
Abstract
Orogastric tube (OGT) procedures are done in 20% of newborn unit cases. This study was contemplated to work out a formula to predict OGT length in terms of femur length in neonates and its agreement to existing standards. In this observational study, OGT length was estimated using NEMU (nose-ear-mid umbilicus) in 53 consecutive newborns. Their anterior superior iliac spine to tibial tuberosity length (AS-TT) was measured and equated using linear regression analysis in Stata. We further verified the accuracy of the new formula and comparison of time taken by both the methods. Strong positive correlation was seen between OGT and AS-TT (r = .88). OGT length was 10.14 + 0.88 AS-TT, which can be used in neonatal intensive care unit newborns with greater accuracy and with lesser time than the classical method. Strong agreement levels were seen. AS-TT closely relates to the femur length and can be chosen as a guide as it is faster when compared to other methods.
Introduction
Short-term orogastric (OG) or nasogastric (NG) tube insertion is a routine procedure in a newborn care unit for short-term assisted feeding in cases of neonates with functional gastrointestinal system. It has got a wide range of functions and is a life-saving measure in such situations. 1 OG or NG tube feeding may be required for every fifth child admitted to the hospital. 2 Orogastric tubes are used also in other cases3,4 such as aspiration of stomach contents, detecting gastric perforation, administer medications, and so on. It is now made mandatory for every intubated patient. Enteral tube feeding is also an effective method for providing nutrients to individuals in different health care settings.5-7
Despite the availability of a number of methods to estimate OG tube lengths, none of the methods have 100% credibility. 8 Various studies have highlighted the risk of misplacing OG/NG tubes despite using accepted methods. Factors such as restlessness and recumbent position often lead to inappropriate positioning of OG tubes. The signs and symptoms of misplaced OG/NG tubes is frequently unnoticed. Aspiration pneumonia may be a consequence of aspiration of minimal quantities of liquid following tube feeding. Tubes with their lower end just above the gastroesophageal junction are responsible for this. On the other hand, tube feedings through a NG/OG tube, which has been placed beyond the stomach probably into the duodenum, can cause nausea and vomiting, abdominal discomfort, dumping syndrome, and diarrhea. Such complications prolong the expected duration of hospitalization and delay the treatment process.8-11
There have been various studies that claim to predict accurately misplaced OG and NG tubes, including some that use weight of the child. 12 NEX (nose-ear-xiphoid), NEMU (nose-ear-mid umbilicus), and ARHB (age-related height-based) have also been used by various researchers. Studies have even shown that direct distance NEX or the reverse measurements in the form of XEN can be replaced by NEMU or the new ARHB equation in neonates, which have better placement. While studies show that NEX is a poor guideline with more risk of aspiration pneumonia due to its inability to reach the mid-stomach, 13 ARHB-formulated equations to estimate NG/OG tube lengths were found to be the best predictors. Only around 3.4% of NG/OG tubes were not placed appropriately in the stomach in the case of ARHB guidelines. 14 In spite of all these, each of these techniques has its own levels of accurately inserting the OG/ NG tube.
The importance of femur length is well recognized as an anthropometric measurement in relation to fetal growth. Various studies have demonstrated its relevance in neonatal anthropometry such as identifying cases of small for gestational age, predicting weight sonographically, predicting trisomy 21, and so on.15-17 Femur length has been shown to have a constant relationship with the patient’s stature. As such femur length is of known significance with a wide range of implications in medical science.
Neonatal intensive care unit (NICU) admissions are generally critically ill patients with majority of them depending on NG/OG tube during initiation of feeding and its continuation over the first few days of life or the need for gastric lavage as per requirement. Being critically ill patients, every step must be taken to do the necessary interventions as quickly as possible without compromising on accuracy. Considering the significance of femur length cited in various neonatal anthropometric studies and being a single measurement, which makes it easily measurable, “AS to TT length (anterior superior iliac spine to tibial tuberosity length)” was considered as an appropriate parameter that could be applied to deduce the OG tube length accurately and quickly. As it may be difficult to measure femur length correctly without going for radiology, the authors have used anterior superior iliac spine (AS) and the tibial tuberosity (TT) as 2 distinct bony prominences, close to the upper end and lower end of femur, respectively, which are easy to locate and hence easy to measure. The length from AS to TT nearly corresponds to the femur length, and is referred to throughout the article.
We have done this study as a pilot project, which helps us in formulating an easier, accurate, and faster OG tube insertion process. Based on the results and statistically generated equations, a wider study is in process covering a larger sample size, thus authenticating our pilot project. This study was undertaken to derive the existence of any correlation between AS-TT and OG tube length.
Objectives
To find out a formula to predict OG tube length in terms of femur length of neonates and its agreement levels to the existing standards.
Materials and Methods
The study is basically an observational study and consisted of 3 parts. The first part was done over a period of 3 months (November to January 2016) on 53 newborns admitted to the newborn intensive care unit of the tertiary care center. Comparison of NEMU method of OG tube length was done with AS-TT so as to find out the relation between these 2 key variables along with other covariates at hand. Every consecutive baby who required OG tube insertion as an intervention was included in this study. Calculation of gestational age was done based on the mother’s history followed by a correction based on the New Ballard score. 18 Dysmorphic, preterm, and intrauterine growth retardation newborns, newborns having congenital anomalies, congenital dislocation of hip, very sick neonates, and newborns whose gestational age at birth mismatched with New Ballard score were excluded from the study.
OG tube insertion was done using the NEMU method, which is a standard practice in our setup. After OG tube insertion, the position of the OG tube was confirmed clinically (gastric contents aspiration or pushing air and carefully auscultating for gurgling sound over the epigastric region or thoroughly examining the visual characteristics of aspirate). 1 If the aforementioned criteria were not met the tube position was adjusted till clinical confirmation. Radiological confirmation was not done, as it has been associated with radiation hazards, and also has ethical issues with children admitted to this setup. After optimal placement, the marking of the tube at the lip was rounded off to the nearest centimeter.
The length from the AS to the TT was then measured in these cases using a nonstretchable tape. All subjects were assessed by a single observer to avoid bias. Data were entered in a master sheet prepared in Microsoft Excel (Version 2007) and analyzed using Stata Version 12.0 SE licensed to the corresponding author. Relation between the length of OG tube by NEMU with that of AS-TT was done using correlation analysis and scatter plots. Agreement levels of these methods was also plotted using Bland Altman analysis. Average time taken by the researcher to conduct the process using AS-TT was also recorded for all the cases. Simple linear regression analysis was done to model for OG tube length as a dependent variable with AS-TT as the independent variable was also calculated using regression analysis. Sensitivity analysis was also done by placing other covariates in the model and then deciding their role in the model as per practical needs. Agreement levels for the 2 methods was assessed using Bland Altman’s analysis and Pittman’s test of difference.19-21
The second part involved validating AS-TT as a predictor of OG tube length using the regression model (generated in the first part). OG tube insertion was done till the length calculated using the new equation (using AS-TT length) over a set of 10 other newborn babies admitted to the NICU with due consent from parents. Those senior pediatricians of the department who were not involved in the study assessed the presence of the lower end of the OG tube inside the stomach. This was done to avoid bias. All the cases of measurement by the AS-TT method and insertion was done by the one of the researchers.
The third part involved calculating time taken for inserting the OG tube using the NEMU and AS-TT methods by 10 medical personnel (nurses and resident doctors of pediatric department) and comparing them for any significant difference. To avoid bias, the cases were randomly allotted using lottery method. The time was calculated from the point of first contact with the newborn till the member called out the measured distance aloud, which was rounded off to the nearest whole number in seconds. The insertion of feeding tube followed later on. Time taken was recorded using a stopwatch in 10 different stable newborn cases.
Ethical concerns were sorted out before the study was initiated. Ethical clearance was obtained from the institute’s ethics committee. Informed consent was taken from the parents of the baby who needed OG tube insertion for participation in the study. Radiography was avoided for confirmation of tip of OG tube inside the stomach looking at the side effects of radiation exposure early in life and risk involved in mobilizing the child out of the NICU without any emergency requirement.
Results
A total number of 66 cases were recruited for the study. Thirteen cases were excluded from the study, as they did not meet inclusion criteria. Out of the 53 newborns included in our study, 29 (54.71%) were females and 24 (45.29%) were males. The birth weight ranged from 2.25 to 3.4 kg, with an average birth weight of 2.81 kg (confidence interval [CI] 2.73-2.89 kg). The gestational age of the term infants in these cases had a mean of 262.5 days (CI 262-263 days). AS-TT varied from 9.5 to 13.5 cm, with a mean of 11.82 cm (CI 11.55-12.09 cm). The mean length of the OG tube needed in such cases was 20.51 cm (CI 20.24-20. 77). Details are given in Table 1.
Summary Statistics of the Newborn Cases Admitted in the NICU.

Abbreviations: NICU, neonatal intensive care unit; BW, body weight; OGT, orogastric tube; AS-TT, anterior superior iliac spine to tibial tuberosity length; GA, gestational age.
Scatter plot between OGT length and AS-TT demonstrated almost a linear correlation (Figure 1). Correlation analysis was done between OGT length as the dependent variable with birth weight, gestational age in days, and AS-TT (Table 2). It was observed that there is a strong positive correlation between OGT and AS-TT, with a correlation coefficient r of .88. Correlation was also high between OGT and birth weight (r = .72). The relation between gender and OG tube length derived as per AS-TT was not found to be statistically significant.

Scatter plot (along with 95% confidence limits) of OGT length and AS-TT.
Bivariate Analysis (Correlation) of Femur length (AS-TT) With OG Tube Length (NEMU) and Other Covariates.
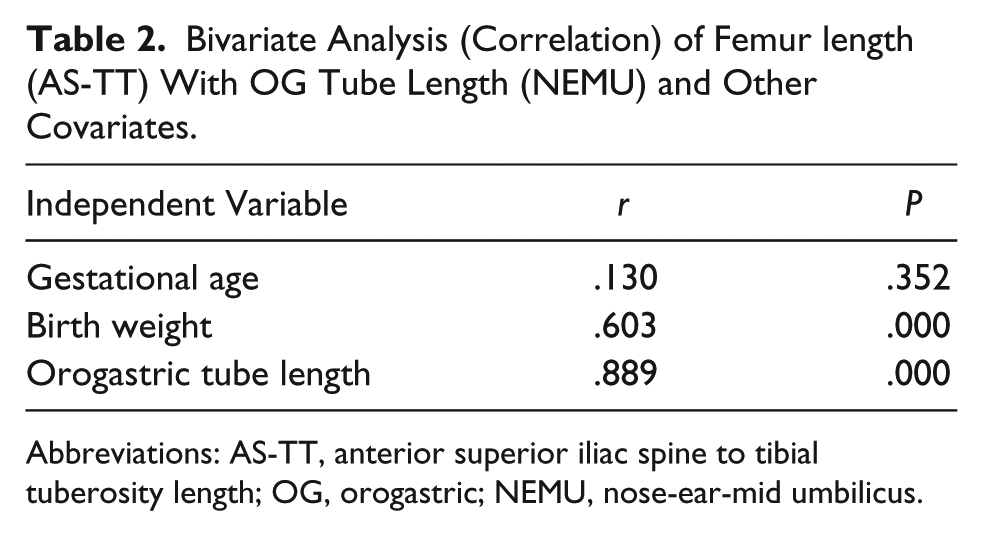
Abbreviations: AS-TT, anterior superior iliac spine to tibial tuberosity length; OG, orogastric; NEMU, nose-ear-mid umbilicus.
Further regression analysis was done on these factors (Table 3 and 4) so as to remove the effects of other variables. It was seen that a linear regression equation could explain the relation of OG tube length with that of AS-TT. It can be written as follows:
Linear Regression of OGT With Femur Length (AS-TT) (N = 53).

Abbreviations: OGT, orogastric tube; AS-TT, anterior superior iliac spine to tibial tuberosity length; Coeff., coefficient of regression; SE, standard error; CI, confidence interval; FL, femur length.
Linear Regression of OGT With Femur Length (AS-TT) and Birth Weight (n = 53).

Abbreviations: OGT, orogastric tube; AS-TT, anterior superior iliac spine to tibial tuberosity length; Coeff., coefficient of regression; SE, standard error; P, probability; CI, confidence interval; BW, body weight; FL, femur length.

Furthermore, a sensitivity analysis was done by adding birth weight into the equation, which showed that this equation was also able to explain the relation:

Bland Altman analysis of FL and OGT (measured by NEMU) showed that the limits of agreement (reference range for difference) was 7.764 to 9.613 (on the same side, which means these are statistically significant) while the mean difference was 8.689 (CI 8.561-8.816; Figure 2). Pitman’s test of difference in variance was r = .028, n = 53, and it was not found to be statistically significant (P = .840), showing that the variances of both the measurements were similar.

Bland Altman plot of femur length (AS-TT) with orogastric tube length.
The average time taken by the physician and nurses to measure AS-TT was 10.6 seconds, while for NEMU it was 12.3 seconds, which was found to be a clinically significant time difference. But if the researcher did AS-TT measurement procedure (which would mean that if AS-TT was done by an experienced person), the actual time taken to measure AS-TT was around 7 to 8 seconds, and for NEMU 11 to 12 seconds. However, for nurses it was a bit longer.
Discussion
Currently, prediction of OG tube placement length is based on normograms that are dependent on weight, ARHB, NEMU, and NEX. The NEX measurement is done by stretching the tube to be inserted first from the tip of the nose to the bottom of the earlobe and then to the xiphoid process. The NEMU measurement is done by stretching the tube to be inserted first from the tip of the nose to the bottom of the earlobe and then to the observed midpoint between the xiphoid process and the umbilicus. 1
In 1978, Ziemer and Carroll 22 reported that an NG tube that was inserted using the NEX method reached just below the gastroesophageal sphincter, whereas majority of the tubes were positioned appropriately when inserted as per the NEMU method.
In 1987, Weibley and colleagues 23 carried out a prospective study where the NEMU insertion length predictor was used on 30 premature infants with gestational age ranging between 28 and 36 weeks. Prospectively, on radiological confirmation, it was deduced that the NEMU distance fell short in 39.3% of the infants.
In 2004, Tedeschi et al 24 applied the NEMU method to place 43 NG/OG tubes in 38 premature infants with gestational age ranging between 25 and 35 weeks. Two (4.6%) tubes were not placed appropriately in the stomach.
The above-mentioned studies used the universally accepted NEMU method to predict NG/OG tube length. The errors might have been due to inaccuracy while adding up 2 consecutive measurements. Also, the dimensions would vary if the head were not maintained passively in neutral position by the observer while taking the measurements.
In 2007, Beckstrand et al. 25 studied 20 external measurements (including NEX, NEMU, age of the patient, anthropometric parameters like weight and height/length) to assess their role as possible insertion length predictors in 494 children aged between 2 weeks and 19 years of age. Regression equations that were generated using height in age groups (ARHB) were found to be the most reliable method for estimating NG/OG tube length. In spite of using their suggested equations, 3.4% of NG/OG tubes were not placed appropriately in the stomach.10,14
Taking the entire length (height) of the baby is a cumbersome process and requires manual efforts for extending the lower limbs in an active baby and more accurately the use of an infantometer. The nonavailability of an infantometer at peripheral setups, the use of an assistant to stabilize the active neonate and the risk of transmitting infections during the process make the necessity of an easier and safer method the need of hour.
Freeman et al 12 performed a prospective study on infants weighing 397 to 4131 g. Formulas were derived to predict tube insertion length in centimeters: OG tube = [3 × weight + 12]. The formula correctly predicted 60% of misplaced OG tubes. 12 Weight may be easily and accurately taken. However, in sick unstable newborns, in peripheral health care setups, during the resuscitation procedure, if the baby has too many intravenous lines attached to him or her, and if the newborn is dependent on ventilator or any other machine, weighing the baby may not be possible. In all these conditions, AS-TT may prove to be a better option as it does not interfere with the ongoing treatment or resuscitation.
Our study shows that there is a positive correlation between the optimum OG tube length and AS-TT in newborns. Among the 29 females and 24 males included in the study, the length of the OG tube inserted was found to be independent of the sex of the baby. No previous studies have succeeded in establishing a relationship between the OG tube length and the neonate’s gender.
In this study, correlation was high between OG tube length and birth weight (r = .72). A relationship between these 2 parameters was established in a prospective study undertaken by Freeman and colleagues. 12 The significant relationships of OG tube length with respect to AS-TT and birth weight generated in our study led to the formulation of Equation (2).
There are various occasions where measuring weight of the neonate may be difficult in the NICU. Some patients might get edema and some may lose weight in the NICU. Considering it was a variable factor, the measurements too can vary. Also, it will not be easy to record weight accurately in critical patients on ventilator. So including weight in the equation using AS-TT may rather delay the OG tube insertion process in case of any emergency intervention needed. Hence, sticking to the equation based solely on the AS-TT (without considering birth weight) can be a better one, as assumed by the researchers. Considering the stomach capacity of neonates to be around 20 mL, 26 the standard error as per Equation (1) is quite acceptable.
Nurses and physicians who carried out the AS-TT and NEMU measurement exercise were trained in NEMU measurement while untrained/unskilled personnel measured AS-TT. This was because the routine procedure they used for OG tube insertion was NEMU. Thus, they took a longer time than the researcher. The nurses in fact took comparatively more time compared to physicians or researchers as they were new to the AS-TT technique and took more time locating the bony prominences as knowledge of human anatomy was lacking and palpating skills were poor. Medical professionals did not face much problem with it.
Conclusion
All previously known methods for estimating OG tube lengths like NEX, NEMU, and weight- or height-based methods have their respective errors and associated risks. In the presence of these fallacies, a newer, safer, and universally accepted anthropometric parameter like “anterior superior iliac spine (AS) to the tibial tuberosity (TT) length,” closely related to femur length, can be chosen as a guide to estimate OG tube length, since it has good levels of agreement with standard methods like NEMU with maximum accuracy.
Limitations of the Study
The small sample size and exclusion of preterm babies is a disadvantage of the study, which leads to right sided skewing of the data. Further studies are in process where we are including preterm neonates to find out if this equation is validated in them. Confirmation of OG tube position through the gold standard technique, that is, radiographs, has not been done.
Future Direction
We are presently evaluating the regression equations covering a larger sample size where comparison of both the above-mentioned equations and testing their credibility with respect to the speed and accuracy of positioning would be possible. The formula that we derived in our study may further be validated by a well-designed randomized controlled trial before it can be widely used.
Author Contributions
S Mahapatro: Contributed to conception; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
S Mohanty: Contributed to acquisition and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SKP: Contributed to design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RKR: Contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SS: Contributed to acquisition; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.