
Abstract
The need for neonatal advanced resuscitation can differ by location and region, and there is limited information on the factors that affect this need. The research focused on assessing the rate of advanced resuscitation for newborns in northern Iran and identifying associated factors. This retrospective cross-sectional study investigated the newborn resuscitation steps in different departments of a maternity hospital over a 5-year period. Data on advanced resuscitation rates were analyzed. The study included 9247 live births, with 586 resuscitations analyzed. Among the resuscitated newborns, 358 (61.09%) required advanced resuscitation, representing 1.2% of all live births. The need for advanced resuscitation was significantly higher in NICU admissions (83.2%) compared to delivery room resuscitations (38.4%). The success rate was also higher for delivery room advanced resuscitations. Location, prematurity, and staff experience affect advanced resuscitation needs, underscoring the need for enhanced neonatal resuscitation services in low and middle-income regions.
Introduction
Transition from intrauterine life to extra-uterine life is a big physiological challenge for newborns at birth, with dramatic changes in the cardiovascular and respiratory systems.1 -3 While most of the newborns would have started breathing within the first 30 seconds of life or after drying and stimulation, some need more or less support to successfully transition to extra-uterine life.1,4 Every year, nearly 1 million children are born with hypoxic-ischemic conditions and survive with possible complications like cerebral palsy, disability, and learning difficulties; it is therefore proven that providing proper resuscitation at birth would help reduce the mortality and morbidity rates.5,6 Approximately 10% of newborns need some type of resuscitation immediately after birth. This usually involves initial steps of resuscitation or positive pressure ventilation. However, the need for more advanced interventions, such as intubation, chest compressions, and giving medications, is rare and cannot be predicted before delivery.7,8 The shortage of skilled individuals in delivery rooms for advanced resuscitation may present challenges, as these interventions demand experienced personnel and effective teamwork .9,10
Research confirms that although a small percentage of newborns, ranging from 0.1% to 0.3%, require advanced cardiac resuscitation immediately after birth, the need for resuscitation interventions and procedures varies among different regions and countries. 11 There exist differences in resuscitation needs among developed, developing, and underdeveloped countries. This difference may exist because intrapartum risk factors are more common, and prenatal care is less accessible in low resources-settings .lower to moderate-income countries have high rates of perinatal mortality and morbidity resulting from a lack of access to quality healthcare services.1,4 Quality of healthcare provision has been identified as one of the major factors not only in low-income countries but also in high-income nations so far as neonatal mortality and morbidity rates are concerned. Indeed, research on neonatal resuscitation and advancements in related programs has a critical role in reducing neonatal mortality rates. 12 The need for advanced neonatal resuscitation procedures differs between NICU (neonatal intensive care unit) and delivery rooms. The level of resuscitation required for newborns is influenced by issues such as the environment of resuscitation and improvement in technology, which play a crucial role in improving outcomes . 13
There is limited information in the scientific literature on factors associated with the need for neonatal advanced resuscitation interventions. 14 Hospital resources and capacities vary globally, and findings from one region cannot be extrapolated globally to another region.15,16 Therefore, resuscitation programs should be adjusted according to the unique conditions of the resuscitation environment. All these differences have to be understood so that appropriate planning and provision for newborn resuscitation can be done in different settings by health providers.
Iran has a national neonatal resuscitation program based on NRP (Neonatal Resuscitation Program) and HBB (Helping Babies Breathe) principles. It provides structured training that covers the initial steps, positive pressure ventilation, and post-resuscitation care, including surfactant and caffeine therapy, for healthcare workers. 17 Studies show its effectiveness within the Iranian system. In Iran, the Neonatal Resuscitation Program (NRP) is managed by the Ministry of Health. It is communicated through medical universities and training units in hospitals. Training happens as both preservice courses for medical, nursing, and midwifery students and in-service courses for practicing staff. Certification lasts for 2 years, and staff must complete refresher training afterward. All specialists, nurses, and midwives in hospital’s neonatal resuscitation team are certified, having completed the neonatal resuscitation course.18,19 While understanding these factors is important to prepare the team and ensure appropriate care for preterm births that are common in tertiary care centers, there is a lack of information regarding neonatal resuscitation in Iran. 20 This study was performed to determine the rate of advanced resuscitation of newborns and its related factors in various wards of a maternity hospital in northern Iran.
Materials and Methods
This retrospective cross-sectional descriptive study was conducted at Imam Khomeini Hospital in Sari Northern Iran, and affiliated with Mazandaran University of Medical Sciences. The study investigated all neonatal resuscitation records performed in the delivery room or NICU from April 2019 to December 2023.
The hospital is an obstetric tertiary academic referral center for high-risk pregnancies, with the capacity to handle approximately 2000 deliveries per year. The whole setup has a gynecological and obstetric care department with facilities for normal vaginal delivery and cesarean sections, a neonatal department with 12-bed NICU. Each ward boasts of one main resuscitation crib and one standby crib; a mobile resuscitation crib is also available in case multiple births or very preterm deliveries occur.
The core resuscitation team typically consists of a midwife, a nurse assistant, and a pediatric resident. In critical situations such as premature birth, suspected asphyxia at birth, and high-risk scenarios a consultant neonatologist is called up. A full resuscitation team includes a consultant neonatologist if not already present, a neonatal nurse, and an anesthesiologist may also be called to provide comprehensive support. At least one trained midwife and one pediatric resident are at every delivery. For high-risk deliveries (eg, preterm labor <34 weeks, multiple gestation, meconium-stained amniotic fluid, fetal distress, or maternal complications such as preeclampsia), a neonatologist and an anesthesiologist are also there. In routine low-risk deliveries, a neonatologist may not be present, but is available right away if needed.
All staff are trained regularly and periodically trained in neonatal resuscitation, and the resuscitation procedures follow the updated guidelines established by the American Academy of Pediatrics for newborn resuscitation, following the International Liaison Committee on Resuscitation (ILCOR) and latest version of NRP.21 -23 Endotracheal intubation is done only by a neonatologist, pediatric resident, or anesthesiologist on the team. The neonatal unit is equipped to support both basic and advanced resuscitation procedures. Basic equipment includes bag-mask devices, suction apparatus, and radiant warmers, which are routinely available in delivery rooms. Advanced resuscitation tools include Laryngeal Mask Airways (LMA), endotracheal tubes (ET), laryngoscopes (Continious Positive Airway Pressure) CPAP systems, and mechanical ventilators. These resources are accessible in both the delivery room and the NICU, enabling timely escalation of care in accordance with NRP guidelines.
The study involved newborns requiring resuscitation at birth or upon admission to the NICU, and their information was recorded on relevant forms throughout the study period. Neonates without ethical indications for resuscitation, such as those with a gestational age below 22 weeks, birth weight under 400 g, life-threatening congenital anomalies, and, encephalopathy were excluded. Forms with incomplete data were excluded from the analysis.
Resuscitation follows the NRP algorithm, 23 beginning when a newborn shows poor tone or fails to breathe spontaneously. Positive Pressure Ventilation (PPV) is initiated if the heart rate is below 100 beats per minute or if the baby is apneic or gasping. If the heart rate remains below 60 bpm after 30 seconds of effective PPV with visible chest rise, advanced resuscitation begins. Chest compressions are started, ideally with an advanced airway in place. drugs are administered if bradycardia persists after 60 seconds of coordinated compressions and ventilation. Oxygen is titrated based on pulse oximetry, with room air used initially and supplemental oxygen added only if saturation targets are not met.
A standard newborn resuscitation form prepared by the Ministry of Health of Iran is included in the file of all newborns and is filled in for resuscitated neonates.
Individual maternal and neonatal characteristics such as gestational age, multiple pregnancies, amniotic fluid status, type of delivery, presence of maternal or fetal underlying diseases, and neonate gender were extracted and documented. Gestational age was determined using the reported date of the last menstrual period or prenatal ultrasound. Maternal and fetal diseases were recorded from prenatal consultations that were documented in the resuscitation sheet.
In this study, detailed actions beyond the initial steps of resuscitation for each baby were documented, including oxygen supply, positive pressure ventilation, intubation, cardiac massage, and drug administration. Additionally, the time and location of resuscitation were noted. In this study, we defined basic resuscitation as including initial steps and bag-mask ventilation (BMV), and advanced resuscitation as involving intubation, chest compressions, and giving drugs alongside and simultaneous with positive-pressure ventilation, based on the latest version of NRP. 23 Apgar scores were recorded at 1 and 5 minutes with the final result was recorded for each neonate. Resuscitation conducted during transfer between wards for the same newborn was considered as a single entry to avoid duplicate data. The outcome, whether stabilization or newborn death, was recorded post-resuscitation.
The rate of advanced resuscitation required at birth was determined relative to the total number of live births. The percentage of newborns necessitating advanced resuscitation was calculated separately for the NICU and the delivery room, allowing for a comparison between the 2 settings. Furthermore, an assessment was conducted to evaluate the association of risk factors with the requirement for advanced resuscitation.
In the context of the study mentioned, advanced resuscitation measures for newborns include intubation, cardiac massage, and administration of medications.
Sample Size
Based on the probability of a 5% type 1 error (α) and a test power of 90%, and considering the need for advanced resuscitation as indicated for the previous study, 20 the minimum sample size required was determined to be 506 cases.
Statistical Analysis
All analyses were performed using SPSS version 26 software. Descriptive statistics including mean ± standard deviation for quantitative variables and frequency (percentage) for categorical variables were used for data analysis. Statistical comparisons were performed using the chi-square test or Fisher’s exact test for categorical variables and Mann-Whitney U test for continuous variables. In addition, a logistic regression model was used to evaluate the relationship between risk factors and the need for advanced resuscitation. A P-value of less than .05 was considered significant for all comparisons.
Ethical Considerations
Data extraction was conducted confidentially from neonatal resuscitation sheets, and all neonatal interventions adhered to the latest guidelines for resuscitation. Consent was waived for the study given that enrollments were already completed and based on the population. The study was approved by the research ethics committee of Mazandaran University of Medical Sciences (IR.MAZUMS.REC.1401.17327).
Results
During the study period, there were 9247 live births in the hospital, with 603 newborns requiring postnatal resuscitation. After excluding 17 cases, a total of 586 resuscitation cases were analyzed. The number of newborns meeting the inclusion criteria across the study period was distributed as follows: 137 cases in 2019, 76 in 2020, 75 in 2021, 166 in 2022, and 132 in 2023. Among these cases, 339 (57.8%) were male and 421 (71.8%) were delivered by cesarean section. 81.1% of cases were extremely or very preterm. Prenatally, 26.1% of the newborns were diagnosed with Intra Uterine Growth Restriction (IUGR), while the remaining 73.9% were not (Table 1). Of the 9247 live births during the study period, 586 newborns (6.34%) required basic resuscitation. All resuscitation episodes began with basic interventions, and 358 of these cases subsequently required escalation to advanced resuscitation measures, corresponding to 3.87% or 38.7 per 1000 live births. The medical record registration process is illustrated in Figure 1.
Distribution of Gestational Age and IUGR Status Among Resuscitated Newborns.
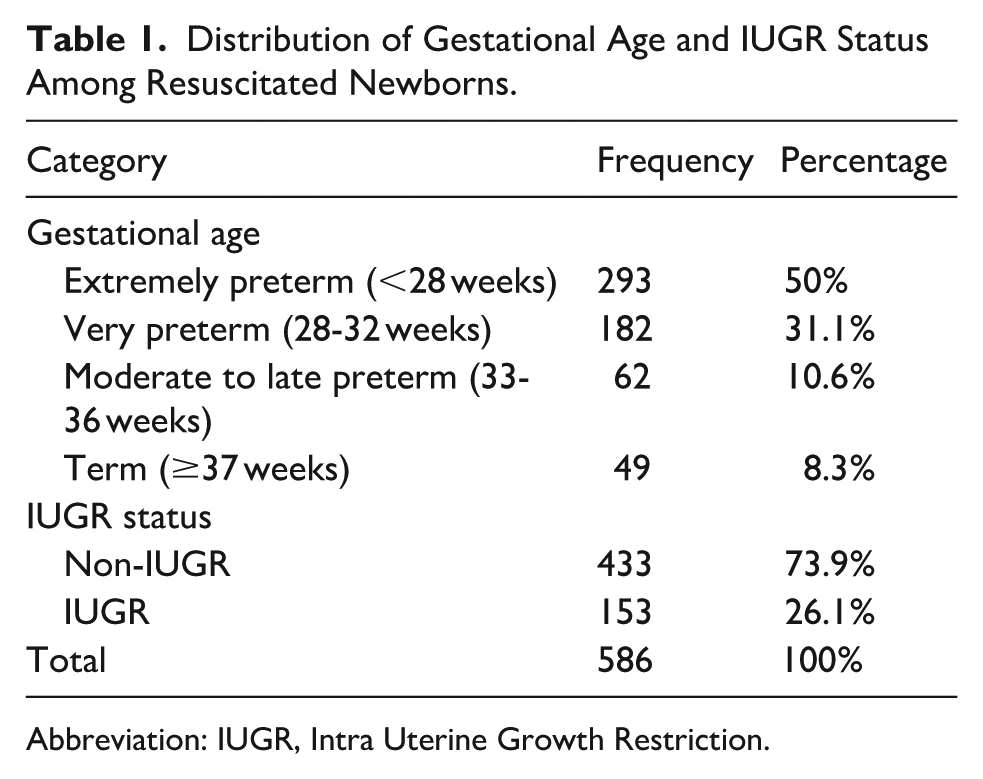
Abbreviation: IUGR, Intra Uterine Growth Restriction.

Flow chart of the study population.
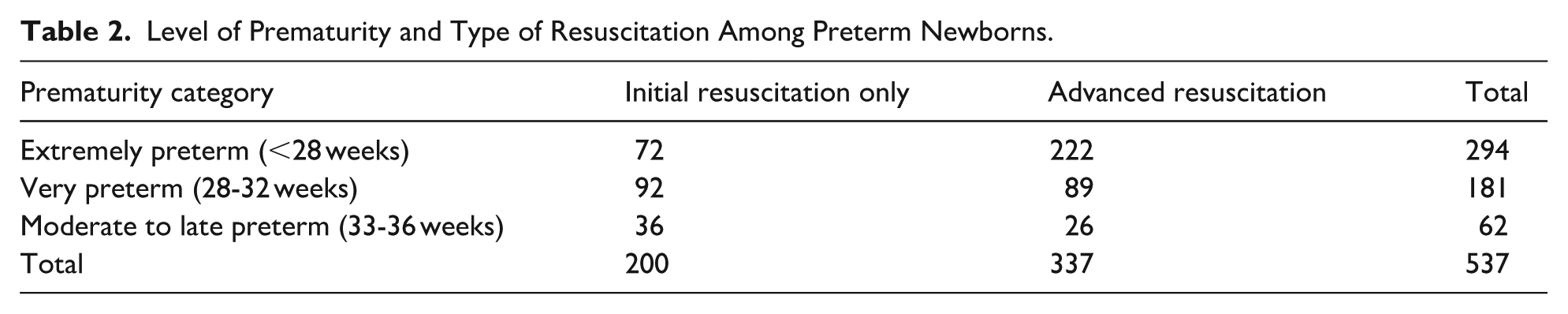
Extremely preterm infants represented the largest proportion of advanced resuscitation cases, accounting for 222 out of 337 preterm newborns who received advanced interventions. In contrast, very preterm and moderate to late preterm infants comprised 89 and 26 cases, respectively (Table 2). The mean gestational age of neonates who received resuscitation in the delivery room was 29.9 ± 4.5 weeks, while in the NICU, it was 27.4 ± 3.8 weeks. In addition to this, the average Apgar score of neonates resuscitated in the delivery room was 4.35 ± 2.18 at 1 minute and 6.59 ± 2.44 at 5 minutes, with a median of 5 and 7, respectively.
Level of Prematurity and Type of Resuscitation Among Preterm Newborns.
The requirement for advanced resuscitation among newborns resuscitated in the delivery room was 111 cases, representing 1.2% of all live births. This rate varied across the study period, ranging from 0.8% to 1.86% annually.
The requirement for advanced resuscitation was significantly higher in newborns hospitalized in the NICU compared to newborns resuscitated in the delivery room (P < .001). Table 3 shows and compares the proportion of newborns requiring various steps of resuscitation and advanced resuscitation to the total number of newborns requiring resuscitation after birth in 2 distinct settings: the NICU and the delivery room.
Newborn Resuscitation Needs to Different Steps Compared to Total Resuscitated Neonates.
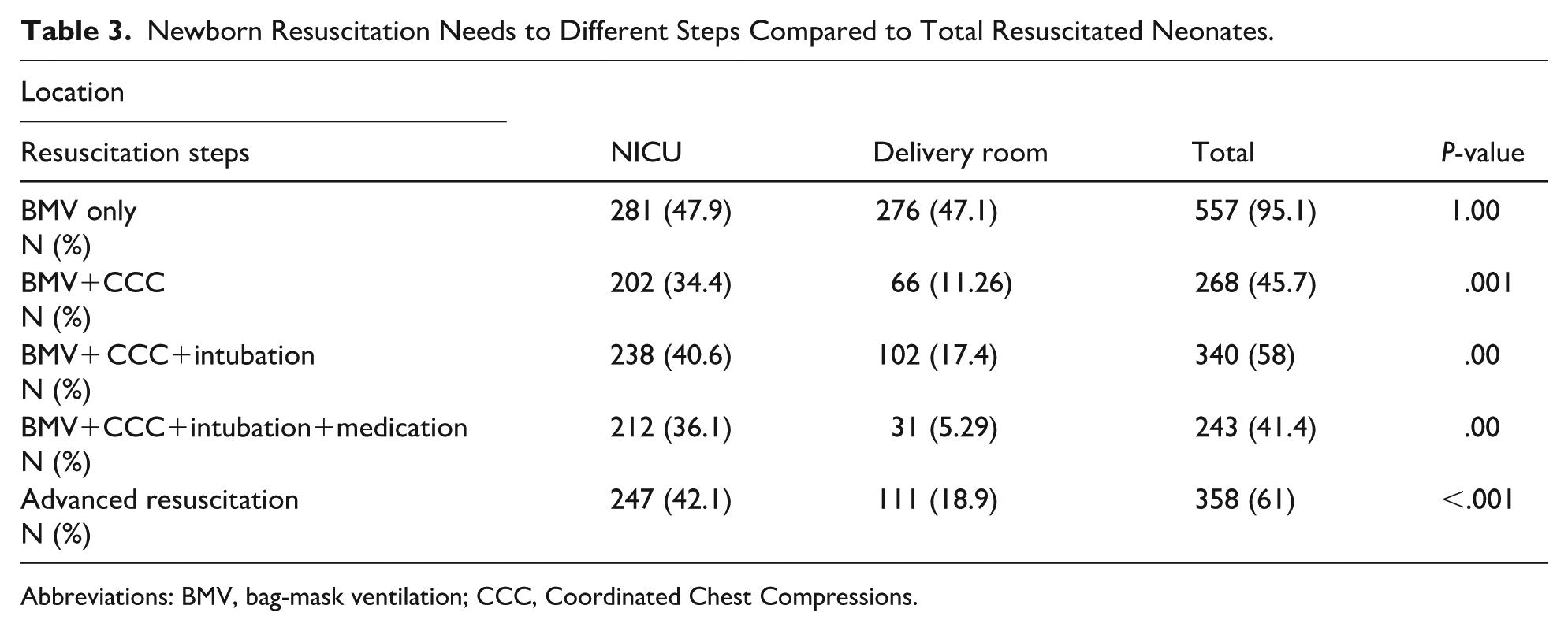
Abbreviations: BMV, bag-mask ventilation; CCC, Coordinated Chest Compressions.
Among the 297 neonates resuscitated in the NICU, 247 (83.2%) underwent advanced resuscitation. In comparison, out of the 289 babies resuscitated in the delivery room, 111 (38.4%) received advanced resuscitation, showing a statistically significant difference (P = .00).
Among the 586 newborns who underwent resuscitation, bag-mask ventilation was performed in 557 cases (95.1%), and intubation was documented in 340 cases (58%). Of these, 358 infants (61.1%) required advanced resuscitation, defined as the use of intubation, chest compressions, or medication administration. Within this group, cardiac massage was recorded in 266 cases (74.3%), intubation in 339 cases (94.7%), and drug administration in 242 cases (67.6%). Free-flow oxygen was administered in 302 cases (51.5%) as an adjunctive measure.
Resuscitation success was documented in 439 of the 586 cases (74.9%). All cases requiring only basic resuscitation were successfully stabilized. Among newborns who received advanced resuscitation, 211 cases (58.9%) were successfully stabilized, representing 36% of all resuscitated neonates.
Of the newborns admitted to the NICU, 163 (54.8%) were successfully resuscitated, while 276 (95.5%) of the newborns resuscitated in the delivery room were successfully resuscitated. The comparison between the 2 groups showed that the resuscitation success rate was significantly higher in the delivery room (P < .001).
Analysis of risk factors associated with advanced resuscitation rate, using logistic regression, identified prematurity, leadership by someone other than a neonatal consultant, resuscitation in the NICU, multiple births, and fetal issues as risk factors in this scenario (Table 4).
Risk Factors for the Need for Advanced Resuscitation Steps in Newborns.

Discussion
Over a 5-year-period in a tertiary care hospital, our study found that the need for advanced resuscitation accounted for approximately 1.2% of all live births. The need for advanced resuscitation was significantly higher in the NICU compared to the delivery room. Factors influencing the need for advanced resuscitation include prematurity, multiple births, resuscitation led by a non-neonatologist, and fetal complications. Our results underscore the common concern for advanced resuscitation in our resource-limited maternity hospital, with approximately 61% of resuscitated neonates requiring advanced stages.
Although the rate of advanced resuscitation in the delivery room was not very high compared to the total number of live births in our hospital, it is higher compared to many other studies conducted in regions with more resources. A study in Norway reported that the need for advanced resuscitation in their center was rare and short-term neonatal outcomes were favorable. 24 This low incidence is likely attributable to the presence of highly trained personnel, standardized delivery room protocols, and robust antenatal care systems. In a study in the Republic of Korea, a significant reduction in the trend of intubation during neonatal resuscitation was observed with improved delivery room care. A reduction in the trend of advanced resuscitation was associated with a reduction in neonatal mortality and morbidity. 25 These findings suggest that systemic improvements in perinatal care can directly influence the need for advanced interventions. A study in Thailand showed that approximately 3% of newborns required resuscitation with 0.2% of cases necessitating advanced resuscitation. Mortality was significantly higher in newborns requiring advanced resuscitation. 26
Compared to these contexts, our higher rate of advanced resuscitation may reflect underlying disparities in prenatal risk profiles, resource availability, and the timing of clinical decision-making. It also highlights the importance of strengthening delivery room preparedness and investing in scalable, context-sensitive resuscitation strategies tailored to the realities of low- and middle-income setting.
However, some studies have shown a higher requirement for advanced resuscitation compared to our study. For instance, in Italy, 2% of newborns, and in Tanzania, 6% of newborns required advanced resuscitation, which is higher than our findings.27,28 The Italian data, drawn from tertiary centers with widespread access to neonatal equipment, suggest that higher intervention rates may reflect proactive escalation protocols rather than increased neonatal risk. In contrast, the Tanzanian figures likely stem from systemic limitations in antenatal care and delayed recognition of perinatal distress, necessitating more frequent advanced interventions. A study from South Africa focusing on resuscitation in very low birth weight neonates indicated that 10.6% of these babies needed advanced resuscitation, contributing to the higher mortality rate in this group. 29 These elevated rates underscores the vulnerability of extremely preterm neonates and highlights the critical importance of early identification and skilled resuscitation in high-risk deliveries. Limited research on neonatal resuscitation has been conducted by researchers in Iran. One Iranian facility reported an approximate 1.15% rate of advanced resuscitation requirement in a study similar to ours, while another study documented a 3.9% prevalence, surpassing the rates observed in our study.20,30 Additionally, a study specifically on preterm infants revealed that around 5% of babies required advanced resuscitation. 31
Furthermore, various health centers may implement variations in resuscitation strategies. In a retrospective study conducted in China by the Chinese Neonatal Network 2019 involving very preterm neonates, nearly 50% of these neonates either required advanced resuscitation steps or exhibited an increasing trend in interventions in the delivery room, which was associated with higher mortality rates. the study’s findings highlighted the diverse resuscitation approaches across different centers and underscored the importance of standardizing resuscitation protocols. 32 It is evident that mortality rates are elevated in resource-limited settings when advanced resuscitation is necessary. 15
In our study, factors such as prematurity, multiple births, absence of a neonatologist as the resuscitation team leader, and fetal problems were found to be associated with an increased requirement for advanced resuscitation. A large multicenter prospective study conducted across several countries identified late prematurity, underlying maternal diseases, general anesthesia, instrumental delivery, obstetric complications, and fetal bradycardia as risk factors for advanced resuscitation. However, in our study, obstetric complications and underlying maternal diseases did not demonstrate a significant impact. 14 The type of delivery did not affect the need for advanced resuscitation in our study. Conversely, a study that contradicts our findings, reported that the type of delivery did influence the need for advanced resuscitation. 20
Although the need for advanced resuscitation steps in neonates is still reported to be rare, particularly in the delivery room, documentation of events related to resuscitation has often been inaccurate or incomplete leading to gaps in articles related to neonatal resuscitation. 8 While most technological advancements and monitoring improvements in the delivery room have enhanced resuscitation at birth, providing better care, and improved outcomes, the delivery room remains a specific setting with significant challenges. Advances in equipment, such as the availability of more advanced facilities like respiratory function monitors, video laryngoscopy, electrical impedance tomography, artificial intelligence, video recording, augmented reality, and non-contact monitoring, may prove beneficial in future resuscitation efforts in the delivery room . 13
Meanwhile, the need for advanced resuscitation measures may vary across different conditions and locations. Depending on local circumstances and resource constraints, the implementation of neonatal resuscitation protocols may differ. Our study revealed a significant disparity in the utilization of advanced resuscitation techniques between the NICU and the delivery room. A recent study indicated that approximately 0.25% to 3% of neonates admitted to the NICU required cardiopulmonary resuscitation. Consistent with our findings, the resuscitation rate was 10 times higher in the NICU compared to the delivery room. 33 A recent study conducted at our facility demonstrated a rising trend in preterm births and NICU admissions in recent years compared to pre-COVID-19 times. This observation may support the justification for employing advanced resuscitation methods at our facility. 34 Therefore, it is crucial to optimize the care of hospitalized neonates based on their individualized resuscitation requirements.
Our study demonstrated that the lack of a neonatologist leading the resuscitation process led to a higher demand for advanced resuscitation techniques. This underscores the significance of having trained personnel present to avoid inappropriate or excessive interventions. Previous research has indicated that hospitals engaged in neonatal resuscitation should prioritize elements like advanced equipment, proficient providers, and efficient team collaboration. 35
The primary strength of our study lies in examining the need for advanced resuscitation across various settings. By identifying risk factors associated with newborns and deliveries that may necessitate advanced resuscitation, we can enhance readiness for such situations. This study has the potential to assist hospitals in resource-constrained areas by improving staff readiness and resource distribution across diverse hospital settings.
Our study had several limitations. Firstly, it was retrospective and conducted at a single center. Secondly, being retrospective, the study may have been impacted by the COVID-19 pandemic, as a portion of the study period overlapped with the pandemic. The effects of the pandemic could have influenced the outcomes, and we were unable to eliminate potential confounding variables due to the study’s design.
Conclusion
Our results revealed a high demand for advanced resuscitation in the delivery room, particularly in the NICU, especially for preterm neonates and those with fetal issues. This emphasizes the importance of increased awareness and readiness in such scenarios, as well as the presence of skilled professionals during high-risk deliveries. Enhancement in the quality of neonatal resuscitation services is necessary in in low- and middle-income areas. It is recommended to conduct more prospective population-based studies on the need for advanced resuscitation.
Footnotes
Acknowledgements
The authors would like to thank Akram Valizadeh for her assistance in the data collection and the Clinical Research Development Unit (CRDU) of Boo Ali Sina Hospital, Mazandaran University of Medical Sciences for their support and cooperation throughout the study.
Ethical Considerations
Ethical approval was obtained for this report from the research ethics committee of Mazandaran University of Medical Sciences (IR.MAZUMS.REC.1401.17327).
Consent to Participate
Consent was waived for the study given that enrollments were already completed and based on the population.
Author Contributions
AHS, SAK, and RF are responsible for designing and conducting the study and they developed the first draft manuscript. AHS and SAK are responsible for data gathering. MM is responsible for data interpretation and analysis. All authors agreed on the final submitted version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted by a grant from (1401.17327) Mazandaran University of Medical Sciences as a medical student thesis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.