
Abstract
Concussions are a major cause of morbidity in pediatrics. Many concussions occur during activities with emergency medical service (EMS) providers present to determine if a higher level of care is needed. Data are limited on how capable these providers are. We assessed the ability of EMS providers to recognize pediatric concussions. Fifty-six total responses were included, 38 from EMS and 18 from our MD/RN (medical doctor/registered nurse) group. No statistical differences were found between the 2 groups when adjusted for age, gender, number of years in practice, and number of pediatric concussions managed. This first of its kind pilot study was designed to assess EMS personnel’s ability to recognize and triage pediatric concussions. Our findings show EMS providers are statistically identical in their ability to recognize and triage concussions to physicians. The performance of our MD participants was lower than expected. Larger studies are needed to further investigate EMS providers’ ability to recognize a concussion.
Keywords
Introduction
There are approximately 1.6 to 3.8 million concussions diagnosed each year in the United States. 1 These figures are estimated to understate the total number of concussions, accounting only for patients who seek medical care. 2 Thirty-eight million children and adolescents play in organized sports in the United States, a known risk factor for concussions.3,4 Concussion symptoms are often misinterpreted by patients and their families as the symptoms are nonspecific in nature. 5 If a concussion is suspected, many athletes report not seeking medical attention assuming the injury is not severe or trying to avoid being pulled from the game. McCrea et al suggest that a significant number of pediatric concussions go either unrecognized or untreated, increasing the risk of serious long-term consequences. 6 Additionally, there is a misperception that pediatric athletes are more resilient to head injury; however, as their brains are still developing, children are more susceptible to the effects of head trauma. 1 And despite common belief, it has been shown that concussions are more common in high school than in collegiate athletic activities. 7 It is clear that untreated concussions can potentially have both short- and long-term effects. Failure to remove a concussed player from a game can lead to second-impact syndrome, or diffuse cerebral edema secondary to a second head injury prior to full recovery. 8 Studies have shown that there are long-term deleterious effects to concussions as well. These include postconcussion syndrome, presenting with the persistence of fatigue, poor sleep, headaches, dizziness, and mood and personality disturbances. 9 Additionally, it has been shown that patients with concussions have persistent deficiencies on neurophysiological testing and poorer academic achievement.10,11
Due to the potential sequelae of concussions, it is critical to make an early diagnosis and initiate appropriate management. Early symptom recognition allows for appropriate treatments, including removal of the patient from the game/sport until symptoms resolution and completion of the appropriate return to play regiment. 12 For this to occur it is critical for physicians and first responders properly recognize the signs and symptoms of pediatric concussion.
No prior study has assessed emergency medical service (EMS) personnel’s ability to recognize and triage pediatric concussions. The purpose of this study is to serve as a pilot study to assess El Paso EMS personnel’s comprehension of pediatric concussions and knowledge of appropriate early management practices.
Methods
An assessment tool was developed to assess comprehension of the Centers for Disease Control and Prevention criteria for clinical diagnosis of concussion and of initial treatment steps. 5 This survey included demographic questions, questions assessing the respondent’s confidence in managing pediatric concussions, and questions assessing the respondent’s ability to recognize pediatric concussion presentations, symptoms, severity, and their ability to appropriately triage pediatric concussions. Eight case presentations were provided, requiring respondents to determine if a concussion was present and if the patient needed further evaluation. Presentations included both scenarios where a concussion was present and was not present. Four questions asked the surveyed to identify symptoms of concussion from multiple choices. A response of “I don’t know” was not included as an answer choice option as clinical situations require a decision to be made. We used the “Sports-Related Concussion in Children and Adolescents,” from the American Academy of Pediatrics (AAP); Centers for Disease Control and Prevention “What are the Signs and Symptoms of Concussion”; and “Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators” from Carney et al to build evidence-based case presentations and questions where the correct answer could clearly be elicited using the AAP guidelines.1,5,13 The survey is provided in the appendix. The assessment was administered using Qualtrics, an online survey tool distributed by email.
With permission from the El Paso Fire Department’s medical director, the survey was emailed to all registered fire department EMS personnel, including EMT-Bs, EMT-As, and EMT-Ps, who are the 911 emergency responders in the El Paso, Texas, area. Additionally, the survey was distributed to emergency medicine physicians at Texas Tech University Health Science Center El Paso Paul L. Foster School of Medicine as well as to pediatric physicians and nurses at El Paso Children’s Hospital. We obtained institutional review board approval from each institution included in this study.
The results of the study were analyzed with the primary goal to compare the responses of our EMS personnel to our physician/nurse cohort that was trained in concussion recognition and diagnosis. All statistical analyses were performed by the Texas Tech Biostatistics Department. Continuous data were described using mean and standard deviation (SD), while categorical data were described using frequency and proportion. Continuous data were compared according to profession (EMS, MD/RN [medical doctor/registered nurse]) using unpaired t test. Categorical variables were compared according to profession using Fisher’s exact test. Results with P value less than or equal to .05 were considered as statistically significant. Statistical analyses were conducted using SAS version 9.4 (Cary, NC).
Results
Participants
Of the approximately 950 surveys emailed, 56 (5.6%) were received in total, with 38 from our EMS group and 18 from our MD/RN group. The EMS group included 20 EMT-Ps, 1 EMT-A, and 17 EMT-Bs. Our MD/RN group included 10 MDs (6 pediatricians, 1 pediatric emergency medicine physician, and 3 emergency medicine physicians) and 8 RNs. Both groups had similar characteristics (Table 1), with the exception of the EMS group responding entirely as male. The mean respondent age was 41.49, had an average of 13.55 years in practice, and managed an average of 6.36 pediatric concussions per year. Fifty-eight percent of physicians and 65% of EMS personnel reported receiving prior education on concussions. The EMS group did report greater self-rated ability to both treat and manage pediatric concussions at 6.68 and 6.94, respectively, as compared to our MD/RN group at 4.29 and 4.75 (P < .05, P < .05).
Comparison of Variables According to Profession, Using EMS, MD, and RN Survey Data (n = 57).

Abbreviations: EMS, emergency medical service; MD/RN, medical doctor/registered nurse cohort.
Concussion Recognition and Response
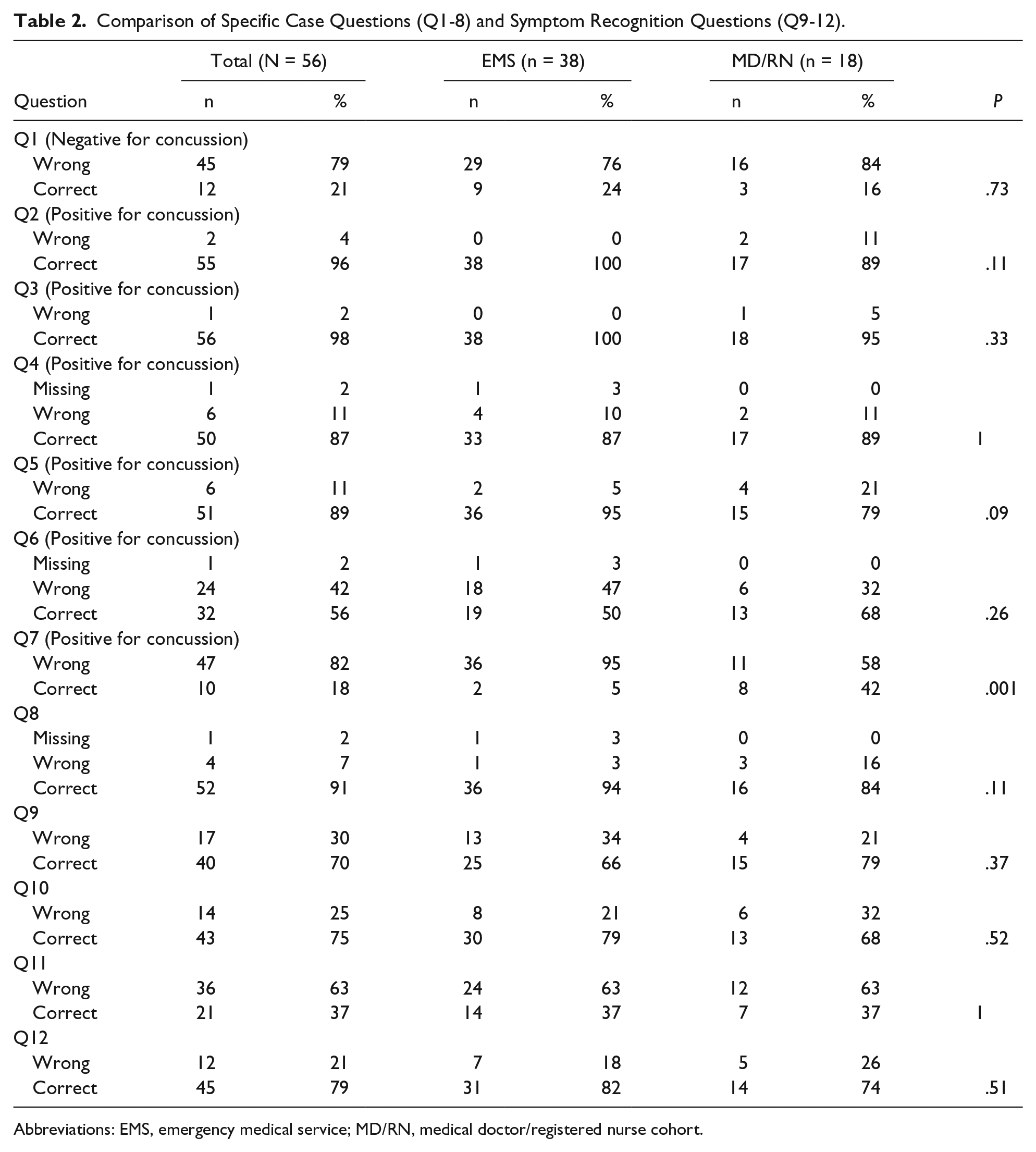
Respondents in both groups correctly answered an average of 8.19 of the 12 concussion recognition and response questions, with no statistically significant difference between the EMS and MD/RN groups (P = .9428). Individual analysis of each question is provided in Table 2. There were no statically significant differences between the 2 groups on any individual question except question 7, where 5.26% of the EMS group and 57.89% of the MD/RN group appropriately recognized and responded to a positive concussion case scenario (P ≤ .013). Additionally, on the two questions with the lowest correct response rates, questions 1 and 11, correct response rates were 21.05% and 36.84%, respectively, with no statistically significant differences between the 2 cohorts (P = .732, P = 1). There were no differences between the 2 groups in how severe concussions were rated.
Comparison of Specific Case Questions (Q1-8) and Symptom Recognition Questions (Q9-12).
Abbreviations: EMS, emergency medical service; MD/RN, medical doctor/registered nurse cohort.
Adjusted Differences
We looked at adjusted association between profession and overall corrected responses on pediatric concussion shown in Table 3. When examining the impact of age, gender, number of years in practice, previous concussion education, and number of pediatric concussions managed per year, and progression (MD/RN vs EMS), there were no statistically significant factors corresponding with overall corrected responses to our questions. Age and previous concussion education approached statistical significance (P = .1001, P = .1262, respectively), but the effects were small (regression coefficient [RC] = 0.047, RC = 0.625, respectively).
Adjusted Association Between Profession and the Overall Corrected Response on Pediatric Concussion.

Abbreviations: RC, regression coefficient; CI, confidence interval; EMS, emergency medical service; MD/RN, medical doctor/registered nurse cohort.
Discussion
Current literature has shown that early diagnosis of concussion in pediatric patients is critical to initiating early treatment and preventing possible devastating sequelae. As concussions frequently occur during sporting events, often it is the parents, coaches, and athletic trainers who are the first to assess an injured child. Prior surveys of parents, coaches, and athletic trainers have shown that many lack knowledge of concussion symptoms and treatment, showing a need for additional concussion-related education.14,15 Additionally some surveys have shown that only 37.5% of coaches referred their concussed players to an emergency department, 16 likely due to poor on-field concussion assessment and management leading to many missed concussions. 17 Among physicians, a study in 2015 reported that pediatric emergency physicians “diagnosed concussion less often relative to international consensus-based guidelines” leading to concussions being underdiagnosed. 18 When medical students were surveyed, most reported never having had any formal didactic education on concussion and lacked clinical exposure to concussion management. 19 Although the data on how EMS providers perform on similar measures is limited, it would not be unreasonable to think that they would mirror emergency medicine physicians in the underdiagnoses of pediatric concussions. There seems to be a global lack of education with regard to concussions in children.
Our study showed that 58% of the physician/nurse group and 65% of the EMS group have had prior education on concussions (P = .57). Although this may be concerning for medical educators, it is encouraging that the EMS personnel report having had statistically similar levels of exposure to concussion education as their hospital colleagues. This prior education likely played a role in the overall ability of our EMS cohort to diagnosis and triage pediatric concussions when assessed. In this study, EMS responders correctly recognized the signs of concussion and chose the appropriate initial course of action, with comparable results to the physician-nurse cohort. Additionally, it is interesting that although EMS personnel report seeing less than 25% of the concussion volume that physicians and nurses report treating, they expressed increased confidence in their ability to treat and manage concussions. These findings may be related to an increase in efforts to disseminate concussion awareness and education in the medical community.
These findings suggest that in El Paso, Texas, both prehospital and hospital providers alike are able to recognize and triage pediatric concussions when assessed and that emergency response personnel are being well trained on concussion management. This is reassuring as physician coverage at sporting events is limited, and EMS providers are often the first to assess many sports-related injuries. These findings suggest that prior educational efforts directed to this cohort improve awareness of concussions and early recognition. Additionally, our findings suggest that the presence of emergency response personnel at sporting events may lead to more accurate triaging of concussions and lead to fewer missed diagnoses.
This study adds to the growing body of evidence that physicians continue to miss symptoms of traumatic brain injuries. When looking only at the ability of the physician (MDs) cohort to recognize symptoms of a concussion, only 40% of physicians correctly answered all 4 questions requiring correct identification of a symptom of a concussion, with 25% of all physician response incorrect on these 4 questions. This seems to expose an area of weakness in both the initial and continuing education of physicians and posits that current pediatric physicians in this cohort may not be keeping pace with current medical literature. Zonfrillo et al published similar findings concluding that providers “may not have adequate training or infrastructure to systematically diagnose and manage” concussed patients. 20 These findings are alarming as they likely support the growing evidence that children with concussions are being undiagnosed, untreated, and at being placed at risk for significant life altering consequences.
Our study has certain limitations. As with any study relying on individual’s willingness to complete a voluntary survey, there is the potential for an uncorrected selection bias. Due to the limited number of surveys completed, the study was potentially underpowered, limiting our ability to better define potential differences among our study groups. Additionally, this study relied on an assessment that had not previously been validated.
Conclusion
This is the first study to assess the knowledge of concussions among emergency response personnel. The El Paso, Texas, region, like many other areas, lacks an adequate number physicians, leading to increased dependency on other provider types. Our data serve as a pilot for further investigations and to show that with concussion education, paramedics and other emergency service personnel can accurately triage pediatric concussions and respond accordingly. A follow-up investigation into the reliability and validity of our EMS provider’s concussion recognition could potentially illuminate more in this area. Additionally, further investigation and action may be necessary to improve continued medical education efficacy on current pediatric practices.
Author Contributions
JNS: Contributed to conception and design; contributed to analysis; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MIL: Contributed to conception and design; contributed to analysis; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
BEJ: Contributed to conception and design; contributed to analysis; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Appendix
Acknowledgements
El Paso Fire Department, for participation in the study; and Justin Wright, MD, and Saul A. Speirs, JD, for critical review of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for statistical analysis by the Texas Tech division of Biostatistics and Epidemiology was provided by the Department of Pediatrics, Texas Tech University Health Sciences Center El Paso.