
Abstract
Background. Pediatric obesity has become a significant public health concern. Pediatricians are the ideal group to help identify and treat this epidemic, but unfortunately, many pediatricians are not trained to discuss obesity with patients and their families. Standardized training initiatives for pediatric residents on prevention and/or management of obesity are needed to equip emerging pediatricians to combat the obesity epidemic. Objectives. This systematic literature review aims to examine the effectiveness of childhood obesity prevention/counseling resident training interventions. Methods. A comprehensive literature search was performed using preidentified search terms and limited to articles published prior to November 6, 2019. Articles were analyzed by 2 reviewers with a standardized evaluation tool. Results. A total of 698 articles were identified by the search. These were reduced to 111 articles after title review and 11 articles following abstract/full paper review. The 11 articles described 10 different obesity training interventions for residents. The articles varied in their size, length of training session, and study design. Despite these variations, all articles outlined positive outcomes, including an increase in physician confidence, positive changes in behavior, and/or improved electronic medical record documentation. Conclusions. With the continued increase in pediatric obesity, there is a need for practical, easy-to-implement, standardized trainings for pediatric residents on obesity prevention and treatment. More investigation needs to be done to look at long-term results of current interventions as well as other outcomes such as whether physicians are correctly identifying patients who are overweight or obese and whether there is improvement in patient follow-up.
Keywords
Introduction
Childhood obesity has increased significantly over the past few decades with almost 1 in 5 children meeting criteria for obesity. 1 Over the past 30 years, the prevalence of childhood obesity has more than doubled among children ages 2 to 5 and has practically tripled among children ages 6 to 19. 2 Children with obesity are more prone to be adults with obesity. 3 The comorbidities of both childhood and adult obesity are vast, with medical and financial implications. 4 They range from an increased risk of osteoarthritis to stroke and ultimately death.5,6 As of 2008, the medical care costs of obesity were estimated to be $147 billion. 7 Decreasing the number of children with obesity in the United States and worldwide would affect the health care of future adults and, in turn, make vast improvements in the current national health care expenditure.
Given the frequency with which young children receive care in a clinical pediatric setting in the first 5 years of life, pediatricians are ideal individuals to target for training to prevent and identify overweight or obesity in childhood. 8 Unfortunately, management and treatment of obesity is limited by appropriate diagnosis. 9 Trainees often find discussing obesity with a child and his or her family as one of the more challenging communication scenarios. 10 Despite the frequency with which residents are expected to have these conversations with families, there is minimal standardization of training for pediatric residents on the prevention or management of obesity in pediatric patients. Less than a quarter of all accredited pediatric programs offer a structured teaching curriculum on the evaluation, management, and counseling of patients with overweight or obesity. 11 By improving training at the residency level, residents will graduate from their respective programs and bring with them the skills they obtained during training, thus affecting pediatric populations for decades to come.
A recent systematic review (published in 2019) examined obesity education training programs in medical schools as well as residency and fellowship programs. 12 It was not limited to pediatrics nor to the United States. Most of the 27 articles reviewed reported positive outcomes, but, given the broadness of the search, it is difficult to identify field-specific (ie, Pediatrics) or life stage–specific (ie, children) recommendations. 12 In order to inform pediatric obesity prevention/treatment educational best practices for US residency/fellowship programs treating pediatric patients, we conducted a systematic review of the current literature in order to (1) describe the design of training approaches that have been implemented and (2) examine how the impact of these training approaches have been measured. The primary goal was to identify the effect of the didactic training session on resident behavior and confidence in clinical settings to determine preferred training strategies for pediatric residency programs, and studies were evaluated based on if they demonstrated changes in resident physician confidence, in physician clinical behavior, in patient behavior changes, and in chart documentation. Findings from this review may be used to develop new or implement existing evidence-based approaches to obesity prevention/treatment in pediatric residency programs.
Methods
Search Strategy
We conducted a search using PubMed, Embase, Web of Science, and Scopus databases for studies using the search terms: (pediatric OR child/children/childhood) AND (obese/obesity/overweight) AND (resident/residency/trainee/internship) AND (residency OR medical education OR graduate education) AND (education OR curriculum OR train OR didactic OR lecture OR workshop). Inclusion criteria for this review were that the study (1) addresses resident training on pediatric obesity; (2) describes a teaching modality or intervention targeted to improve obesity screening, diagnosis, treatment, or counseling among children and adolescents; (3) took place in the United States; (4) was published in English; and (5) published prior to November 6, 2019.
Article duplicates were automatically removed from the initial selection. The remaining article titles and abstracts were inspected for relevance by 2 reviewers (LW and MS). This resulted in 111 articles for full-text review for relevance. Articles were excluded if they did not include any characteristics described in Table 2. Articles that were not agreed on by both reviewers were evaluated by a third reviewer (RC) for inclusion criteria and discussed with all reviewers for consensus.
In order to address publication bias (published articles may not accurately reflect the breadth of current curricula), we also searched the Association of American Medical College’s (AAMC) MedEdPortal for any curricula but did not find any additional articles discussing pediatric obesity training in residency programs. There was 1 relevant article that appeared in our search on the MedEdPortal, but it had already presented in our database searches.
A data extraction Microsoft Excel sheet was developed prior to the search by the study team. The reviewers independently completed the extraction sheet for all articles that met the search and inclusion criteria. Articles were reviewed for sample size, geographic area, study design, date range of data collection, residency program, patient age, type of intervention/training, measured outcomes, change in physician confidence, change in physician behavior, change in patient behavior, electronic medical record (EMR) changes implemented, and limitations noted of the study. This allowed for standardization of assessment of study quality and outcomes.
We included all studies in which an intervention was aimed at training a pediatric resident about methods for assessing and addressing childhood obesity. The primary outcomes identified the effects of the didactic training session on resident behavior and confidence in clinical settings to determine preferred training strategies for pediatric residency programs. Secondary outcomes included changes in patient behavior after trainings and changes implemented in EMRs documentation.
Studies that consisted of health care workers that did not include pediatric residents or family medicine residents caring for pediatric patients were excluded from this study. Further studies were excluded if they did not include didactic training interventions, measure outcomes after a training, or were review articles or abstract only.
Ethical Approval and Informed Consent
As this was a literature review, no ethical approval or informed consent was needed.
Results
A total of 698 articles were identified by initial searches in PubMed, Embase, Web of Science, and Scopus. A total of 592 unique articles were identified following de-duplication. These articles were then screened for relevance by 2 members of the research team. Of those, 111 articles met initial criteria by either reviewer and were followed by full-text reviews by each reviewer to determine eligibility. A total of 11 articles met criteria for inclusion in this review. There was no disagreement between the 2 reviewers regarding article eligibility. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram illustrating the process can be seen in Figure 1.
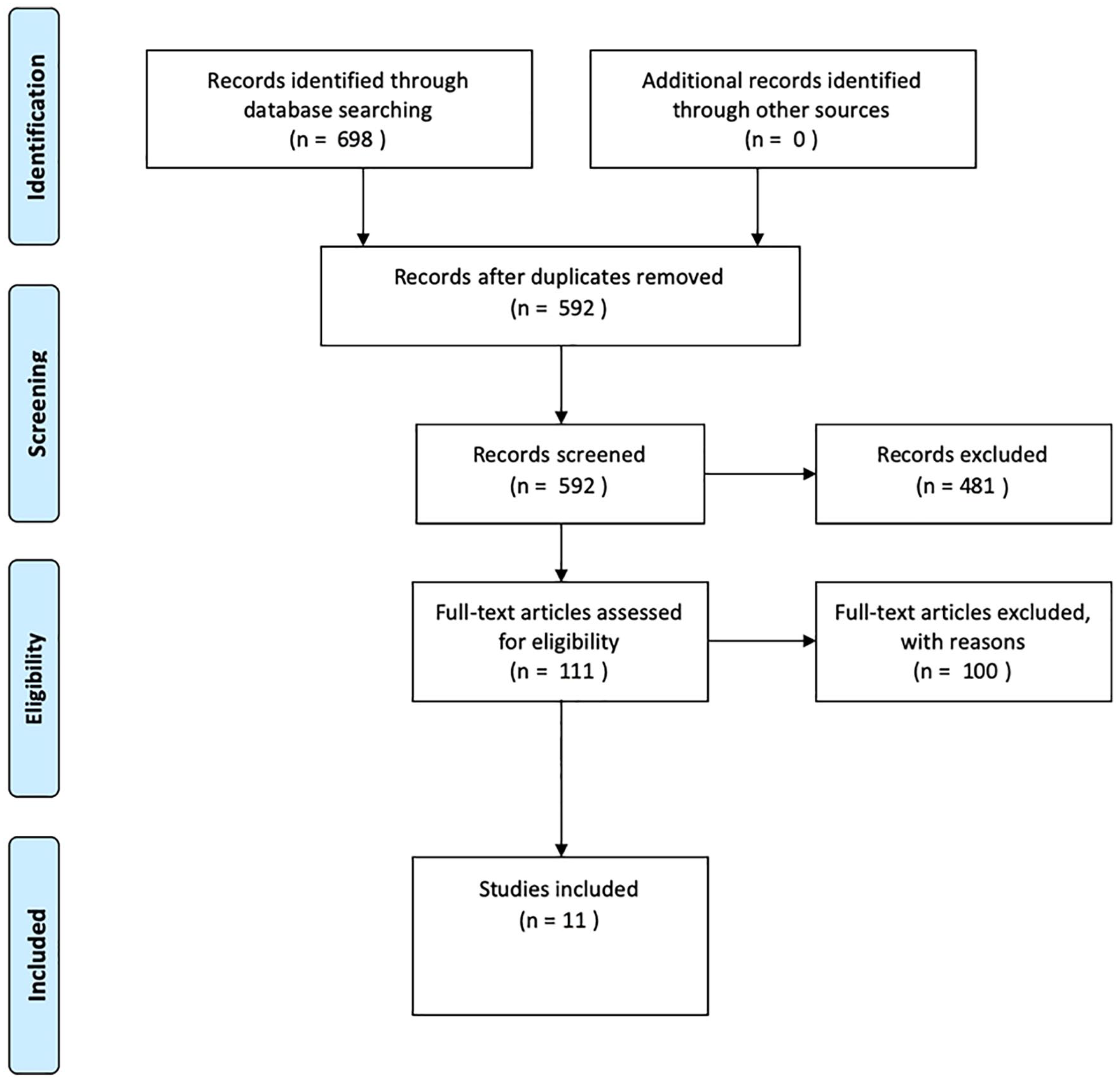
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for article eligibility.
Results are presented under the following headings: study characteristics, intervention implementation, and intervention outcome measures.
Study Characteristics: Setting, Number, and Training Recipients
The 11 articles that met eligibility criteria were published in a range of journals between 2006 and 2019, and all were conducted within the United States. The majority of the studies in this review were single-site studies and were located specifically in an urban setting. Participants in the training included residents at all stages of training. Five of the studies were primarily pediatric residents,13-15 3 included only family medicine residents,16-18 and 3 were a combination of pediatric residents with other specialties (internal medicine, internal medicine/pediatrics, pediatrics/child psychiatry/psychiatry).19-21 Four of the studies included attending physicians,10,15,16,20 one of which included community physicians and not just faculty physicians. 10 Sample size ranged from 6 to 119 physician participants (Table 1).
Study Characteristics.

Abbreviations: BMI, body mass index; EM, emergency medicine; NR, not reported.
Intervention Implementation
The trainings were mostly education-based, but 6 of the trainings included motivational interviewing techniques as well.10,13,16,17,19,21 Many of the training sessions were an hour,10,14,18 with the shortest training session being 15 minutes 15 and the longest training session being a half day in clinic with a nutritionist. 11 In only 2 studies did a small portion of the participants receive repeat training.15,16 Six of the trainings occurred in the outpatient setting,11,15,16,18-20 2 (same study but different articles) occurred during noon conference,10,14 and 2 occurred online.13,21 The trainings that were done in person were led by a variety of clinicians, ranging from psychology residents to nutritionists and board-certified pediatricians (Table 1). The details of 1 study (including the length of the training sessions, where the sessions were conducted, and who conducted the sessions) were not included in the article. 17 Since the articles only provided a brief overview of each training and do not include details of the sessions, it is difficult to assess whether the trainings covered the National Academy of Medicine’s Obesity Training Competencies. 22 Most of the studies do not specifically address obesity training competencies. However, after reviewing the methods, the most frequently cited practices aligning with the competencies were demonstrating a working knowledge of the epidemiology of the obesity epidemic, using patient-centered communication when working with individuals with obesity, and utilizing evidence-based care/services for people with obesity.
Intervention Outcome Measures
To assess the efficacy of the training interventions, we looked at whether each of the 11 studies measured outcomes in the following 4 categories: physician confidence, physician clinical behavior, patient behavior changes, and chart documentation (Table 2). Limitations for each of the studies as described in the text of the individual studies is shown in Table 3.
Study Implementation and Outcomes.

Abbreviations: NR, not reported; EMR, electronic medical record; BMI, body mass index.
Limitations of Included Studies (as Noted by Study Authors).

Abbreviations: EMR, electronic medical record; BMI, body mass index.
Physician Confidence
Physician confidence in obesity counseling and identification skills has been examined, with the implication that increased physician confidence in specific patient care skills is more likely to increase utilization of those skills in clinical settings. Seven of the 11 studies reviewed evaluated physician confidence before and after the training session.10,11,13,15,17-19 All 7 found a significant increase in comfort and perceived competency with various aspects of obesity identification and counseling. Six of the 7 studies did not include a comparison group10,11,13,15,17,19; however, one study specifically compared comfort and competence in a group that had received prior training versus a group of new trainees. 18 The group that had received prior training had a significantly higher level of self-reported comfort and competence compared with the group of new trainees, but both groups did show improvement in every topic following training intervention.
Physician Clinical Behavior
Most of the studies (6 of 11) looked at clinical behavior changes in the physicians, specific to patient interactions.10,11,13,18-20 One study evaluated physician effectiveness at obesity prevention and healthy lifestyle counseling but did not comment on the results. 11 One study discussed subjective behavior changes; the residents self-reported “changes in delivery of care” including being more open-ended in questioning and making more specific recommendations. 13 The remaining studies reported an increase in physician time spent discussing obesity; frequency of discussing diet, physical activity, and weight; and an increase in motivational interviewing techniques. These were evaluated by pre- and posttests, surveys, and chart reviews.
Patient Behavioral Changes
Assessment of patient behavioral changes refers to behavioral changes in the patients and their families regarding their health after the training sessions occurred, with the presumption that they are related to changes in physician management after the training session. Only 2 studies evaluated changes in patient behavior after the training intervention via surveys, and both reported an improvement in patients’ attempts to lose weight via healthier eating, increased physical activity, and/or decreased television time.14,21
Chart Documentation
Electronic medical record reviews provide a systematic method for evaluating whether new practices are being implemented by trainees but is dependent on proper reporting. Only 4 of the 11 studies looked, via chart review, at the effect of the obesity training sessions on EMR documentation.15-17,20 These studies did find improved documentation of body mass index, nutrition and physical activity history, and nutrition and physical activity counseling. Two studies also noted an increase in frequency of follow-up appointments.15,20 Only one study noted an increase in referrals to subspecialists and laboratory tests ordered if obesity was recognized. 20
Discussion
Despite increasing childhood obesity rates over the past 3 decades, the first reports identified by this systemic literature review of obesity training curricula for resident physicians was not published until 2006, and less than one fourth of all Accreditation Council for Graduate Medical Education (ACGME)-accredited pediatric programs currently offer a structured curriculum on pediatric obesity. 8 This systematic review sought to illuminate the various published strategies utilized for training resident physicians on methods for addressing childhood obesity in the clinical setting, and to evaluate which training methods demonstrated improvements in confidence, physician clinical behavior, patient behavioral changes, and/or changes in documentation. Eleven articles were identified, and the training approach, outcomes, and limitations were described.
The training approach and content used within the 11 articles varied; however, most focused on obesity identification and treatment topics, with little emphasis on prevention. Given that a primary goal of pediatric care is based around anticipatory guidance and prevention, this review identified surprisingly few studies on the implementation of preventative strategies in the primary care setting to decrease the rising rates of overweight and obesity. Future training programs should consider incorporating and evaluating obesity prevention strategies in residency training programs.
This review focused on both physician and patient outcomes, including physician confidence, clinical behaviors, and changes in documentation, in addition to patient behavior changes based on parent surveys. Most studies evaluated physician and/or patient outcomes pre-/posttraining, with no comparison group. Given the nuances of residency training, including variability of experience and years of training, a control group would be challenging but needed to account for the differences in skill sets between residents. In addition, most surveys included small sample sizes and were limited geographically to single training programs. Outcome measures varied but included surveys, observation, interviews, and chart review. The majority of the studies found that training residents in childhood obesity prevention/treatment is able to produce an increase in confidence in their counseling skills, in resident satisfaction with these visits, in body mass index recognition and classification, obesity and overweight knowledge, and in weight counseling techniques related to motivational interviewing. Few studies focused on patient outcomes, and none demonstrated long-term weight changes in patients identified as obese. Our home institution used the findings from our initial literature search to institute a new obesity training curriculum for pediatric residents in the outpatient setting. The article analyzing our results is included in the literature review above and aimed to include initially identified gaps in the training outcome evaluations.
Future studies should hone in on the most effective approach to training pediatric residents in pediatric obesity prevention and treatment, including the content/approach, type of training platform (need for refresher sessions or repeat sessions), duration of training most effective, and duration of sustainable effects. There were only 6 published trainings that occurred in 1 hour or less of training time, despite evidence that direct, simple training tools are overall more useful for resident education and comfort in obesity-related counseling in comparison to longer tutorial sessions.10,14,15,18,20,21,23 Given this, an examination of training duration, specifically whether brief training sessions can sustain this efficacy and demonstrate reproducible benefits, is needed. Additionally, only 2 studies documented improvement in expected follow-up visits,15,20 and none investigated the time frame and follow through for these visits to determine if closer evaluations and management took place as a result of these interventions. Finally, it is notable that few studies examine whether, after these trainings, there was correct identification of overweight/obesity based on standard criteria.
Limitations of the review articles include difficulty in interpretation with inconsistency of outcome measures across the studies. This could be addressed in future research with a standardized outcome measure such as a simulated patient or standard documentation practices that could be evaluated on chart review. Such changes, however, would be expensive, time-consuming, and may be difficult to implement across various institutions. Additionally, each study had small sample sizes and were geographically limited at single study sites. Future studies should consider a multisite study, with a goal of larger sample sizes and longer term follow-up evaluations, including postgraduation review. Overall, the heterogeneity of the studies makes generalizability difficult.
Conclusion
With demonstrated increasing rates of childhood obesity, it is necessary to equip pediatric resident physicians with knowledge and skills to help prevent and manage this epidemic. This review demonstrates that childhood obesity educational interventions can be implemented within residency training and leads to improved confidence in obesity counseling, positive physician clinical behavior changes, improved documentation, and positive patient behavioral changes. Further studies on resident training in obesity counseling and intervention are needed to determine whether such interventions lead to improved care and patient-related outcomes, as well as long-term, sustainable changes in physician practices. The ultimate goal should be a standardized evidence-based curriculum for obesity prevention and counseling that can be implemented in pediatric training programs nationwide.
Footnotes
Author Contributions
MS conceptualized and designed the study, assisted in analysis and interpretation of the data, drafted the initial manuscript and approved the final manuscript as submitted.
LW conceptualized and designed the study, assisted in analysis and interpretation of the data, drafted the initial manuscript and approved the final manuscript as submitted.
SS conceptualized and designed the study, assisted in analysis and interpretation of the data, drafted the initial manuscript and approved the final manuscript as submitted.
YW conceptualized and designed the study, assisted in analysis and interpretation of the data, drafted the initial manuscript and approved the final manuscript as submitted.
EH conceptualized and designed the study, assisted in analysis and interpretation of the data, drafted the initial manuscript and approved the final manuscript as submitted.
RC conceptualized and designed the study, assisted in analysis and interpretation of the data, drafted the initial manuscript and approved the final manuscript as submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported with funding by the Maryland State Community Health Resources Commission (Grant #14-018). This funding agency played no role in the study design, data collection, analysis, interpretation of data, or the preparation of this article.