
Abstract
Background
Congenital heart disease (CHD) is the most common birth defect worldwide, and left untreated may cause significant morbidity and mortality. Hemodynamically significant CHD requires early diagnosis and surgical correction to prevent mortality and allow for normal development.
In Guyana, there has historically been a lack of access to the diagnostic tools and medical expertise necessary to assess and manage CHD. Many children with CHD in Guyana suffer recurrent illness, abnormal development, poor quality of life, and early death. 1
In the past, a small number of Guyanese children with CHD were sent abroad for surgery, most often to India. The majority of these patients received funding from charitable organizations that provide financial support to critically ill children. Unfortunately, the lack of physicians trained in pediatric cardiology and echocardiography resulted in children being sent overseas with an incorrect diagnosis or inoperable disease. Patients had virtually no follow-up after returning to Guyana postoperatively, including those who had undergone palliative procedures or would be expected to require additional interventions later in life. With no triage system in place, funds were allocated to patients who happened to be referred or who had better access rather than those most in need.
With the support of the Libin Cardiovascular Institute of Alberta at the University of Calgary, the Guyana Echo Education Program was instituted in 2012. The program established a fully functioning echocardiography lab at the Georgetown Public Hospital Corporation (GPHC) and trained local physicians to perform and interpret echocardiograms. While the program was initially targeted toward providing adult echocardiography, an urgent need was identified to provide diagnosis for pediatric patients with cardiac disease. In the span of 1 year, 70% of pediatric echocardiograms performed at the GPHC revealed significant abnormalities, highlighting the burden of underdiagnosed CHD. 2 To address this need, under the direction of faculty from the Libin Cardiovascular Institute, local pediatricians were educated in echocardiography and basic pediatric cardiology. The GPHC pediatric cardiology clinic was then established and the Guyana Paediatric Cardiology Steering Committee (GPCSC) was formed to review and triage patients requiring surgery so that those most in need might receive timely intervention. The clinic is open to the entire population of Guyana through the public health system without cost to the patient. The Ministry of Public Health of Guyana has undertaken to publicize the availability of this service to all urban and rural areas, and agreed to facilitate transportation of remote rural patients to GPHC for assessment and management.
A partnership was developed with the International Children’s Heart Foundation (BabyHeart), a non-governmental agency based in the United States. BabyHeart, under the direction of an experienced pediatric cardiac surgeon/CEO of clinical operations, travels with a team of pediatric cardiology, surgical, and intensive care experts to developing countries to perform pediatric cardiac surgeries and cardiac catheterization–based diagnostics and interventions. Their goals include education of local health care professionals, thus assisting in building capacity for sustainable pediatric cardiac care.
Under the new program, all pediatric patients with cardiac pathology are seen at the GPHC pediatric cardiology clinic, triaged by GPCSC, and reviewed with BabyHeart and Libin Cardiovascular Institute faculty. Decisions regarding medical management, additional investigations, and timing and type of intervention are made on a case-by-case basis by a multidisciplinary team. Under this system, cardiac surgeries, cardiac catheterizations, and catheterization laboratory–based cardiac interventions are undertaken locally by the BabyHeart team. All patients are followed at the GPHC pediatric cardiology clinic by the local echocardiography-trained pediatrician, under direct and/or remote supervision of Libin Cardiovascular Institute faculty.
Study Objectives
To assess the impact of the Echocardiography Education Project, the GPHC pediatric cardiology clinic, and the GPCSC on outcomes in Guyanese children with CHD.
To gain an understanding of the features of CHD in this developing nation by collecting observational data on all pediatric patients with CHD referred to GPHC.
Methods
A retrospective cohort study was undertaken to compare the characteristics and outcomes of children with CHD in Guyana before and after the implementation of GPCSC.
Population
Patients in the pre-GPCSC cohort were diagnosed with CHD prior to the creation of GPCSC and were sent abroad for surgery with the aid of one or more charitable foundations and government funding. Patients included were younger than 18 years at the time of initial surgery and had complete demographic information available. This cohort includes patients sent for surgery from 2005 to 2014, details which have been presented previously. 1
Patients in the post-GPCSC cohort were identified to have CHD after the implementation of GPCSC and were diagnosed, triaged for surgery, and followed through GPCSC. Patients were included if they were younger than 18 years, had consent provided by a parent or guardian, and underwent cardiac surgery or a therapeutic catheterization lab intervention from February 2014 and July 1, 2016. This time period was selected as a convenience sample and is representative of the patients referred to GPCSC during its first 2 years of operation.
Patients who had initial diagnosis and surgery prior to GPCSC but were later referred to the clinic were included in the pre-GPCSC cohort. For a brief period in 2014, during which time GPCSC was functioning, a small number of patients were still being sent for surgery by charitable foundations without involvement of GPCSC. Patients from this time period were allocated according to whether or not they had been seen and triaged by GPCSC.
Ethics approval was granted by the University of Calgary Conjoint Health Research Ethics Board (CHREB) and the Research Ethics Committee of the Guyana Ministry of Public Health.
Variables
For both cohorts, data were collected on demographics and documented postoperative follow-up. When available, note was made of mortality and need for additional surgical intervention.
Data on the pre-GPCSC cohort were primarily obtained from the records of the charitable foundations that facilitated the surgeries. 1 A substantial number of the patients from the pre-GPCSC cohort had information missing, including date of birth, age at surgery, and final diagnosis. Patients with unknown date of birth were excluded and those for whom no follow-up information was available were assumed to have had no cardiology or echocardiography follow-up.
For the post-GPCSC cohort, as well as pre-GPCSC patients subsequently followed through GPCSC, data were extracted in an anonymized fashion from the clinic’s electronic medical record and database.
A qualitative comparison was made of the descriptive statistics of the 2 cohorts.
Results
In the pre-GPCSC cohort, 88 patients were identified as being sent abroad for surgery between 2005 and 2014. Twenty-one patients had no recorded date of birth and were excluded from the comparative analysis. Complete data were available for 16 (23%) patients, with partial data for 51 (77%) patients. Of the pre-GPCSC cohort, 9% are known to be deceased, and 43% are known to be alive. Vital status of the remaining 48% (42 patients) is unknown. Of the pre-GPCSC patients known to be alive, 95% have subsequently had follow-up through GPCSC.
Twenty-five percent of the pre-GPCSC cohort had a pre-operative diagnosis different from their final diagnosis (Table 1). Nineteen patients were sent abroad but did not undergo surgery; 4 (21%) due to inoperable disease or misdiagnosis and 15 (79%) for unknown or other reasons (Table 1).
Summary of Patients, Including Patients Referred for Surgery Who Did Not Undergo Surgery of the Pre-GPCSC Cohort.

Abbreviations: GPCSC, Guyana Paediatric Cardiology Steering Committee; HIV, human immunodeficiency virus.
Since the inception of GPCSC, 319 patients have been referred for assessment and management of CHD. A total of 114 were identified as requiring surgical or catheterization procedures and of these, 74 patients were prioritized to receive interventions through BabyHeart within the study period. Seventy-six interventions were performed, with 60 surgical procedures and 16 interventional catheterization procedures in 74 patients. Seventy (95%) of these patients are currently alive (Table 2). Of the 4 patients who died postoperatively, 2 were early (within 30 days) postoperative cardiac-related deaths, and 2 were late postoperative (>30 days). Of the late postoperative deaths, 1 was cardiac related and 1 was noncardiac in etiology. Complete data on all patients in the post-GPCSC cohort is available and no patients were lost to follow-up.
Average Age (Ranges) at Time of Diagnosis and Intervention, Number of Postintervention Follow-up Visits and Echocardiograms and Mortality of the Pre- and Post-GPCSC Cohorts.

Abbreviations: GPCSC, Guyana Paediatric Cardiology Steering Committee; N/A, not available.
Known to be alive.
The cardiac pathology of patients in both the pre- and post-GPCSC cohorts is detailed in Table 3.
Cardiac Pathology and Mortality of Patients Who Received Intervention in the Pre- and Post-GPCSC Cohorts.
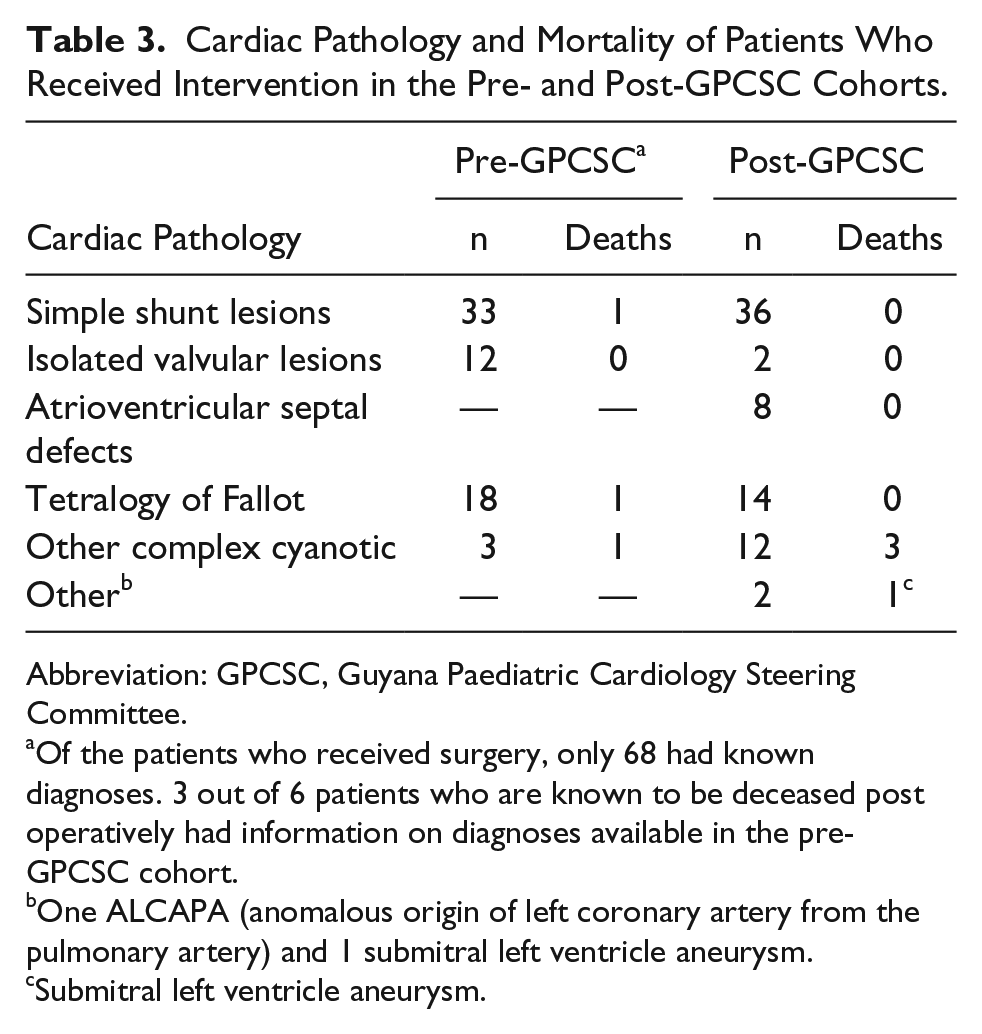
Abbreviation: GPCSC, Guyana Paediatric Cardiology Steering Committee.
Of the patients who received surgery, only 68 had known diagnoses. 3 out of 6 patients who are known to be deceased post operatively had information on diagnoses available in the pre-GPCSC cohort.
One ALCAPA (anomalous origin of left coronary artery from the pulmonary artery) and 1 submitral left ventricle aneurysm.
Submitral left ventricle aneurysm.
There was no difference in age at time of surgery between the pre- and post-GPCSC cohorts with a mean of 77.0 months at time of first surgery (Table 2). More patients post-GPCSC received appropriate follow-up, including echocardiograms postoperatively (Table 2). In the pre-GPCSC cohort, none of the patients received echocardiograms unless they were subsequently followed up at GPCSC. In the post-GPCSC cohort, all patients surviving to hospital discharge received follow-up visits and echocardiograms (Table 2).
In the pre-GPCSC cohort, 16 (24%) of all patients (55% of those children we were able to identify and assess) were found to have required additional intervention following their primary surgery. Of these, 2 had disease progression rendering them inoperable by the time that they were assessed, and 6 have received subsequent intervention through GPCSC. An additional 8 children are either on the waitlist for intervention, or being followed for appropriate timing of additional intervention. In the post-GPCSC cohort, 7 children required planned repeat intervention, 3 of whom have received this intervention, and 4 of whom were being followed for appropriate surgical timing at the end of the study period.
Discussion
Prior to the implementation of the GPCSC, children were sent abroad for surgery without triage, failed to receive appropriate follow-up, and had a greater likelihood of mortality postoperatively. After the establishment of GPCSC, patients were triaged appropriately for intervention, all patients received follow-up and echocardiograms, and patients experienced greater survival rates postoperatively.
In the pre-GPCSC cohort, 88 patients were sent for surgery; however, only 67 patients (76%) received the planned intervention. A total of 68 interventions were performed in the span of 8 years (2006-2014). In the post-GPCSC cohort, 76 prioritized interventions were performed on 74 patients in the span of 20 months (January 2014 to July 2016). None of the patients in the pre-GPCSC cohort were systematically triaged for surgery. For instance, children who required tetralogy of Fallot repair were given the same priority as those requiring atrial septal defect repair. In contrast, all patients in the post-GPCSC cohort were triaged by specialists, with higher priority given to patients with advanced or time-sensitive pathology.
While the sample sizes between the pre- and post-GPCSC cohort are similar, complete data was unavailable for 77% of the patients in the pre-GPCSC cohort. Lack of appropriate documentation and follow-up in Guyana resulted in 42 patients (48%) being lost to follow-up. In contrast, all patients in the post-GPCSC cohort have complete data and none have been lost to follow-up.
The post-GPCSC cohort had a lower mortality rate (5%) than the pre-GPCSC cohort (9%); however, the pre-GPCSC postoperative mortality rate was likely underestimated due to loss to follow-up of 42 patients (48%). It was initially assumed that earlier age at time of diagnosis and intervention would be the primary outcome drivers for increased survival rates in the post-GPCSC cohort; however, the mean age at time of diagnosis and intervention were similar between the pre- and post-GPCSC cohorts. For purposes of this study, age at time of diagnosis was defined as the first medical documentation in which the patient was recognized to have CHD. Age at time of diagnosis was often difficult to ascertain accurately in the pre-GPCSC cohort due to poor documentation. In the post-GPCSC cohort, patients were often referred at an older age, either due to incidental findings or symptoms resulting from progression of CHD. It is likely that many patients suspected to have CHD were not sent for diagnosis or management prior to GPCSC due to lack of access and only came to medical attention once the GPCSC was implemented.
Average age at intervention was also similar between the pre- and post-GPCSC cohorts. In the post-GPCSC cohort, patients that were triaged to receive surgery immediately were often older patients with advanced pathology, in whom withholding or delaying surgery could result in an inoperable state. This too was likely a reflection of the lack of knowledge and access to diagnostic expertise for CHD prior to GPCSC, and delay in recognition of the availability of public expert care, resulting in patients being referred at a later age. These factors contributed to the similarity of age at time of intervention in the pre- and post-GPCSC cohorts.
A more instructive indicator may be the age ranges for time of diagnosis and intervention. With availability of echocardiography and developing local cardiac expertise post-GPCSC, there were more neonates and infants identified with significant CHD who were appropriately treated. These patients received definitive repair or hemodynamic palliation within recommended timelines. The youngest patient diagnosed in the post-GPCSC cohort was 1-day old, in comparison to 2 months of age in the pre-GPCSC cohort. The youngest patient to receive intervention in the post-GPCSC cohort was 3.4 months of age compared with 5.8 months in the pre-GPCSC cohort.
Since the pre- and post-GPCSC cohorts had similar average age at diagnosis and intervention, other factors must have contributed to increased survival in the post-GPCSC cohort. These likely include expert preoperative management, appropriate surgical triage, routine postoperative follow-up including echocardiography, timely management of complications, increased patient and parent education regarding postoperative care, and triaging for repeat intervention.
Correction of complex cyanotic pathology is technically challenging, involves an increased level of risk, and often requires additional interventions. More patients in the post-GPCSC cohort received surgical intervention for complex cyanotic cardiac pathology as compared with the pre-GPCSC cohort (Table 3). The availability of diagnostic tools, expertise, and appropriate follow-up as well as triage for appropriate prioritization now allows for proper management of these complex patients.
Limitations
While the post-GPCSC cohort represents a reasonable cross-sectional sample of the population of Guyana with CHD, the pre-GPCSC cohort does not. Children sent for surgery in the pre-GPCSC cohort would have had the financial means to pay for what limited investigations were available and the social, political, and financial opportunities to advocate for funding. This suggests a bias toward children from an urban setting, from families with higher socioeconomic status. The GPCSC operates through a publicly funded hospital with an open referral system and as a result is more likely to provide care to a broader population base. However, despite the open-access referral system and attempts to disseminate the availability of GPCSC by the Ministry of Public Health, children in the remote regions of Guyana are likely to be underrepresented.
Guyana is divided into 10 geographical regions, with the majority of the population concentrated in the urban regions, located on the coast. GPCSC operates out of the Georgetown Public Hospital Corporation, the country’s only public tertiary care hospital, located in Region Four, where 41% of the population resides. The remainder of the population resides in the more remote inland regions of Guyana. Travel from remote regions is often a multiday trip, requiring travel by road and boat. Therefore, the geography of Guyana poses challenges to accessing and providing care to inland populations.
Over time, GPCSC has received an increasing number of referrals; however, there is a relative lack of referrals from remote rural health clinics and from the private health care centers in Georgetown. Contributing to this is the lack of knowledge regarding identification of CHD among Guyanese health care providers. Similarly, there is inadequate awareness of the expertise and free services that GPCSC provides. There may be reluctance on the part of private healthcare providers to refer to the GPCSC, since this could be construed as an acknowledgment of their lack of expertise in pediatric cardiology. Finally, there may be reluctance of patients to utilize the free services provided by GPCSC as this would conflict with the cultural notion that private health care is a premium service, and therefore superior to the public system.3,4
An issue identified during this study was the systemic lack of data, ranging from public health data in Guyana to data on patients with CHD diagnosed before the creation of the GPCSC. For some patients, the only information available was name and date sent for surgery, with no data on age, diagnosis, or surgical procedure performed. 1 The poor quality of information is consistent with a low level of expertise and lack of standardized records for delivery of health care in Guyana, in particular in the care of children with CHD. 5 This also illustrates the lack of robust public health data in Guyana, which results in inadequate accountability in the healthcare system and leads to gaps in healthcare delivery and planning. 5 In contrast, there has been and will continue to be, complete data available for all children followed through GPCSC.
Future Directions
Future research projects examining demographics of patients managed through GPCSC will be vital. This will help guide future policies and improvements that must be made in order to provide a higher standard of health care. Identification of barriers to referral to GPCSC by staff and patients will be crucial. Knowledge of these obstacles will allow for development and collaboration with health care staff and patients to create a more unified approach to pediatric cardiac care in Guyana.
Despite the advances made by the development of the GPCSC and partnership with BabyHeart, there remain some forms of complex congenital heart disease that are not amenable to rescue by regular scheduled surgical/interventional missions. Fortuitous presentation at the time of such missions allows for timely intervention, but otherwise these children perish. Ongoing education and development of local capacity for urgent interventions is even more critical for these children.
The obstacles to providing care in Guyana will be challenging to overcome, particularly nonmodifiable factors such as geography. The best approach will be to target upstream modifiable factors. While the Ministry of Public Health of Guyana has been supportive in spreading awareness of the GPCSC’s services, the problem may lie with lack of knowledge of rural health care providers of how to identify when a referral to GPCSC is indicated. An educational campaign aimed at teaching providers about symptoms and physical findings consistent with CHD may allow for early referral to GPCSC and subsequently lead to earlier intervention and improved outcomes.
Author Contributions
DI (senior author): research design and funding, supervision of implementation and analysis, manuscript collaboration, review and revision.
VN: research implementation, data collection, analysis, manuscript writing.
AB: research design, analysis and manuscript collaboration.
RS: research design assistance, manuscript collaboration.
MS: data collection (local contributor), manuscript collaboration.
KM: research design, analysis and manuscript collaboration.
SZ: database development, data collection and analysis, manuscript review.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge that funding for this study was provided through research grants from the Libin Cardiovascular Institute of Alberta at the University of Calgary, and from Global Health and International Partnerships, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.