
Abstract
Functional gastrointestinal disorders (FGIDs) are a common problem in pediatric patients and can affect quality of life. However, the extent of these disorders may vary in different subpopulations of children. This study investigated the prevalence of FGIDs in an inner-city primary care practice. Healthy patients between the ages of 9 and 17 were administered a validated questionnaire that assessed for FGIDs and other somatic complaints. Eleven of 145 patients (7.5%) met criteria for FGIDs based on Rome III Diagnostic Criteria. Raynaud-like symptoms tended to occur more often in patients meeting criteria for FGIDs, although this association was not statistically significant (P = .07). The lower prevalence of FGIDs in this population compared with earlier studies may suggest a link between socioeconomic status and the prevalence of FGIDs. Larger population-based studies consisting of a heterogeneous cohort from a variety of socioeconomic backgrounds are necessary to further elucidate the true connection between FGIDs and socioeconomic status.
Keywords
Introduction
Recurrent abdominal pain (RAP) is common among children, leading to absence from school and impaired quality of life. 1 A recent systemic review, including studies with a variety of definitions for RAP, found a prevalence as high as 19% in children. 2 The Rome III Diagnostic Criteria established a uniform method of classifying RAP into different categories of functional gastrointestinal disorders (FGIDs), such as abdominal migraine, cyclic vomiting syndrome, functional abdominal pain syndrome, functional dyspepsia, and irritable bowel syndrome.
External factors may influence the development of FGIDs. Although the data are limited, children of lower socioeconomic status may harbor a higher risk for developing RAP.3,4 Many children with FGIDs have comorbid psychological disorders, including anxiety and depression.1,5 Preliminary data from tertiary referral centers also suggest a relationship between FGIDs and somatic comorbidities, such as migraine headaches, fibromyalgia, sleep disturbances, and chronic fatigue. However, these associations were found in a self-selected, more affected population and may not be present in all children with FGIDs. 6
This study aimed to investigate the prevalence of FGIDs in an inner-city primary care pediatric clinic in the United States using Rome III Diagnostic Criteria. A secondary aim was identification of comorbid nonpsychiatric symptoms among children meeting criteria for FGIDs in this population.
Methods
This cross-sectional questionnaire study was approved by the University Hospitals Case Medical Center Institutional Review Board. It was conducted between August 2012 and May 2013 at a large urban primary care clinic in Cleveland, Ohio. Healthy patients between the ages of 9 and 17 seen in clinic for well-child visits were recruited. Parents provided written informed consent, and participants provided written assent. Patients in clinic for a sick visit or patients with a history of organic gastrointestinal disorders including inflammatory bowel disease, cancer, celiac disease, liver disease, peptic ulcer disease, and food allergies were excluded.
A modified version of the Ohio Dysautonomia (ODYSA) instrument was administered to participants (see the appendix). The questions were read aloud and the answers were recorded by a study coordinator. The ODYSA is a comprehensive survey of somatic symptoms across organ systems developed for both adult and pediatric use. 7 It uses validated published question sets where available (e.g. Rome III modular questions for FGIDs, International Headache Association criteria for migraine headache symptoms, and the Epworth Sleepiness Scale for daytime sleepiness) or, alternatively, face-valid questions.8-14 The ODYSA instrument was modified by removing question-sets relevant only to adults. Besides FGIDs, the ODYSA instrument assessed participants for migraine headache symptoms, recurrent syncope, daytime sleepiness, chronic body pains, chronic fatigue, urinary frequency (defined as feeling a strong need to urinate with little or no warning), orthostatic symptoms, and Raynaud-like symptoms (defined as fingers or toes turning white, red, or blue on cold exposure).
Statistical analyses were performed using SAS version 9.3 (SAS Institute Inc, Cary, NC). The prevalence of FGIDs and other somatic complaints were summarized descriptively using frequency and percentage. Demographics were compared between patients with and without FGIDs using Fisher exact tests and Wilcoxon 2-sample tests. The association between FGIDs and other somatic complaints were examined using Fisher exact tests. Two-sided P values were reported; P < .05 was considered statistically significant.
Results
A total of 165 patients were approached for the study. Eight patients refused participation and 12 patients were excluded due to food allergies. Participant demographics are described in Table 1. Of the 145 participants, 11 (7.6%) fulfilled criteria for FGIDs. A proportion of patients fulfilled criteria for several FGIDs, most commonly abdominal migraine (Table 2).
Demographics and Overall Somatic Symptoms in Patients With and Without FGIDs.
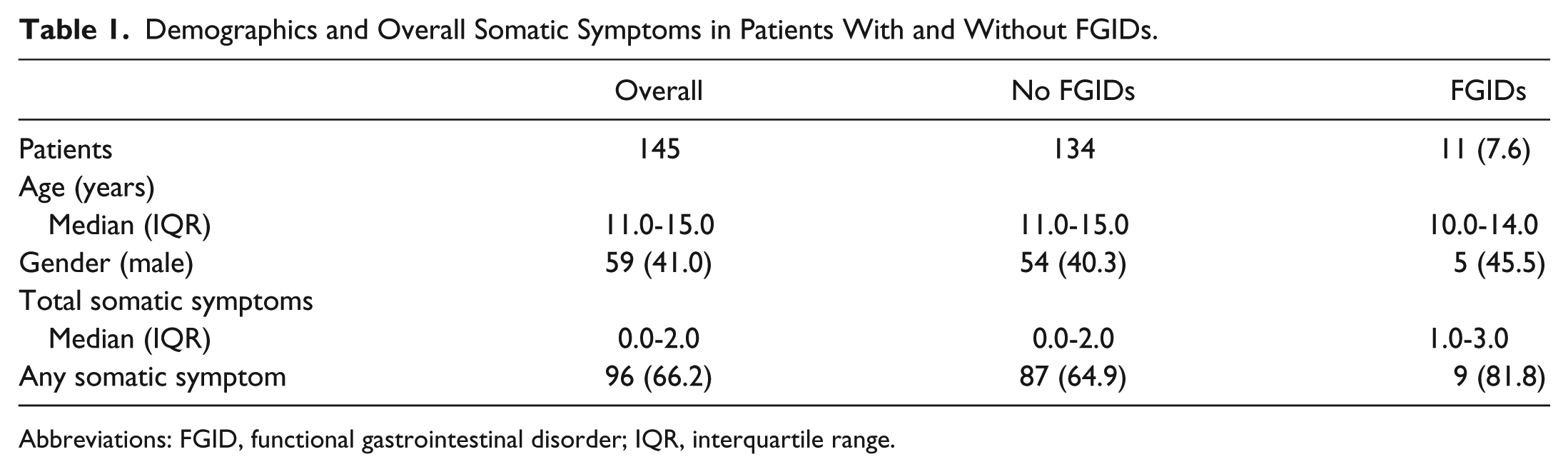
Abbreviations: FGID, functional gastrointestinal disorder; IQR, interquartile range.
Characteristics of the Patients With FGIDs.

Abbreviation: FGID, functional gastrointestinal disorder.
The prevalence of each somatic complaint in this cohort is shown in Figure 1. Somatic complaints were reported in 66.2% of patients. Daytime sleepiness was the most common complaint, reported by 39.3% of patients. Raynaud-like symptoms occurred more often in participants with FGIDs, and while trending toward significance, there was likely inadequate power to achieve true statistical significance. Raynaud-like symptoms were reported in 3/11 (27.2%) of participants with FGIDs as compared to 11/134 (8.2%) of participants without FGIDs, P = .07. No statistical association was found between FGIDs and the other symptoms investigated (Figure 2).

Prevalence of somatic complaints in all patients.

Somatic complaints in patients with and without FGIDs.
Discussion
FGIDs, while not extensively studied, are highly prevalent and often underrecognized in the pediatric population. Children with FGIDs may manifest symptoms that affect physical and emotional well-being as well as have a negative effect on academic performance. Overall, it is a significant cause of impaired quality of life in pediatrics. In order to provide better care for children with FGIDs, it is necessary to understand the extent of the disorder, identify potential associated risk factors, and recognize comorbid conditions.
This study investigated the prevalence of FGIDs in an inner-city primary care pediatric practice in the United States and found the prevalence using Rome III Diagnostic Criteria to be 7.6%. To our knowledge, this is the first study investigating the prevalence of FGIDs based on Rome III criteria in this population. Previous studies report the prevalence of RAP to be as high as 19%. 2 There are several reasons why this study population may have had a lower prevalence of FGIDs. First, whereas other studies defined RAP in a variety of ways, this study used Rome III Diagnostic Criteria, which has strict diagnostic cutoffs. Additionally, whereas several Scandinavian studies suggested that socioeconomic status may be associated with RAP,3,4 this is the only known US study to investigate this association. The results of the current study may suggest a lower prevalence of FGIDs among US children of low socioeconomic status. Further research will need to investigate the association between socioeconomic status and FGIDs among children in the United States.
Another difference found in this study, compared with prior literature, was the high prevalence of abdominal migraine, typically present in only a small portion of the population. 15 Our cohort is too small to meaningfully interpret this finding, but this does suggest that the prevalence of FGIDs and the predominant type of FGIDs should be further investigated in this population.
Additional thought-provoking findings from this data set include the high prevalence of any somatic symptom, daytime sleepiness, and orthostatic symptoms in this population, regardless of the presence or absence of FGIDs. The high prevalence of these symptoms in an unselected group of subjects without FGIDs is surprising and requires further investigation to understand the basis of these findings.
The main limitations of this study include the small sample size and the use of a questionnaire as a diagnostic tool rather than physician assessment. Additionally, participants with food allergies were excluded from the study—possibly lowering the prevalence of FGIDs in the study population.
In summary, the lower prevalence of FGIDs in this study compared to previous studies may suggest a link between socioeconomic status and the prevalence of FGIDs. Additionally, these data are consistent with the prior literature that depicts an association between FGIDs and other somatic complaints, 7 such as Raynaud-like symptoms, although likely related to the small sample size this was not statistically significant in our study. A similar population-based study with a larger sample size and a heterogeneous cohort from a variety of socioeconomic backgrounds may provide new insight regarding any possible association between FGIDs and socioeconomic status.
Footnotes
Appendix
Acknowledgements
The authors are thankful to Carol L. Rosen, MD, Division of Pulmonology at Rainbow Babies and Children’s Hospital, Judith Kelsen, MD, Division of Gastroenterology at The Children’s Hospital of Philadelphia, and Jacquelyn Hatch-Stein, Division of Endocrinology at The Children’s Hospital of Philadelphia for their valuable suggestions during the editing process.
Declaration of Conflicting Interests
Thomas Chelimsky, MD, was a member of the Advisory Board for Ironwood Pharmaceuticals in 2014. The authors have otherwise declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.