcomes which can impact the assessment of aerobic fitness level, V̇O2 max test results analysis, and exercise prescription.
The present research is designed to assess the knowledge of MD students regarding physical fitness evaluation as well. Physical fitness evaluation includes a group of tests that measure the body components of physical fitness, including body composition, cardiorespiratory endurance, musculoskeletal flexibility and muscular fitness. 28 The available information in the research literature for comparison, aside from the study by Leal et al., 20 is insufficient. In contrast to previous research conducted by Leal et al., 20 the observed prevalence of misconception regarding physical fitness evaluation among clinical MD students in this study exceeded those observed in the Leal et al. study. The observed difference between the present study findings and Leal et al.’s study findings can be potentially attributed to several factors, one of which may be the differences in medical school curricula between Jordan and Brazil. Medical education is known to vary globally, with different institutions emphasising distinct aspects of the curriculum. These differences include the amount of exercise physiology content in the curricula, the timing of the introduction of such topics, and other unique features of medical education related to each country. Evaluation of individual’s fitness is essential for identifying health risks and designing an effective physical exercise that meets individual’s fitness needs and aims. 28 Nevertheless, misunderstandings about physical fitness assessment could result in improper exercise recommendations and possibly harmful outcomes. Additionally, a lack of knowledge about the essential elements needed for reliable laboratory tests and misconceptions about the goals and execution of these investigations could make laboratory testing less accurate and reliable, which would result in improper exercise recommendations and inadequate outcomes.
The results of the current research demonstrated that a substantial number of MD students were ignorant of the facts about the importance of targeting both muscle groups and energy systems in establishing training programmes. Several previous studies29–31 illustrated the indispensability of including both body musculature and energy systems in developing potent fitness training required for outstanding performance and minimum risk of injury. In regard to the knowledge of workload aspects of a physical training program which include intensity, duration and frequency of training, 32 it was observed that 41% of the medical students taking part in the current study possessed wrong knowledge regarding the components of training load which may result in the planning of training programmes that are unsatisfactory or unsuccessful to gain optimal results. 33 The vast majority of medical students in this showed poor knowledge regarding the RER. RER is used to identify the comparative contribution of each of carbohydrates and fats to total energy consumption during exercise. This physiological parameter increases with the increased level of exercise intensity. Further, high RER suggests that carbohydrates are the main source of body energy while a low RER reflects that fats are the principal source of body fuel. 34 Understanding the way that the body utilises energy during physical activity can help physicians to improve individuals’ training and adjust their dietary needs. For instance, training individuals for endurance sports, such as marathons demands concentrating exercise of moderate intensity that will encourage their bodies to utilise lipids as the primary source of energy. If there was a good quality of knowledge, this training could be associated with professional counselling for these individuals to make some dietary modifications accordingly, like consuming more fat than carbohydrates. Therefore, an adequate understanding of RER-related concepts is crucial for the proper construction of training programmes that focus on certain energy systems to fulfil the metabolic requirements for that specific training.
The findings of the current study suggested that the knowledge of future doctors regarding concepts related to exercising at high altitudes is lacking. Practising exercise at high-altitude environments may be associated with some physical challenges such as reduced temperature and atmospheric pressure, hypoxia and higher levels of solar radiation. 35 Such changes are linked to adverse consequences on the human body, such as skeletal muscle size loss that can result in a corresponding body mass reduction. 35 On the other hand, recent studies have demonstrated that exercising at high altitudes provides various advantages for both athletes and residents. Training at high altitudes increases oxygen transport, enhances aerobic capacity, and stimulates erythropoietin production. It is common for athletes to use a periodisation strategy, which involves living at high altitudes and training at low altitudes to maintain optimal training conditions. 36 Health professionals, possessing good knowledge in this aspect may offer valid medical advice to individuals who are exercising or living at high altitudes on the way they exercise or live to accommodate these physiological changes associated with high altitudes. For example, to avoid overexertion, physicians may need to advise individuals who will be going to or residing at high altitudes to take more frequent breaks or engage in less intense exercise. Physicians may also need to advise patients on how to protect themselves from increased exposure to ultraviolet radiation, such as by wearing protective clothing and sunscreen. Additionally, having awareness of medical disorders that are related to high altitudes, such as pulmonary/cerebral oedema and acute mountain sickness 37 helps physicians to expect, diagnose, and treat those disorders once they happen and thus save the lives of patients. As a consequence, doctors having proper awareness of the physiological changes that take place at high altitudes and how they may impair physical activity will provide better care for those individuals who are active at high-altitude environments. Furthermore, our analysis revealed that participants who were married and residing in villages demonstrated a higher level of knowledge in exercise physiology compared to their unmarried and urban counterparts. The enhanced knowledge of exercise physiology observed among married participants is probably due to a greater exchange of information in the context of a spousal relationship. Exercise physiology may be more understandable under the influence of spouses or participating in shared activities. Additionally, the potential presence of community-based programmes or local health initiatives may be connected to the higher knowledge levels among the villagers. Compared to bigger urban areas, village settings frequently generate close-knit communities where health-related information is shared and disseminated more efficiently.
In the current study, most participants reported that they have sufficient knowledge to counsel a patient on exercise prescription in the future which contradicts with findings of the current study. Another contradiction observed is that most respondents agreed to the statement pointing to the importance of improving the MD curriculum in terms of exercise physiology. These differences in responses may be due to variations in self-assessment and individual perceptions since previous studies in the literature suggest that self-assessment is a multifaceted process influenced by various cognitive and social factors.38–40 Therefore, it is possible that participants’ perceptions of their own knowledge differ from what the questionnaire measures objectively.
The findings of this study regarding awareness and knowledge of exercise physiology have a number of practical implications such as:
Knowledge gaps in exercise physiology can be problematic not only in terms of prescribing exercise and counselling patients, but it can also hinder student’s perception of normal physiological mechanisms and subsequently the diagnosis and management of medical disorders. A thorough understanding of respiratory, cardiovascular, metabolic and energy systems is crucial to comprehend certain pathophysiology of several medical disorders and their treatment. By analysing exercise physiology knowledge among MD students, areas of weakness can be identified, and targeted educational interventions can be incorporated into the curriculum to improve it. This will increase awareness of exercise physiology among future physicians.
Physicians with adequate knowledge of exercise physiology will likely prescribe exercise regimens adequately, promote physical activity, and manage patients affected with exercise-related health problems.
Facilitating interdisciplinary collaboration between healthcare professionals, promoting effective communication and incorporating exercise as a preventative and treatment component.
Study limitations
Despite being the first study exploring and investigating the misconceptions regarding exercise physiology knowledge among undergraduate MD students in Jordan, this study potentially has some limitations. For example, using a self-reported survey, respondents may inaccurately understand or respond to certain questions due to cognitive limitations. Additionally, there is a possibility that participants will provide information based on memory, which could introduce recall bias. Another potential limitation of the current study could be that data collection using online platforms is possibly associated with disparities in access to survey. Despite these limitations, the use of online self-reported questionnaires remains a valuable tool in many research contexts.
Conclusion
In conclusion, this study found that Jordanian undergraduate MD students during their clinical clerkship held misconceptions and inadequate awareness of key principles in exercise physiology. Therefore, efforts must be made to increase awareness and improve knowledge about basic physiological fundamentals related to exercise physiology among medical students in Jordan, as they represent the backbone of healthcare professionals of the future who will deal with medical conditions related to physical activity and exercise. As a result, educational organisations may customise some educational programmes to enhance the exercise physiology knowledge of future healthcare providers and make sure that they are well-prepared to address the growing significance of exercise for improving health and managing disease.
Footnotes
Acknowledgements
The authors would like to thank the MD students who took part in this study for sharing their time and experience.
Author contributions
IA: Conceptualisation. IA, YA, MMA: Data analysis. IA: Project administration & Supervision. IA, YA, MMA: Resources & Software. IA, YA, MMA, AKO, ME, MA: Writing – original draft. IA, AKO: Writing – review & editing. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Hashemite University Institutional Review Board (IRB) Committee (No. 26/2/2022/2023).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.