
Abstract
Background. Asthma results in significant pediatric hospitalizations in the inner city. Many asthmatic children were admitted to our hospital as a result of lack of medications or medical supplies that had been previously prescribed (“ran out,” “broken,” or “lost”). Objective. To identify the incidence of children admitted for asthma because of lack of prescribed medications/supplies and to assess risk factors for poor adherence between groups. Methods. This was a prospective chart review of 200 asthmatic children admitted to Children’s Hospital of Michigan, Detroit. The data included asthma severity, lack of prescribed medications/medical supplies, and outpatient management. Results. In all, 35.5% or 71/200 of asthmatic children admitted had lack of prescribed medication/supplies (9% lacked both). The most common deficiency was β2-agonist (20.5%; 41/200). Teenagers had the highest lack of medications/medical supplies (55.6%; 5/9) compared with toddlers (17.2%; 16/93) and preschoolers (17.9%; 5/28). Patients with severe persistent asthma had a higher incidence of lacking medicine (31.8%; 7/22) compared with 25% (14/56) with moderate persistent asthma and 23.4% (15/64) of mild asthmatics. We found the lack of asthma medical supplies, including nonfunctioning or lost nebulizers/spacers, in 44.4% (4/9) of teenagers, 17.2% (16/93) of toddlers, and 21.4% (6/28) of preschool-aged children. We found no significant difference in these deficiencies whether patients were managed by asthma specialists or primary care providers. Conclusions. Significant numbers of asthmatic children admitted reported lack of prescribed medications/medical supplies. The most severe asthmatics were most likely to run out of medications. Interventions targeted at these deficiencies may avoid hospitalizations.
Introduction
Asthma is one of the most common chronic inflammatory diseases, affecting approximately 10 million children and 30.5 million adults in the United States. 1 Despite new management guidelines and strategies, asthma remains a significant cause of pediatric emergency department visits and hospitalizations, especially in the inner city. Contributing factors for poor asthma control in this risk group include poor adherence, poor perception of asthma symptoms, and medical beliefs that contradict prescribed treatment associated with poor adherence, estimated to be 25% to 85%.2-7 Factors associated with poor asthma control also include low socioeconomic status, stress, specific allergens, adolescence, male gender, and exposure to pollutants.5,8-12
Apart from prevention, the best strategy for management of asthma exacerbations is early treatment. Important elements of early treatment at the patient’s home include patient education with a written asthma action plan, training on the recognition of early signs of worsening asthma, prompt action, removal or withdrawal of environmental factors contributing to the exacerbation, prompt communication between patient and clinician, and appropriate intensification of therapy by increasing inhaled short-acting β2-agonist and, in some cases, adding a short course of oral systemic corticosteroids (Evidence A). 13 A major focus of research has been on the development of strategies to improve adherence, with most evidence focused on shared decision making, improved communication, and training to early identification of barriers to treatment.14-16
Many asthmatic children were admitted to our hospital in part because of lack of (“ran out,” “broken,” or “lost”) medications or medical supplies, including nonfunctioning nebulizer machines/lost spacers at home. Although, most teenagers and school-aged asthma patients are able to use inhaled β2-agonists via spacers relatively well, in our hospital, we found that many of these patients preferred to use β2-agonists via home nebulizers during acute asthma exacerbation (probably because of shortness of breath and also because of the higher dose delivered in a nebulized treatment compared with the usual 2 puffs of the inhaler). Most of our patients, even severe asthmatics with “experience,” do not use meter-dosed inhalers well without a spacer device. We sought to identify the true incidence of hospitalized asthmatic children who reported their lack of asthma medications and medical supplies and identify patterns of age and asthma severity associated with poor adherence to keeping medicines and medical equipment available.
Methods
We performed a prospective chart review of 200 asthmatic children admitted to Children’s Hospital of Michigan in Detroit. This study protocol was approved by the Wayne State University and Detroit Medical Center Institutional Review Boards (IRBs). The data were gathered from December 2008 through March 2010. The information included age of the patients, gender, clinical asthma severity, the lack of asthma medications and type of the medications that were unavailable (β2-agonist and/or inhaled corticosteroid), the lack of medical supplies (nonfunctioning home nebulizer or home nebulizer/spacer was not available), and whether the patients were managed by an asthma specialist or a primary care provider. All data analyses were performed using SPSS version 17.0. 17 Categorically scaled variables were reported using a frequency command, with proportions and ratios. Continuously scaled variables were reported using means, SDs, and medians. Comparisons between categorically scaled variables were conducted using cross-tabulations, with proportional differences tested for significance using either a Pearson’s or Fisher’s exact test. Where appropriate, continuously scaled variables were examined between groups using either a Mann-Whitney U or Kruskal-Wallis test. Statistically significant differences were considered achieved at a P value ≤.05, 2-tailed. Descriptive analyses were performed by using mean, frequency, and SPSS. Subgroups analyses were performed by using Fisher’s exact test at 95% CI for P value. The parameters for subgroups analyses included the lack of asthma medication and the lack of medical supplies for asthma, compared in each asthma severity category, age groups, gender, and management by either an asthma specialist or primary care provider.
Results
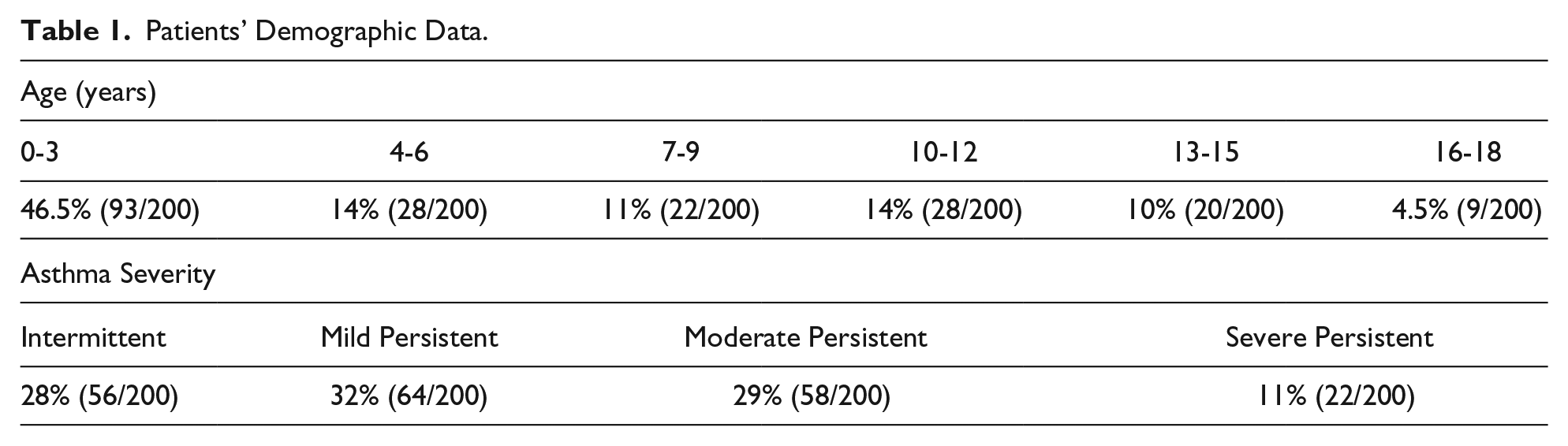
The majority of asthma patients in our study were 0 to 3 years of age: 93/200 (46.5%). Out of 200 patients, 119 (59.5%) were male and 81 (40.5%) were female. In regards to asthma severity, 56/200 (28%) had intermittent asthma, 64/200 (32%) had mild persistent asthma, 58/200 (29%) had moderate persistent asthma, and 22/200 (11%) had severe persistent asthma. The majority of our patients (156/200 [78%]) were managed by their primary care providers, whereas 44/200 (22%) were managed by an asthma specialist (see Table 1).
Patients’ Demographic Data.
Greater than a third (71/200 or 35.5%) of asthmatic children admitted to our hospital had either a lack of asthma medication or a home nebulizer machine/spacer device. Of these patients, 18/200 (9%) had a deficiency in both medicine and medical supplies. The most common deficiency was β2-agonists: 41/200 (20.5%). We found that 16/200 (8%) patients ran out of controller medication and 13/200 (6.5%) ran out of both controller and rescue medications. Of 200 patients, 44 (22%) had either a nonfunctioning home nebulizer (33/200 [16.5%]) or the nebulizer/spacer was not available (ie, lost in move or lost in fire were most common responses; 11/200 [5.5%]).
By using the lack of asthma medication as the parameter, we found that teenagers had significantly more problems with a lack of medication (5/9 [55.6%]), compared with toddlers (16/93 [17.2%]; P = .017) and preschool-aged children (5/28 [17.9%]; P = .027). Severe persistent asthmatic children trended toward more problems with lack of their medications than those with other subtypes of asthma severity, although there were no statistical differences found between each asthma severity category (see Table 2).
Subgroup Analysis Using Lack of Medication as Parameter.

Compared with teenager group (16-18 years of age).
Compared with severe persistent asthma.
Similarly, there were no statistical differences for the lack of asthma medication between patients who were managed by primary care providers (35/156; 22.4%) or asthma specialists (10/44; 22.7%; P = 1) or gender of the patients (male 28/119 [23.5%], vs female 17/81 [21%]; P = .732).
Regarding the lack of medical supplies, teenagers seemed to have more problems with a nonfunctioning or nonavailable home nebulizer/spacer compared with other age groups. However, no statistically significant differences were found by age group, asthma severity level, gender, prescriber of medication (specialist vs primary care), or a lack of medical supplies (see Table 3).
Subgroup Analysis Using “Lack of Medical Supplies” as Parameter.

Nonfunctioning home nebulizer or home nebulizer was not available.
Compared with teenager group (16-18 years of age).
Compared with severe persistent asthma.
Patients who ran out of their asthma medications were significantly more likely to have more problems with a home nebulizer/spacer availability (18/45 [40%]) than patients who had their asthma medications (26/155 [16.8%]; P = .002).
Discussion
Many studies in the past investigated and discussed approaches to improve care in inner-city asthmatics. These included identifying key risk factors for asthma morbidity, defining mechanisms of immune system deviation and immune tolerance, educational programs, and an EPR-3 guidelines-based approach as well as incorporating shared decision making.12,14-16,18-20 A study identifying risk of asthma morbidity found poor medical adherence in more than one-third of inner-city patients. 21 Others have identified adherence difficulties associated with limited knowledge, lack of motivation, inconvenience, challenges with parental support, and poor provider communication as critical areas contributing to nonadherence.7,16 To our knowledge, details in poor medical adherence, including running out of asthma medication and the lack of home nebulizer/spacer, have not been clearly identified. Our study revealed that significant numbers of hospitalized asthmatic children report lack of obtaining and refilling prescribed medications and medical supplies, especially the severe persistent asthmatics. We conclude that interventions such as home delivery or refill reminders may avoid these preventable hospitalizations. Further investigations and research need to be conducted in this area to identify very specific risk factors for these adherence issues and, likewise, very specific interventions. The awareness in asthma prevention and management in physicians, health care personnel, and the parents of asthma children should be encouraged and emphasized. The limitations of our study included distribution of our participants, such as the small number of participants with severe persistent asthma and a limited number of patients older than 15 years. The interpretation of data in these subgroups of patients limits statistical comparison with other subgroups of patients.
Author Contributions
PP: Contributed to conception and design; contributed to analysis; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
BH: Drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RT: Contributed to analysis; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ES: Contributed to conception and design; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Acknowledgements
We would like to acknowledge Wafe Alam, RN, for her assistance with data collection and chart review for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.