
Abstract

Introduction
Anticholinergic drug exposure is very common and responsible for 15% to 20% of hospital admissions and up to 40% of intensive care admissions related to acute poisonings.1,2 A well-described anticholinergic toxidrome frequently occurs after exposure to various drugs with anticholinergic properties including antihistamines, atropine, tricyclic antidepressants, jimsonweed, atypical antipsychotics, and scopolamine. 1 These drugs can antagonize both peripheral and central muscarinic receptors to produce anticholinergic toxidrome. Central nervous system manifestations are usually presenting symptoms and include severe agitation, hallucinations, and acute psychosis. Peripheral manifestations often include flushing, dry mouth, dry skin, mydriasis, urinary retention, fever, tachycardia, and hypertension. In severe cases, death can occur due to dysrhythmias.
Supportive care is the mainstay of management of anticholinergic toxidrome including hydration, temperature control, and removal of the offending agent. 3 Patients with delirium and agitation are at risk of self-harm and potential harm to medical staff. These patients frequently require medical therapy with benzodiazepines or benzodiazepines and physostigmine to control delirium and agitation. 3 Benzodiazepines work to control agitation by enhancing the effects of γ-aminobutyric acid (GABA) at the GABA-A receptors, while physostigmine crosses the blood-brain barrier and reverses the toxidrome by reversibly inhibiting acetylcholinesterase. 4 Benzodiazepines have been shown to control agitation in less than 25% of patients and proved ineffective in reversing delirium in these patients. 5 Additionally, benzodiazepines require frequent dosing and can cause significant respiratory depression, resulting in higher rates of intubations in these patients. 5 Physostigmine is an antidote available to treat anticholinergic toxidrome. Physostigmine use is limited for multiple reasons including the need for frequent dosing, unavailability in many centers, lack of familiarity with its use among providers, and certain undesirable side effects including seizure, dysrhythmia, and bowel or urogenital obstructions.3,6 These limitations of benzodiazepines and physostigmine have encouraged physicians to use adjunct therapies to control manifestations of anticholinergic toxidrome.7-9 In this article, we present 2 novel cases of dexmedetomidine use to treat anticholinergic toxidrome, a toddler who is so far the youngest reported case to the best of our knowledge and an adolescent girl who had a relative contraindication to physostigmine use.
Case 1
A 3-year-old, 13.6-kg boy was presented to a local emergency department (ED) with agitation and hallucinations after unintentional ingestion of 10 to 20 tablets (25 mg each) of diphenhydramine. On initial assessment, he was delirious and experiencing visual hallucination. He had heart rate (HR) of 166 beats per minute, respiration rate (RR) of 30 breaths per minute, and blood pressure (BP) of 119/71 mm Hg. Initial laboratory evaluation showed normal routine serum chemistry and negative urine drug screen for amphetamines, barbiturates, methadone, opiates, phencyclidine, benzodiazepines, cocaine, cannabinoids, and ecstasy. Electrocardiogram (EKG) showed normal QRS interval and QT interval.
On arrival to the pediatric ED, the patient’s vitals were BP of 142/92 mm Hg, HR of 158 beats per minute, and RR of 26 breaths per minute. He appeared agitated and was grabbing and scratching at himself. Additional pertinent physical exam findings include pupils dilated to 7 mm and a dry oral mucosa. He received a 1-mg dose of intravenous midazolam to control agitation with a minimal clinical response. Subsequently, he received two 1.5-mg doses of lorazepam in an attempt to control agitation and minimize agitation. The patient remained agitated and continuing to pull off his monitor leads, intravenous (IV) line, and clothes. He was then transferred to the pediatric intensive care unit (PICU) for a possibility of a midazolam IV drip initiation.
On arrival in the PICU, the patient required an intranasal dose of midazolam 6 mg, to help control agitation, while placing a new IV catheter. He developed more notable features of anticholinergic toxidrome (severe agitation, fever, tachycardia, tachypnea, hypertension, and dilated pupils). Physostigmine was considered but was not given due to limited experience of the providing physician and inpatient pharmacist, a need for frequent dosing, and unavailability of onsite toxicologists to guide the therapy. He was started on dexmedetomidine infusion at the rate of 0.5 µg/kg/h. The patient had a dramatic response to dexmedetomidine infusion with control of agitation in 30 minutes. After approximately 10 hours of dexmedetomidine infusion, he had no agitation, normal neurological exam, and normal vital signs (Figure 1). The dexmedetomidine drip was discontinued, and he was transferred out to lower acuity care.
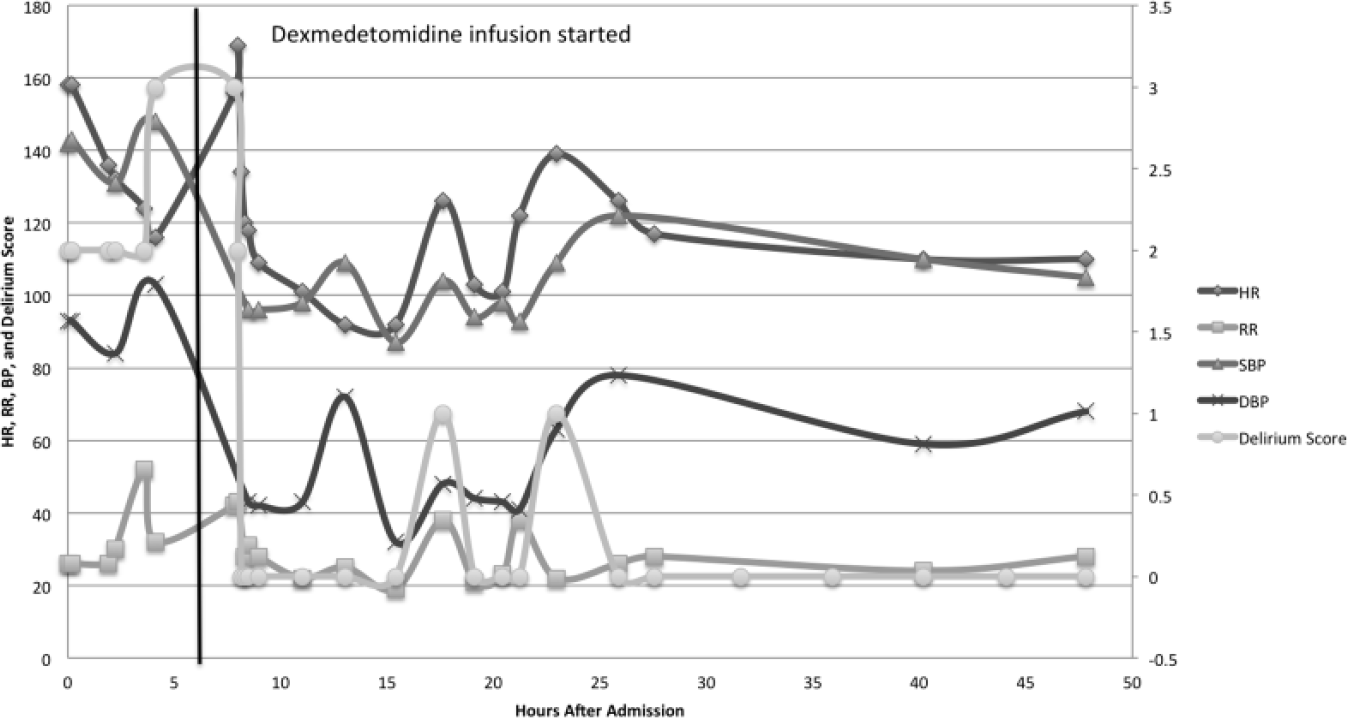
Case 1: Trend of vital signs and delirium score.
Case 2
A 15-year-old, 45.1-kg teenager was brought to the ED for altered mental status after an intentional unwitnessed ingestion of dicyclomine. The patient’s mother found the patient having hallucinations and an empty bottle of dicyclomine (approximately 20-30 tablets). There were also empty bottles of ranitidine and ciprofloxacin. Also, her urine drug test was found positive for cannabinoids. In the ED, she was severely agitated and hallucinating. She was given a 2-mg intramuscular dose of lorazepam after she pulled out her IV line. Her initial vital signs were a temperature of 36.7°C, HR of 64 to 74 beats per minute, and RR of 26 to 29 breaths per minute. However, she remained very anxious, hallucinating, and angry. She had inappropriate speech and behavior. She was placed in soft restraints due to potential self-harm or harm to others. Additional pertinent findings on the physical exam included mydriasis (pupil size 6 mm), abrasions over knees due to thrashing on a gurney, a flight of ideas, and incomprehensible speech. She was given an additional 2-mg dose of intravenous lorazepam. She was then transferred to the PICU for ongoing care.
In the PICU, she had an EKG, which showed the corrected QT interval of 420 milliseconds. Physostigmine was considered but was not given due to the high normal corrected QT interval in a setting of multidrug ingestion, which could have increased her risk for developing bradycardia or asystole following physostigmine treatment. She was started on dexmedetomidine infusion at 0.5 µg/kg/h, instead of physostigmine to control delirium. She responded well to dexmedetomidine with a resolution of agitation and hallucinations within 30 minutes. She did not develop severe bradycardia or hypotension while on the dexmedetomidine infusion (Figure 2). She was weaned off the infusion after 6 hours when her altered mental status resolved and normalization of EKG. She was transferred to a psychiatric facility for inpatient psychiatric care.
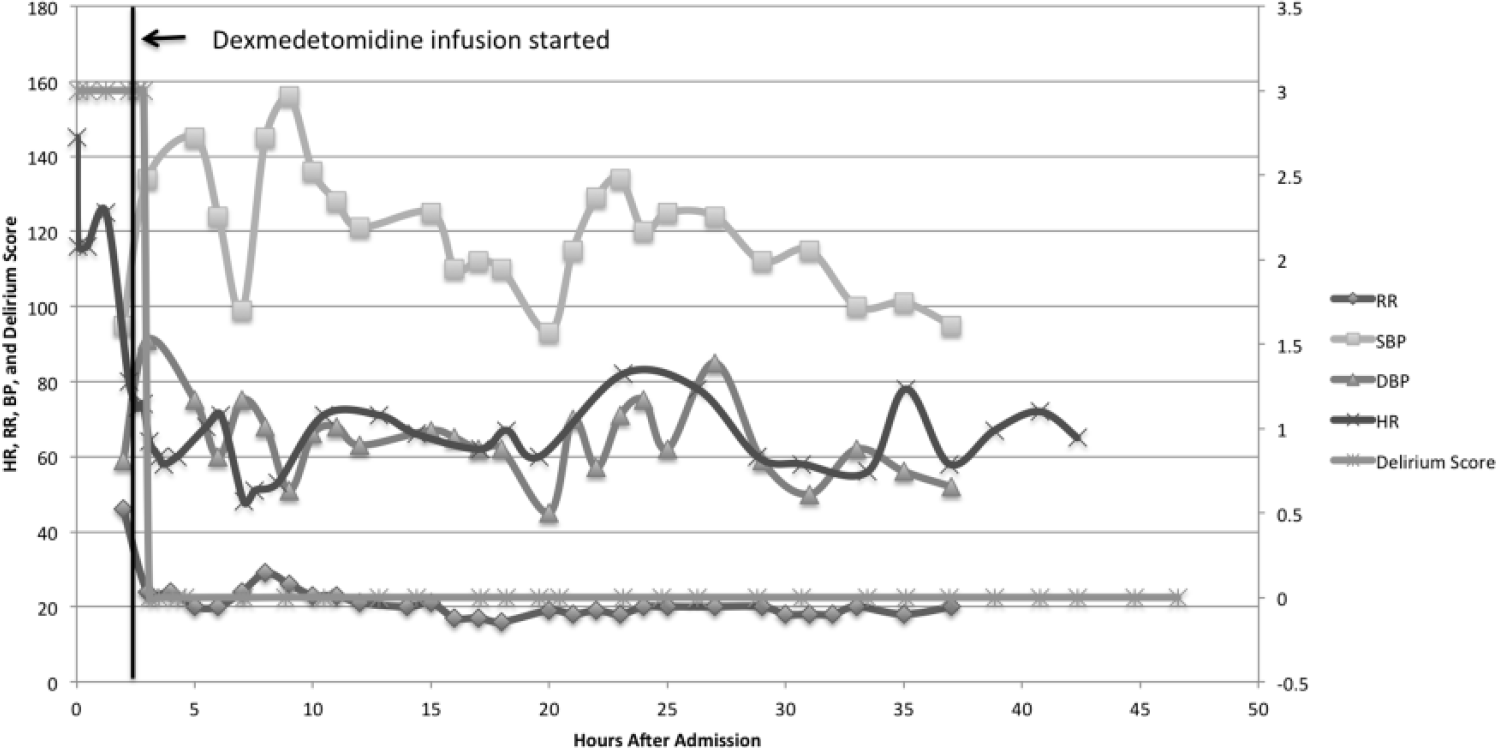
Case 2: Trend of vital signs and delirium score.
Discussion
Our cases demonstrated that dexmedetomidine is an effective adjunctive treatment for anticholinergic toxidrome. In addition to the 2 cases presented in this article, dexmedetomidine has been used successfully to treat 7 other pediatric anticholinergic overdoses cases7-9 (Table 1). Case 1 was the youngest patient to date who received dexmedetomidine to treat anticholinergic toxidrome. Dexmedetomidine successfully controlled both central and peripheral manifestations of anticholinergic toxidrome. Using dexmedetomidine instead of continuous infusion of benzodiazepines allowed treating physicians to avoid respiratory depression and potential intubation as a complication. While in Case 2 dexmedetomidine was used due to relative contraindication to physostigmine use including high normal QT interval and multidrug ingestion with unknown cardiac toxicity profile.
Reported Dexmedetomidine Use in Pediatric Anticholinergic Toxicity Cases.

Physostigmine is an effective antidote to treat anticholinergic toxidrome especially in a clinical severity score of 2 or 3.1,6 However, there is extreme variability in its use among centers across the world related to its availability, local experience, and practice pattern. A review of the Toxicology Investigators Consortium Registry showed that benzodiazepines were prescribed most frequently in 28.7% patients and only 12.4% patients were prescribed physostigmine by toxicologists to control anticholinergic toxidrome. 3 They also found a differential use of physostigmine based on possible causative agents. Physostigmine was used more frequently when the causative agent exerted primarily anticholinergic toxicity as opposed to those agent(s), which exhibit more “mixed” effects. There was a lower rate of intubation but a significantly higher rate of rhabdomyolysis in those receiving physostigmine. There is also significant variability in its dosing regimen ranging from rapid bolus to slow titration. The possibility of excessive cholinesterase inhibition including excessive secretions, bronchospasm, bradyarrhythmias, and seizures are a limitation to its use. Another primary concern is the substantial increase in the risk of seizures and cardiac dysrhythmias with tricyclic antidepressant overdose. 10 The above-described concerns coupled with unfamiliarity with its use among emergency and critical care physicians make physostigmine use sparse in anticholinergic toxidrome.
Dexmedetomidine is a selective α2-adrenergic agonist with sedative, anxiolytic, and analgesic properties. 11 Its sedative and anxiolytic activities are produced by its effects in the locus ceruleous leading to decreased sympathetic outflow with a resultant increased action of the inhibitory GABA neurons. Its analgesic effects are mediated as a result of the release of substance P from the dorsal horn of the spinal cord. Although first approved by the Food and Drug Administration for short-term sedation in mechanically ventilated patients in 1999, dexmedetomidine has increasingly been used for multiple indications. 12 The excellent pharmacological profile with minimal respiratory depression makes dexmedetomidine a reasonable alternative to other sedatives for agitation and delirium associated with anticholinergic toxidrome. Dexmedetomidine’s commonly reported side effects of hypotension and bradycardia offer a significant advantage in controlling peripheral manifestations of tachycardia and hypertension. 13 In contrast to physostigmine, dexmedetomidine may be used safely even in the presence of prolonged QTc. Dexmedetomidine may also diminish the associated fever and flushing by its effect on thermoregulation both centrally and peripherally. Although dexmedetomidine requires continuous monitoring of hemodynamics, its wide availability, minimal effect on respiratory function, ease of titration, and predictable hemodynamic effects support its use as an adjunct therapy for treatment of anticholinergic toxidrome in pediatric patients.
Conclusions
Dexmedetomidine can successfully treat anticholinergic toxidrome and can be a useful adjunct agent, especially in patients at risk of respiratory depression or cardiac toxicity. A larger prospective comparative study is needed to establish its usefulness.
Author Contributions
KC: Contributed to literature review; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RAL: Contributed to literature review; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AS: Contributed to conception; contributed to literature review; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.