
Abstract
Keywords
Introduction
Global health (GH) electives are increasingly being offered during residency. Studies have demonstrated that such electives improve physical exam skills and increase knowledge of tropical medicine.1-8 Recent qualitative research analyzing reflective essays by pediatric GH track residents demonstrated that their learning mapped to the Accreditation Council for Graduate Medical Education (ACGME) competencies. 5
Despite these positive findings, medical educators have questioned GH electives’ value and impact,9-14 and they have called for improvements in GH education.2,3,15 Concerns are raised about lack of trainee preparation, consistency across training sites, and that GH electives may place undue burden on resource-strapped host institutions.9,14,16,17 Recent articles note resident stress during GH electives, and impact of culture shock and reentry.18,19 And little is known about longer term outcomes of GH electives. Some studies show participants are more likely to work with underserved communities, but there are minimal data about ongoing careers in GH.6,20,21
Currently, 58% of pediatric training programs offer international field experiences and 25% offer a formal GH track.22-25 The Boston Combined Residency Program has accessed multiple funding sources to which residents may apply for travel support. We report on a decade’s experience with GH electives.
Methods
In this mixed quantitative and qualitative retrospective study, we explored products (projects and skills developed), outcomes (effect on knowledge and attitudes), and career impact of pediatric residency GH electives. Our objectives were to:
Document GH elective products (projects or research completed and skill development)
Explore how participant factors relate to those products and outcomes, including participants’ knowledge, skills, awareness, and careers
Assess how characteristics of the elective experience affect elective products and careers
To facilitate our evaluation, we developed the logic model presented in Figure 1. 26
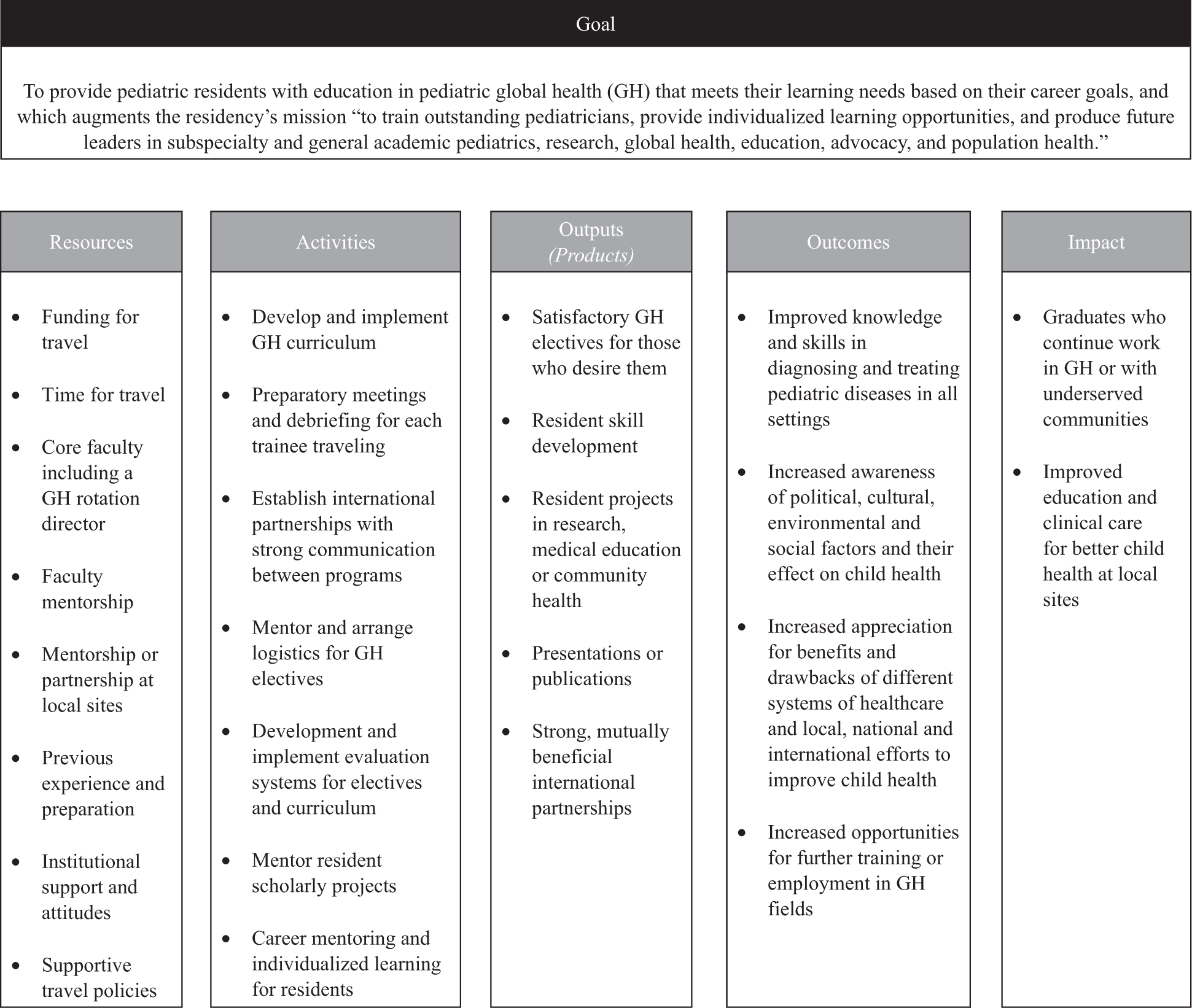
Logic model for global health education in residency.
Based on the logic model, we developed the study survey (see the appendix) to ask about participant and elective characteristics, elective products, self-perceived impact on knowledge and attitudes, along with magnitude of career impact. When possible, questions were modeled after similar studies. 27 Open field text questions asked how careers were affected, and descriptions of current work in GH or with the underserved. We refined the survey with input from members of the executive committee of the Association of Pediatric Program Directors Global Health Pediatric Education Group. In additions, 3 Boston Combined Residency faculty members who had done GH electives at other residencies piloted the survey and provided cognitive interviews and retrospective verbal probing.
All Boston Combined Residency alumni who received funding for a GH elective between 2002 and 2011 were eligible to participate. Using departmental databases, we identified 132 former residents who had used award funds for global travel, excluding the primary author. In March 2014, we emailed the 104 alumni for whom we had accurate email addresses, inviting them to participate in the online REDCap survey. 28 We sent 3 consecutive weekly requests to nonrespondents; we closed enrollment after 6 weeks.
For the quantitative sections of the survey, we used Stata Statistical Software (Release 13; StataCorp LP, College Station, TX) to assess associations between mitigating factors and means of the Likert-type responses for primary outcomes. We conducted χ2 and Fisher’s exact tests for categorical responses and t test for numerical responses. Alpha was set at .05 for all tests. We performed bivariate and multivariate logistic regressions to understand the relative impact of participant factors on outcomes.
For qualitative questions, results were analyzed using principles of open coding and thematic analysis to identify patterns in responses, facilitated by NVIVO software (Version 10; QSR International Pty Ltd, Doncaster, Victoria, Australia). Multiple coding and cross-checking optimized interrater reliability among the 2 coders who separately coded the interviews and met to compare and resolve any differences, and reconstructed and compared relationships among themes.
This study was approved by the Boston Children’s Hospital Institutional Review Board.
Results
We received complete responses from 69 individuals, representing 66% of those emailed and 52% of trainees funded for GH electives. Respondents described 94 GH electives undertaken from 2002 to 2011 in 28 countries.
Objective 1: Global Health Elective Products
The majority (40, 58%) of respondents reported their primary goal was to gain GH clinical experience, with the remainder working on community health projects (14, 20%), research projects (5, 7%), medical education projects (2, 3%), or other (8, 12%).
Table 1 shows elective products grouped as personal/professional skill development, educational projects, or scholarly products. A majority of participants reported improvement in clinical exam skills (48, 70%), with significant increases in mean number of personal skills developed for those who did multiple electives (0.93 outputs vs 2.96, P < .001). Fourteen residents (20%) reported scholarly products, with 11 (16%) presenting at national conferences and 7 (10%) publishing academic articles based on their GH elective work.
Global Health Elective Products.
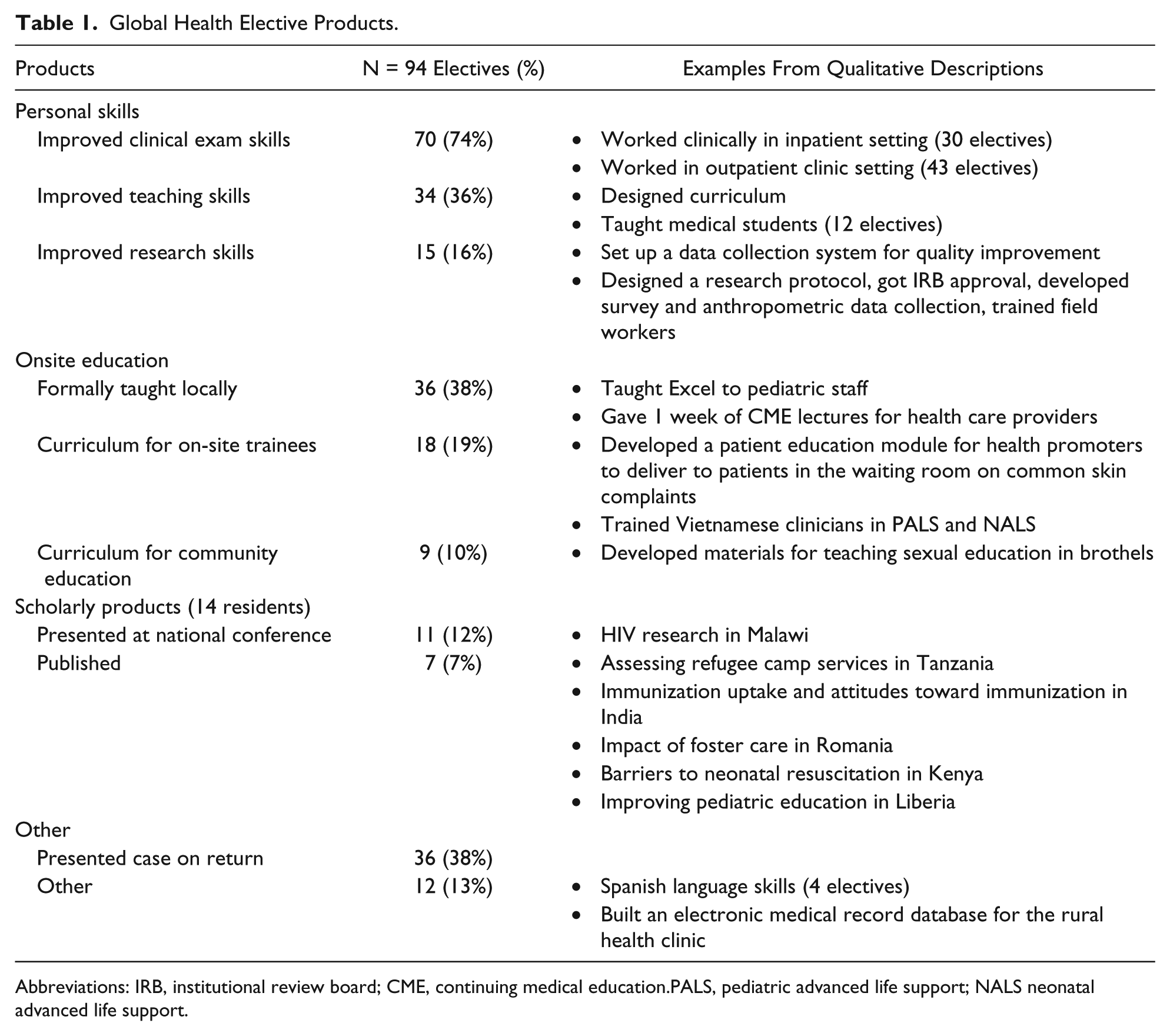
Abbreviations: IRB, institutional review board; CME, continuing medical education.PALS, pediatric advanced life support; NALS neonatal advanced life support.
Objective 2: Participant Factors
Forty-six residents (67%) had previous international field experience, with 13 (20%) reporting a year or more (Table 2). Nearly half of the residents with experience (21, 47%) did more than one GH elective compared with only 4 (20%) with no prior experience (P = .04). Fifty-four percent (25) of the experienced residents had onsite mentorship versus 5 (25%) without previous experience (P = .03).
Unadjusted and Adjusted Participant Factors in Global Health Electives During Pediatric Residency.

Abbreviations: AOR, adjusted odds ratio; CI, confidence interval; Ref., reference.
Overall model significance: P = .016; area under the curve: 0.73; Hosmer-Lemeshow χ2 = 1.17, P = .883.
Overall model significance: P = .304; area under the curve: 0.68; Hosmer-Lemeshow χ2 = 7.15, P = .128.
Overall model significance: P < .001; area under the curve: 0.87; Hosmer-Lemeshow χ2 = 1.47, P = .832.
Previous experience, number of GH electives, previous travel to the site, and cumulative elective time were not significantly associated with completing scholarly products, but were all strongly associated with postresidency work in GH or with the underserved. When controlling for previous experience, continuing a career in GH or with the underserved remained associated with spending more than 5 cumulative weeks on GH elective (adjusted odds ratio [AOR] = 9.4, 95% confidence interval [CI] = 1.6-55.2). When controlling for cumulative elective time, continuing a career in GH or with the underserved remained associated with greater previous experience: (0.5-5 months - AOR 7.3 (95% CI 1.7-31.2), >6 months – AOR 31.1 (95% CI 5.0-192.1).
Objective 3: Global Health Elective Factors
Residents were asked to describe their perceived impact of each GH elective as applied in their current work domestically or internationally. A majority of respondents rated each elective’s impact on their clinical knowledge and skill as mild (38, 40%) to moderate (38, 40%). Most reported a moderate (47, 51%) to large (29, 32%) impact on their awareness of social determinants of health, and almost all reported a moderate (46, 49%) to large (39, 42%) impact on their awareness of health systems.
Twenty-eight (30%) residents spent 2 weeks or less on elective, and only 11 (12%) residents spent longer than 4 weeks. Longer electives had a significantly greater self-perceived impact than those of shorter duration on clinical knowledge and on awareness of social factors’ effects on child health. Thirty-six percent of those who spent longer than 4 weeks on rotation indicated having a large impact on clinical knowledge versus 15% of those who spent 3 to 4 weeks versus none of those who spent less than 2 weeks (P = .01). Fifty-five percent of those who spent longer than 4 weeks on rotation indicated having a large impact on awareness of social factors versus 32% of those who spent 3 to 4 weeks versus 22% of those who spent less than 2 weeks (P = .04).
Relatively few (27, 29%) resident electives were at a site with a formal partnership with the residency program. Twenty-eight (30%) reported having no mentorship, with 23 (24%) being mentored by Boston Combined Residency faculty, 32 (34%) by an on-site clinician and 11 (12%) by both. Neither formal partnership nor mentorship correlated significantly with elective products or outcomes.
Career Effect
The respondents labeled effect magnitude of the electives as career neutral (33, 35%), career affirming/opportunity expanding (48, 51%), and career-altering: transformational (13, 14%). Forty-two respondents explained the elective’s effect on their career decisions with 11 already planning GH careers before the elective (Table 3). Several shifted focus within GH, often toward research. Eleven respondents reported new plans for a GH career, while 2 moved away from GH careers. Five respondents made subspecialty choices based on their experience, and 10 noted an increased focus on public health.
Pediatric Residency Alumni Qualitative Themes of Global Health Elective Career Impact.

Twenty-eight respondents indicated the GH elective(s) enriched their competence as domestic physicians citing improved cultural competence and ability to serve immigrant patients in the United States. Others reported greater awareness of resource utilization. Four individuals wrote about negative experiences—1 remarking on an experience of poor mentorship and 2 noting feelings of being inadequately prepared for GH clinical work.
Many participants commented on changes in their personal perspectives on their roles in medicine after deep personal reflection on their GH experience.
Ongoing Global Health Work
Overall, 44 (64%) of the respondents described continued work in GH or with underserved (usually immigrant) populations after residency (Figure 2): 32 continued in GH either exclusively or combined with domestic work. Much of this ongoing work was academic with a focus on research or teaching. A minority of respondents continued in direct health care delivery with variations in field time from US-based consulting to intermittent travel to full-time expatriate clinical work.

Ongoing careers in global health.
As one respondent noted, “These resident rotations were the foundations on which I’ve been able to build a career focusing on curriculum development, trainings and health services strengthening in Latin America.”
Discussion
This study supports the educational value, personal impact of GH electives, even when accompanied with minimal formal programming. The study adds to the growing body of information about GH and social medicine career trajectories.
We found that a large proportion of trainees who sought GH electives had substantial prior international field experience. They often returned to sites where they had strong ties to build on previous work or initiate new projects. In keeping with Knowle’s theories on motivation in adult learning, 29 they sought career specific learning opportunities by building on past experience.
The GH electives improved residents’ self-perceived skills as clinicians consonant with findings in previous evaluations, and most significantly in understanding social determinants of health and health systems, and improving cultural competency.1-7 The learning was foundational for many respondents, with some as far as 12 years out of training reporting that the elective shaped their ongoing attitudes for current domestic and GH work.
It is noteworthy that trainees with previous GH experience were more likely to have on-site mentorship. While our data failed to show a correlation between mentorship and the outcomes we measured, literature supports that faculty mentorship ensures appropriate supervision and reduces the imposition on global partners.1,30
“Duration of elective” and “cumulative elective time” correlated with greater elective outcomes. Across GME, stringent ACGME requirements and constraints on resident time may leave programs with minimal flexibility to schedule GH electives. To achieve their educational goals, trainees often combine vacation with 2-week electives to extend their GH elective time—a practice that may be detrimental from a mental health perspective given the intensity of GH electives. 31
Individualized learning has become a priority in pediatric training. While the call for all pediatricians to have some GH training has been made, those trainees who intend to build GH careers are best served by having dedicated time in the field, much as subspecialty fields provide dedicated time in the subspecialty clinic or laboratory.8,32 The data presented here support ongoing development of GH “tracks” that may facilitate a seamless path into one of multiple post-residency GH education opportunities. 25
While some pediatric leaders have expressed concern about career prospects in GH, our results indicate that there are rewarding, high-impact career opportunities seeking well-qualified pediatricians. Of the 44 Boston Combined Residency graduates from 2003 to 2012 who described ongoing careers involving GH and work with the underserved, over half held research and teaching positions focused exclusively in the field of GH.
Our study has a number of limitations. We surveyed alumni only from the Boston Combined Residency program, whose selection committee looks favorably on GH experience as a marker of initiative and leadership. Our response rate was limited by not having contact information for 28 (21%) of the residents who had received travel funds and by a 66% response rate among those whom we did contact. We relied on self-reports of scholarly products and self-assessments of learning, raising risk of inherent “social response” bias, which we tried to minimize by designing questions about the impact of the elective rather than the respondents’ assessments of their own competencies, and by providing detailed anchor statements to Likert-type scales. We also did not evaluate GH elective effects on host institutions or communities, an area that needs further exploration.
Conclusion
Residency training programs are challenged to train physicians who are globally competent, particularly trainees who desire careers combating worldwide disease and disability and closing untenable health disparities. This study points to a high number of residents with experience and career aspirations in GH, the scholarly and educational products of their GH electives, and a correlation between the amount of time spent on GH electives and alumni perception of impact. GH electives for pediatric residents can be life-altering experiences that alter ultimate career choices. Trainees with interest in GH should be supported with individualized GH electives that meet their learning needs and allow them to continue contributing to their chosen field during residency training and beyond.
Author Contributions
CR: Contributed to conception and design; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
TT: Contributed to design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MS: Contributed to design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JP: Contributed to conception and design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Appendix
Acknowledgements
The authors wish to thank Dr Frederick Lovejoy for his support of this work and assistance in identifying study participants, and Drs. Ted Sectish and Bob Vinci for their ongoing support of global health programming.
Authors’ Note
Ethical approval was granted by the Boston Children’s Hospital Institutional Review Board (IRB-P00010672); December 5, 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.