
Abstract
We aimed to evaluate the factors associated with nosocomial infections (NIs) in under-5 children and in bacterial isolates from their blood, urine, and stool. We reviewed all under-5 hospitalized children with clinically diagnosed NIs in the inpatient ward at Dhaka Hospital of International Centre for Diarrhoeal Disease Research, Bangladesh, between January and December 2012. Comparison was made among the children with (cases = 71) and without NI (controls = 142). NI was defined as the development of new infection 48 hours after admission. Bacterial isolates in urine, blood, and stool were found in 11/52 (21%), 9/69 (13%), and 2/16 (12%) respectively. In logistic regression analysis, the children with NI were independently associated with severe acute malnutrition, congenital anomaly, invasive diarrhea, urinary tract infection on admission, and use of intravenous cannula during hospitalization. Thus, identification of these simple clinical parameters may help in preventive measures being taken to reduce the rate of NIs in such children.
Introduction
Nosocomial infections (NIs) are one of the most common complications among hospitalized children. 1 They are responsible not only for increased duration of hospitalization with associated substantial costs, but also for life-threatening morbidity in children. 2 Studies have indicated that young infants and children are at higher risk of NI, and multiple factors such as host characteristics, severity of illness, irrational use of antimicrobials, and use of invasive devices are responsible for this hospital-acquired infection.3,4
A number of recent studies reported NIs among patients of pediatric age groups in the critical care ward to determine the types of infections, their possible etiologies, and predictive factors responsible for NIs. Many of them were from developed countries,1,5,6 which often differ from least-reported developing countries in that most of these studies were conducted in critical care units where state-of-the-art medical facilities were available and the participants were critically ill patients with some invasive procedures such as mechanical ventilation and dialysis as well as postoperative or trauma cases. There were no medical cases with minimum invasive procedures, and patients in general wards were not included in these studies. These studies mainly aimed to evaluate bacterial etiologies rather than the predicting factors.1,7 On the other hand, none of the studies reported NIs from a treatment facility for communicable diseases.
Dhaka Hospital of the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) is the largest diarrheal disease hospital in Southeast Asia and used to receive more than 140 000 patients irrespective of age and sociodemographic characteristics with or without complications such as pneumonia or malnutrition or other health problems. The vast majority (60%) of patients were children younger than 5 years of age, and NIs are not uncommon in this facility. This paves the way to determine factors associated with NIs and their possible etiology, with organisms isolated from biological samples such as blood, urine, and stool.
Materials and Methods
Ethical Statement
Our research did not involve any interviews with patients or caregivers, and it was solely a chart analysis. The data were anonymized before they were received by us.
Setting
Dhaka Hospital of icddr,b is located in Dhaka, the capital city of Bangladesh. The hospital was established in 1962 by icddr,b and currently provides free medical care and treatment to patients with diarrhea and/or malnutrition with or without associated problems and/or complications.
There is an excellent infection control and prevention program running in the Dhaka hospital of icddr,b, supervised by the well-knit infection control team of this hospital. The program includes proper hand hygiene in prepatient and postpatient exposure, use of personal protective equipment, proper practice of disinfection and management of hospital waste products, identification and management of NIs, and most important, postexposure prophylaxis after needle stick injury. The hospital follows these universal precautions in all aspects of patient management. However, there are still some risk factors for NIs in this setup, including close proximity of hospital beds, inadequacy of ventilation, and overcrowding of the patients during diarrhea epidemics at least twice in a year. Dhaka hospital of icddr,b has no restriction in regard to the number of admissions and entertains free of cost.
Definitions used in this study are as follows:
Nosocomial infection: If evidence of new infections was identified at least after 48 hours of admission, they were categorized as NIs. Evidence of new infection was categorized clinically as the development of new clinical features in hospitalized children.
Nosocomial pneumonia: If the there was new evidence of clinical pneumonia (defined by WHO classification of clinical pneumonia 8 ), which was confirmed by chest X-ray (defined by WHO classification of radiological pneumonia 9 ) in under-5 children, that developed 48 hours after hospital stay or after 48 hours of complete resolution (both clinically and radiologically) of pre-existing pneumonia with full course of treatment in the hospital, it was deemed nosocomial pneumonia. The radiological evidence of nosocomial pneumonia in patients who recovered from preexisting admission pneumonia developed in a different lobe of the lung. It is prudent to mention that the children who had recovered from preexisting pneumonia and then developed nosocomial pneumonia stayed at the hospital for the recovery of diarrhea or for nutritional rehabilitation.
Preexisting urinary tract infection (UTI): This was defined as lower-abdominal pain, vomiting, and/or fever with the presence of pus cells (≥10/high power field) and red blood cells (RBCs; any number) in urine routine microscopic examination, with or without bacterial growth in urine.
Nosocomial UTI: This was defined as any clinical sign of UTI (such as lower-abdominal pain, vomiting, and/or fever) developing after 48 hours of hospital stay, with the presence of pus cells (≥10/high power field) and RBCs (any number) in urine routine microscopic examination, with or without bacterial growth in urine (coinfection with noso-comial pneumonia or nosocomial sepsis was not considered).
Nosocomial sepsis: If any new clinical signs of sepsis (defined as tachycardia plus hypothermia [≤35.0°C] or hyperthermia [≥38.5° C], or abnormal white blood cell (WBC) count plus presence or presumed presence of infection 10 ) developed after 48 hours of admission, it was considered nosocomial sepsis.
Severe acute malnutrition (SAM): SAM was defined following WHO anthropometry, which has been described elsewhere. 11
Invasive diarrhea: Passage of visible bloody mucoid stool one or more time(s) within 24 hours. 8
Infection: Tachycardia and/or tachycardia plus hypothermia (≤35.0°C) or hyperthermia (≥38.5°C) or abnormal WBC count. 12
Congenital anomaly: In our study, these are also termed birth defects, and these are structural and functional abnormalities in children, including metabolic disorders, which are present from birth.
Study Design
In this retrospective case-control design, all children 0 to 59 months of age admitted to the inpatient ward (both general ward and intensive care unit [ICU]) of the hospital between January and December 2012 and developed NIs were enrolled as cases. Controls were randomly selected by using SPSS software, with a ratio of 1:2 among those who did and did not develop any NI in the inpatient ward during the same period.
Laboratory Investigations
For children who were admitted in the hospital, routine blood morphology investigations (total count, differential count, and hematocrit percentage) were performed. Suspected children with electrolyte imbalance were also screened by measuring serum electrolytes. Blood, urine, and stool culture were routinely performed only for those children with NIs following standard guidelines for management of NIs and laboratory methods, which has been described elsewhere. 13
Data Analysis
A structured questionnaire was developed, and relevant information was retrospectively collected from the electronic data archive of Dhaka Hospital Patients (SHEBA). Data were entered and analyzed using Statistical Package for Social Sciences (SPSS), Windows (version 17.0; Chicago, IL), and Epi Info (Version 1.0.3, USD, Stone Mountain, GA). We compared differences in proportion using the χ2 test. A probability (α) of <.05 was considered to be statistically significant. Strength of association was determined by estimating odds ratios and their 95% CIs. Several approaches were used to predict differences between children with NI and without NI. First, a comparison between the 2 groups was made to observe an overall difference (Table 1). Then, the type of NIs and the common bacterial isolates in different samples were determined, as shown in Tables 2 and 3. Finally, logistic regression was equated by the enter method to determine the independent risk factors for NIs, where variables that were significant in the 2/2 table analysis but were biologically plausible were considered as independent variables, and NI was considered as a dependent variable (Table 4).
Characteristics of Under-5 Children With Nosocomial Infection Admitted in icddr,b Dhaka Hospital in 2012. a

Abbreviations: NI, nosocomial infection; OR, odds ratio; IQR, interquartile range; WBC, white blood cell; RV, reference value.
Values are given as n (%), unless specified.
Types of Nosocomial Infections According to Our Study Definitions (n = 71).

Abbreviation: UTI, urinary tract infection.
Organism Isolated From the Enrolled Children With Nosocomial Infections.

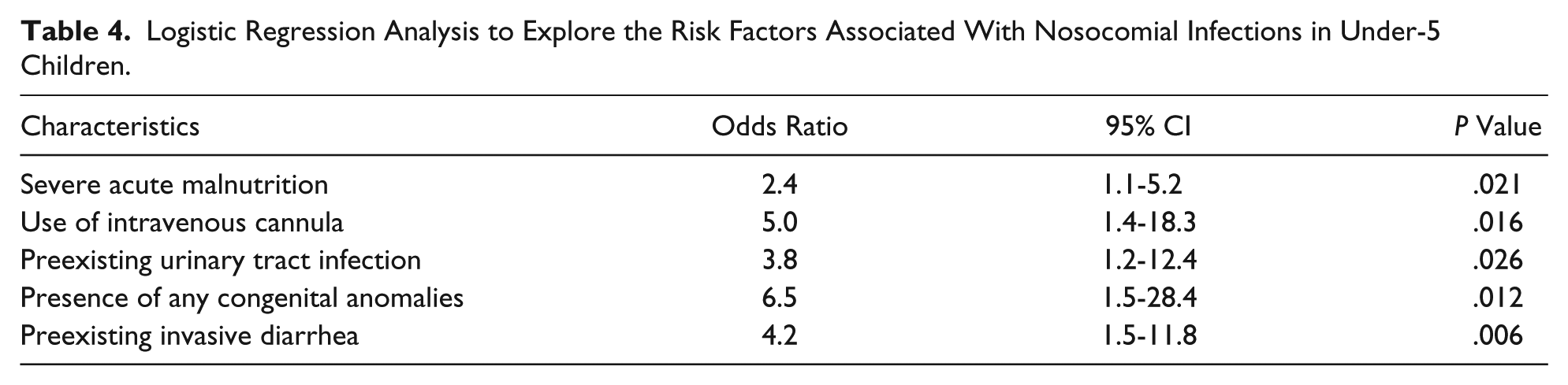
Logistic Regression Analysis to Explore the Risk Factors Associated With Nosocomial Infections in Under-5 Children.
Results
Of the 4321 children, 71 (2%) children were identified as having NIs; 142 were controls. At least 65% of the study children were male, and the median age of the study population was 7.0 (interquartile range = 5.0-10.0) months, with the ratio of boys to girls being 2.8:1. The median ages of the cases and the controls were comparable (Table 1).
Proportion of SAM was significantly higher among the cases compared with controls (Table 1). A significantly higher proportion of the cases had invasive diarrheal disease, UTI, and congenital anomaly, and a higher proportion of them required intravenous (IV) channel or cannula for administering medications such as IV fluid or antimicrobials (Table 1). The cases more often had high white blood cell count and hematocrit (%) on admission compared with their control counterparts; however, serum electrolytes (sodium, potassium) and creatinine were found to have similar distributions. Other clinical characteristics of the patients, such as use of IV fluid, oxygen supplementation and nebulization, common comorbid conditions such as pneumonia, acute watery diarrhea, and sepsis, were statistically comparable among the groups.
Regarding the type of NIs, 84% of the study patients had nosocomial pneumonia followed by hospital-acquired sepsis (13%) and UTI (3%). Among the cases, blood, urine, and stool culture were done in 69, 52, and 16 patients, respectively, and organisms were isolated in 9, 16, and 2 patients, respectively, which is shown in Table 3. In this study, we have observed that among the bacterial isolates in different samples, Gram-negative bacteria were predominant: 12/22 (55%; Table 3).
In multivariate analysis, under-5 children with SAM had 2.4 times, IV cannula users had 5 times, and patients having congenital anomalies had 6.5 times higher risks of developing NIs. On the other hand, children who had a history of UTI and invasive diarrhea had 3.8 times and 4.2 times higher risks for NIs, respectively (Table 4).
Discussion
We observed that pneumonia constitutes 84% of the NIs in our study, which is consistent with that observed in previous studies.14,15 Although 46% of patients had preexisting pneumonia, some of them recovered both clinically and radiologically from community-acquired pneumonia after a full course of treatment and later on developed nosocomial pneumonia, according to our study definition. Most of them had to stay in hospital for the management of their other comorbidities, such as diarrhea, SAM, or dyselectrolytemia. Most of the nosocomial pneumonia could have been a result of viral infection because viruses are the most common causes of NIs in this age group, 16 although we did not perform any investigation to evaluate this. On the other hand, nosocomial pneumonia in our study population may have resulted from aspiration of bacteria from the oropharynx or stomach into the tracheobronchial tree. Approximately 45% of healthy individuals aspirate during sleep, and aspiration is more frequent in patients with ailments requiring hospitalization. 17 Mechanical ventilation–associated pneumonia might be the other cause of nosocomial pneumonia because it is very common in the pediatric population in the ICU,18,19 but in our setting, the rate of developing NI in mechanically ventilated patients was very negligible because of the use of non-invasive continuous positive airway pressure (CPAP) such as bubble CPAP, which significantly reduced the requirement of mechanical ventilation.
Nosocomial sepsis was the second type of NI in this study. We had 9 cases of clinically diagnosed nosocomial sepsis and 9 cases of bacteremia. However, among the 9 cases of bacteremia, only 1 was originally diagnosed as nosocomial sepsis; the other 8 cases were nosocomial pneumonia.
Nosocomial UTI, diagnosed on the basis of our study definition was not a common form of NI in our study population, although 13 other isolates from urine were found as coinfections with nosocomial pneumonia and the remaining 1 isolate from urine was from a patient with nosocomial sepsis. UTI might be one of the causes of sepsis and pneumonia in this age group because most of our children were severely malnourished, and breaches in the integrity of the barrier of the bowel mucosa as well as translocation of bacteria from the gut in severely malnourished children could lead to sepsis and pneumonia. 20
Among the observed bacterial isolates in NIs in our analyses, coagulase-negative Staphylococcus (CNS) was the most common pathogen in blood. Although the chance of contaminants of the CNS and Staphylococcus hemolyticus could not be ruled out, the fulfillment of the definition of NI in these children was critically important. Most of our children were severely malnourished, and in such cases, CNS and Staphylococcus hemolyticus used to be considered as the common causes of NI. 21 Moreover, these organisms as the causes of NIs in other populations has also been reported earlier. 22
In nosocomial UTIs, Escherichia coli was the most common bacteria, although the highest number of nosocomial UTIs were caused by Candida. Almost three-quarters of our children with NIs were severely malnourished, and opportunistic infection with Candida in severely malnourished children is not uncommon. 23 Candida as one of the common causes of nosocomial UTI in well-nourished children has also been reported earlier. 24 Among all the bacterial isolates causing NIs, Gram-negative bacteria were the predominant ones, and this has also been reported earlier.1,7
We also found 2 enteric bacteria in stool samples of 2 different patients with nosocomial pneumonia because these 2 patients also had new episodes of diarrhea as coinfection with nosocomial pneumonia. It is true that these 2 organisms are usually found in community-acquired infection, and it is difficult to make inferences as to whether these 2 organisms contributed to the development of any nosocomial pneumonia at all.
Our observation of Moraxella and Pseudomonas bacteremia and Pseudomonas bacteriuria is not uncommon in ICU patients. 25 Actually, these patients were required to initially stay in the ICU for their severe ailment and then transferred to the general ward after initial improvement in the ICU (ICU and general ward were termed inpatient departments).
Our observation of SAM, congenital anomaly, invasive diarrhea, UTI on admission, and use of IV cannula during hospitalization as independent predictors of NIs is very important because this is the only study that evaluated this information predominantly in a population of children with diarrhea.
Our observation of use of IV cannula as an independent risk factor for developing NI in this study is understandable. Intravenous lines provide both a break in the skin, allowing entry of organisms, as well as a protected site for bacterial growth shielded from immune defenses by a biofilm of platelets, fibrin, and bacterial slime. The risk is greater with increasing duration of the line, central and multilumen lines, and poor insertion technique or line care, which may lead to infection of the insertion site or hub. 26
In all, 77% of our study population had SAM. It has been observed that malnutrition plays an important role in developing NI. Severely malnourished children have depressed cell-mediated as well as humoral immune responses, and they are more susceptible to infection. 27 Besides, this poor nutritional status has also been associated with nosocomial pneumonia and led to early nutritional support for critically ill patients. 28 Early enteral feeding may help maintain the epithelial barrier and prevent pneumonia caused by translocation or migration of bacteria across the gastrointestinal epithelial barrier. 23 Some investigators have postulated that administration of enteral feedings with high pH via the oral gastric tube may increase gastric colonization, volume, pressure, reflux, and pneumonia.29,30 Maintaining the patient in the upright position appears to reduce the frequency of gastric reflux. In addition, care should be taken to prevent contamination of enteral feedings, and vigilance is needed for their administration.31,32
Our observation of NIs in preexisting invasive diarrhea is novel. Although there were no published data, a significantly higher proportion of our children with NIs had severe malnutrition, in whom bacteremia is quite common. 13
In this study, we have also observed that some predisposing infections or comorbid conditions such as UTIs and presence of any congenital anomalies (eg, cleft lips, cleft palates, Down’s syndrome, congenital heart diseases) provoked the development of NI, and they are independent predictors of NI in under-5 hospitalized children. Preexisting infection was a significant risk factor for NI. This was similar to the findings in a multicenter cohort, in which 45% of NIs occurred in patients with preexisting infection.33,34 In the study group, preexisting UTI constituted 14% of the cases. The reason why patients with preexisting UTI develop NI is not clear. However, it might be a result of the translocation of bacteria from the urinary tract, with development of systemic manifestation later. On the other hand, probably there were some cases that had a symptom-free period of preexisting UTI, which eventually became evident after 48 hours of hospitalization. The patients with congenital anomalies may have some difficulties in their normal body physiologies, which is often associated with compromised immunity, 35 and may be susceptible to new infections in hospital settings.
The main limitation of our study is its retrospective nature of identifying risk and bacterial etiology, which prevented us from collecting information on a broader range of variables that may have been potential additional risks. Second, the limitation in the number of patients included in this study might have reduced the ability to identify more subtle differences between the groups and identify further relevant risks for NI. Third, we did not perform any viral isolation, which could have been one of the most common causes of NI in our study population.
In conclusion, our data suggest that hospital-acquired pneumonia plays a substantial role among the NIs in under-5 hospitalized children who are mainly admitted with diarrhea. Under-5 hospitalized children predominantly admitted with SAM, any congenital anomalies, preexisting infection with UTI, or invasive diarrhea and/or use of IV cannula for treatment are prone to develop NIs. The main organisms responsible for NIs were Gram-negative bacteria, which underscores the importance of using extended spectrum antibiotics for their adequate treatment; this may reduce morbidity and deaths from NIs in such children. However, large-scale multicenter prospective studies with children hospitalized for diarrhea may provide more information about the potential preventive measures for NIs in such children.
Author Contributions
KMS contributed to the conception and design; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. TA contributed to the design, critically revised the manuscript, and gave final approval. ASGF contributed to interpretation of data, critically revised the manuscript, and gave final approval. ASMSBS contributed to the design, critically revised the manuscript, and gave final approval. SKD contributed to analysis of data, critically revised the manuscript, and gave final approval. LS contributed to acquisition of data, critically revised the manuscript, and gave final approval. MIH contributed to the design, critically revised manuscript, and gave final approval. MMI contributed to conception, critically revised the manuscript, and gave final approval. MJC contributed to the conception and design, contributed to analysis and interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research protocol was funded by core donors which provide unrestricted support to icddr,b for its operations and research. Current donors providing unrestricted support include: Government of the People’s Republic of Bangladesh; the Department of Foreign Affairs, Trade and Development (DFATD), Canada; Swedish International Development Cooperation Agency (Sida) and the Department for International Development (UK Aid). We gratefully acknowledge these donors for their support and commitment to icddr,b’s research efforts.