
Abstract
Introduction
Speech and language delay (SLD) is a common developmental problem that affects 3-20% of children globally, with significant long-term consequences if left untreated. Despite extensive research on SLD risk factors, regional studies in Palestine remain limited. This study sought to identify key characteristics impacting SLD in Palestinian children aged 2 to 10 years.
Methods
Between January and March 2025, a case-control study was conducted at ten specialized institutes in Palestine. The study included 184 children with SLD and 136 controls who were matched for age and gender. Data were collected using standardized questionnaires that assessed socio-demographic, biological, familial, and environmental factors. SPSS v26 was used for statistical analysis, which included chi-square tests and logistic regression (p-value < 0.05 indicated significance).
Results
Significant risk variables for SLD were rural residency (OR = 4.4, p = 0.008), lower parental education (paternal p = 0.003; maternal p < 0.001), and low family income (OR = 2.5, p = 0.030). Maternal employment showed a protective effect (OR = 0.273, p < 0.001). Biological characteristics such as ENT issues (OR = 3.9, p = 0.012) and a family history of SLD (OR = 8.6, p = 0.001) were significantly linked with SLD. There was no substantial correlation between the multilingual surrounding environment and family size.
Conclusion
The study emphasizes the diverse characteristics of SLD in Palestinian children, with a focus on socioeconomic disparities, biological factors, and familial history. These findings emphasize the necessity of targeted early therapies, particularly in rural and low-income populations, to mitigate the long-term impact of SLD.
Introduction
The global prevalence of speech and language delay (SLD) ranges from 3% to 20%, with approximately 5% of primary school-aged children exhibiting a delay in speech and language. 1 40–60% of children with untreated SLD may experience persistent difficulties, raising their chance of developing cognitive, emotional, behavioral, and social problems as adults.1–4 Children with this issue may experience difficulties with autonomy and possess a higher risk for psychological disorders in adulthood. 5 Teenagers with speech difficulties show significant behavioral and emotional symptoms compared to their typically developing peers, with 35–50% requiring assistance. 6
Screening for speech and language delays or disorders among children who do not have a known condition that affects speech and language development aims to detect these conditions early and provide effective interventions before they interfere with school learning or psychosocial adjustment. 7 Numerous factors are associated with SLD. Research conducted in Eastern India and Iran found a higher frequency of SLD among males,8,9 however, SLD was more common in women in Nepal. 10 SLD are significantly correlated with consanguinity, low parental education, poor communication, monolingualism, and family history.8,10–13 Preterm delivery, infectious diseases, birth asphyxia, oropharyngeal anomalies, convulsions, neonatal difficulties, and prenatal alcohol consumption are all important predictors of SLD.4,11–14 According to research from Bangladesh and Nepal, inadequate nutrition was linked to a higher incidence of SLD. 10 Furthermore, this condition is linked to negative home situations, difficult family dynamics, and excessive screen time.4,9 Otitis media is an additional risk that can result in hearing loss as well as difficulties with speech and language development. 15 Using pacifiers, dummies, thumbs, or bottles, among other sucking practices, can result in oro-motor dysfunction and oral sensory problems. 16
Every child has to have their speech, language, and hearing issues evaluated. Delays in diagnosis and treatment might result in irreversible cognitive decline, which can include low IQ, communication problems, and illiteracy. 16 While language or speech disorders relate to situations where speech or language ability deviates from what is anticipated as normal development, language or speech delays refer to situations where the development of the ability to understand and speak is right but slower than what is considered normal.17,18 Disorders of language and speech can occur independently or in combination with one another. 18 There are, however, difficulties associated with the identification of children who have language and speech delays through the use of universal screening. These children are a diverse group that is difficult to analyze using a straightforward screening instrument due to the fact that they are influenced by cultural, socioeconomic, and contextual factors. 19 In addition, SLD research in Arab countries is scarce, and none to our knowledge, have analyzed Palestinian cohorts. The development of strategies for preventing SLD may result from an analysis of risk variables, and it is essential to comprehend the underlying causes. Thus, the purpose of this study is to investigate the factors that influence speech and language delay in children between the ages of two and ten in Palestine.
Methods
Study setting, period, and design
A case-control study was undertaken from January through March 2025 at ten different institutes specializing in the treatment and education of children with speech impairments, all located in urban centers. Given the variety of speech and language therapy choices accessible nationwide, these facilities were chosen as research locations. This grants access to children from diverse socioeconomic backgrounds, yielding a representative sample for the study. Age- and gender-matched control participants were recruited from nearby primary schools, kindergartens, and daycare centers within the same catchment areas as the participating institutes.
Dependent variables
Speech and language delays in children aged 2–10 years.
Independent variables
Sociodemographic characteristics include age, gender, domicile, maternal and paternal education, mother’s and father’s occupations, monthly income, economic status, nature of father’s employment, type of school attended by the child, and number of siblings. Biological characteristics (illness, severe injury, or hospitalization; hearing problems; seizure disorders; middle ear infection; other ear, nose, or throat (ENT) problems; oral cleft or deformity; oropharyngeal deformity; maternal history of hypertensive disorder during pregnancy; consanguinity of parents; father’s and mother’s ages at childbirth). Feeding-related features (thumb-sucking history, pacifier-use history, and feeding history). Features associated with the family (number of family members, divorce, father’s absence from home, multilingual family environment, SLD history, and family type). Environmental factors include the child’s screen time and any recent stress or trauma they have experienced.
Inclusion and exclusion criteria
Sample size determination and sampling method
The minimum required sample size was calculated using the double population proportion formula in Epi Info version 7.2.2.6, assuming a 95% confidence interval, 80% statistical power, a 5% margin of error, and a planned 1:2 case-to-control ratio. 20 The best estimated sample size among the risk factors was 107. To account for a 10% non-respondent rate, the sample size was expanded to 120, comprising 40 cases and 80 controls. This figure represented the statistically derived minimum enrollment threshold, not a cap on total recruitment.
Recruitment followed a consecutive sampling approach throughout the study period (January–March 2025), whereby all children meeting the predefined eligibility criteria at the ten participating institutes whose guardians provided written informed consent were enrolled. Controls were similarly recruited from primary schools, kindergartens, and daycare centers within the same geographic catchment areas. As the number of eligible participants identified across the participating sites exceeded the minimum required sample, recruitment was not restricted to the calculated threshold. This approach was adopted to enhance statistical power, improve representativeness across diverse geographic and socioeconomic groups, and reduce the risk of type II error.
The final sample comprised 320 participants (184 cases and 136 controls), substantially exceeding the minimum requirement and thereby improving the precision and reliability of the study findings. The final case-to-control ratio (approximately 1:0.74) differed from the initially planned 1:2 ratio, reflecting differences in participant availability during recruitment rather than any modification to the study design. Unequal case-to-control ratios are methodologically acceptable in case-control studies, and all participants were enrolled strictly according to the predefined eligibility criteria.
Data collection and procedures
Following a thorough analysis of pertinent literature sources, the structured questionnaires included in the interviews were meticulously created.9,11,20–31 The questionnaire (Supplementary file) was divided into five categories based on biological, sociodemographic, familial, nutritional, and environmental factors. The response alternatives in the questions were supposed to be mutually exclusive. Questions were formulated using data from pediatric medical records. The initial version of the questionnaire was prepared in English and subsequently translated into Arabic by a qualified professional translator. To ensure linguistic accuracy and conceptual equivalence, the Arabic version was back-translated into English by independent language experts.
Prior to data collection, the questionnaire was reviewed by experts in speech and language disorders, a pediatrician, therapists, and an English language expert to ensure content validity. A pilot study was then conducted with 25 participants (7.8% of the total sample) to assess item clarity, relevance, and feasibility. No major modifications were needed, so these participants were included in the final analysis.
Given that the questionnaire consisted primarily of categorical and independent variables rather than items measuring a single underlying construct, the reliability of the instrument was supported through expert validation and pilot testing.
Data processing and analysis
Data analysis was performed using SPSS version 26 (Version 26.0. Armonk, NY: IBM Corp). Descriptive statistics, including frequencies and percentages, were utilized for categorical data, whilst means and standard deviations were applied to continuous variables. The correlation between speech and language delay and associated factors was evaluated by Chi-square analysis, subsequently followed by logistic regression.
Ethical consideration
The Institutional Review Board (IRB) of An-Najah University granted ethical approval for this work (BioMed. Dec. 2024/63). Official permission was obtained from all participating institutes, schools, kindergartens, and daycare centers prior to data collection. Before participating in the study, all minor participants’ legally authorized representatives (parents or guardians) provided written informed consent; individuals who did not sign the consent form were unable to participate. The consent form delineated the study’s objective and guaranteed anonymous and voluntary involvement, with no penalties for nonparticipation. Prior to inclusion in the study, all individuals provided signed informed consent.
Results
Sociodemographic characteristics of study participants
Sociodemographic features of Palestinian children aged two to ten years were involved in the study.

P-value was obtained using the Chi-square test. P-value < 0.05 was considered significant.
Biological characteristics of study participants
Biological parameters among children aged 2–10 years old who participated in the study.

P-value < 0.05 was considered significant. P-value was obtained using the Chi-square test (*)/fisher’s exact test (^).
Feeding-related features of study subjects
Feeding-related features of study subjects.
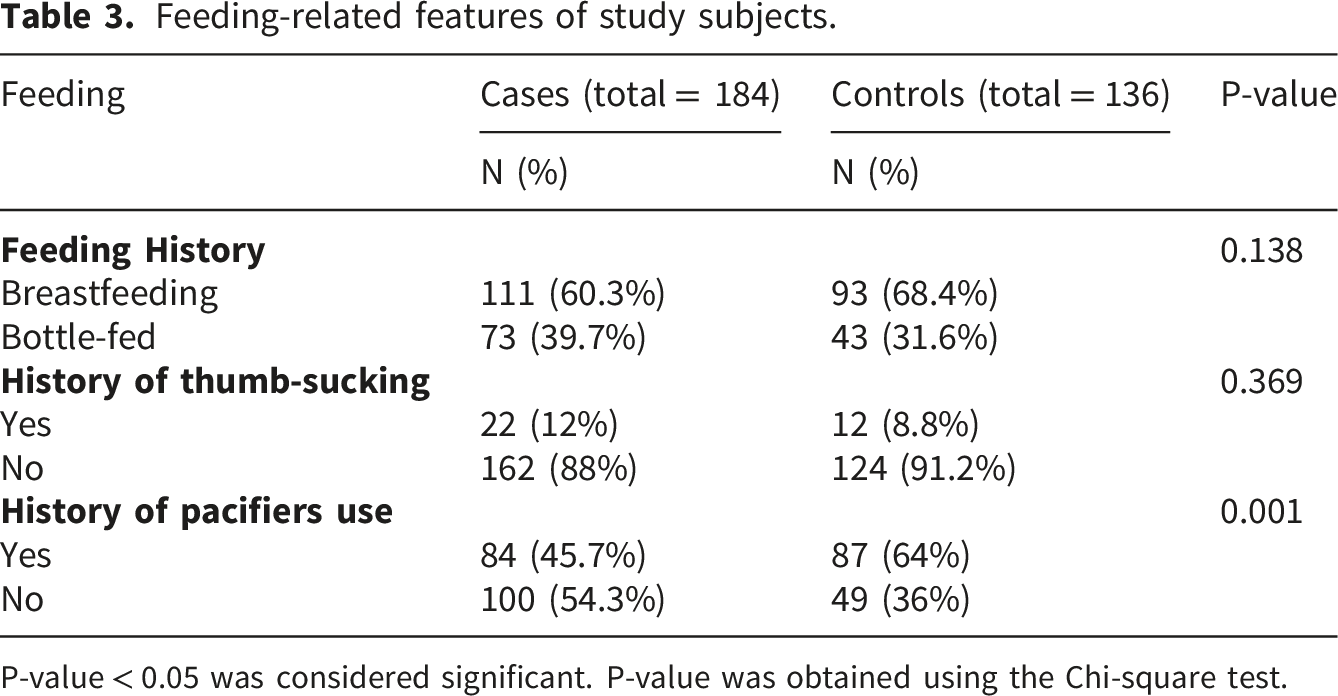
P-value < 0.05 was considered significant. P-value was obtained using the Chi-square test.
Familial characteristics of study subjects
Familial characteristics of study subjects.

P-value was obtained using the Chi-square. P-value < 0.05 was considered significant.
Environmental characteristics of study participants
Environmental characteristics of study participants.

P-value was obtained using the Chi-square test. P-value < 0.05 was considered significant.
Analysis of the associations between SLD and influencing factors of study participants by binary logistic regression
Analysis of the associations between SLD and influencing factors of study participants by binary logistic regression.

P-value was obtained using the multivariate binary logistic regression test. P-value < 0.05 was considered significant.
Maternal employment status was also independently associated with SLD: children of working or self-employed mothers had significantly lower odds (OR = 0.27, p < 0.001, 95% CI: 0.13–0.57) compared to those of housewives. Similarly, household monthly income of 1860–3000 ILS was linked to higher SLD risk, with 2.5 times greater odds than incomes >6000 ILS (OR = 2.5, p = 0.030, 95% CI: 1.09–5.86).
School type emerged as a strong predictor, with children in special schools facing 5.5 times higher odds of SLD than those in regular schools (OR = 5.5, p < 0.001, 95% CI: 2.32–13.05). Other ear, nose, and throat (ENT) problems conferred nearly fourfold increased odds (OR = 4.0, p = 0.012, 95% CI: 1.36–11.38), and family history of speech and language disorders raised odds by 8.6-fold (OR = 8.6, p = 0.001, 95% CI: 2.30–31.82). Results are presented in Table 6.
Discussion
Although substantial research has been conducted on SLD, comprehensive examinations of the contributing factors remain restricted in Palestine. This study sought to identify important associated factors for SLD in Palestinian children aged 2 to 10 years. The age and gender distributions were comparable between cases and controls. This aligns with global epidemiological patterns, where males are consistently overrepresented in SLD cohorts, potentially due to neurobiological and genetic vulnerabilities.32,33 The preponderance of cases in early school years highlights the necessity of early detection and intervention during important developmental periods. 34 Additionally, the finding that cases were seen in the 5–7 age period is suggestive of referral patterns because many students are referred for formal evaluation when they begin lower elementary school, making the challenges more noticeable due to greater social and academic demands.
Several studies have shown that males have a twofold greater risk of SLD, however this study found no statistically significant association between gender and SLD. This gap may indicate cultural, environmental, or sample variables that require additional investigation.35,36 Furthermore, mother-tongue language may play a role in this context; in a study with children (mean age 2 years 9 months) whose rate of language acquisition was attuned to the complexity of their mother tongue, they found that language and, family, but not the child’s gender, accounted for a significant proportion of individual differences in child speech. 37 Furthermore, child-centered audio-recording research of 1,001 children from 12 nations spanning six continents found that child gender did not explain considerable diversity in child speech. 38
Rural residence was significantly associated with SLD. However, this finding should be interpreted with caution, as controls were recruited exclusively from urban schools and daycare centers within the catchment areas of participating institutes, likely underrepresenting rural participants and introducing selection bias that may have inflated the observed association. Future studies should ensure more balanced rural–urban representation in control selection. The observed disparity is also consistent with evidence from low- and middle-income countries, where limited access to early intervention services, specialist healthcare, and educational resources in rural areas contributes to worse developmental outcomes. 39 Rural-urban disparities in developmental outcomes are well-documented, frequently exacerbated by poverty and infrastructural limitations. 40 These places are “concurrently more challenged by limited access to formal child care, affordable housing, living-wage jobs, and social services”. 41
Lower parental education levels and socio-economic status were also strongly linked to SLD. These findings align with evidence that parental education enhances language-rich home environments and cognitive stimulation, which is critical for language acquisition. 42 Lower socio-economic status (SES) and income further compound risks, as economic deprivation limits access to enriching resources and exacerbates familial stress, hindering language development. 43 In contrast, highly educated parents read and interact with their children more regularly, which is proven to increase language development. Thus, our findings coincide with literature suggesting that poor parental education - a sign of limited “language stimulation” at home - is associated with delayed speech in offspring.11,35,44,45 Child socioeconomic status was another strong determinant. Children from lower-income families were much more likely to have SLD in our sample. This is consonant with extensive evidence that poverty impairs language development. For instance, Perkins et al. (2014) note that poverty consistently produces deficits in vocabulary, phonological awareness, and syntax throughout childhood. 46
The father’s occupation did not substantially correlate with SLD, but the overall occupational profile of both parents did. This could indicate that parental jobs function as indicators for family income, social class, and available time for kid engagement. Parents with demanding or restrictive occupations may have less time for one-on-one speech interactions with their kids. White-collar or professional occupations, on the other hand, are frequently associated with better socioeconomic status and education, both of which we have previously found to be protective. In the literature, parental occupation is less commonly researched than education, although it is conceptually interwoven with socioeconomic issues. 11
Family size and number of siblings showed no significant association with SLD, consistent with some prior studies. Some studies have found that larger families dilute parental attention, increasing the likelihood of delays. Karbasi et al., for example, found that a large family size was a substantial risk factor for speech delay. 47 However, in agreement with Kanhere et al., we did not observe such an effect: in our sample, having multiple siblings neither protected against nor exacerbated SLD risk. 45 Siblings may also provide language input (older siblings may converse with younger siblings), and larger families may benefit from family support networks to buffer delays.
A novel aspect of this study was the finding that educational environment -both the type of school attended and the school’s perceived role in speech development-was significantly associated with SLD. This indicates that school-related factors influence speech outcomes. Although causality cannot be inferred, it is plausible that children enrolled in special or language-focused programs are most likely to be enrolled in special schools as the normal governmental school in Palestine does not offer (in majority) special needs classes.
The observed association between SLD and a history of serious injury, illness, or hospitalization aligns with prior research linking early medical adversity to neurodevelopmental disruptions. 48 Such events may impair cognitive development through mechanisms such as prolonged stress, inflammation, or missed educational opportunities during critical learning periods. 49 One well-established cause of speech delay is hearing loss. However, there are a number of complex factors that contribute to speech-language delays, including the child’s environment and biological development.50,51
A striking positive family history was observed among SLD cases, compared to controls. This is consistent with a positive family history of speech-reading difficulties (dyslexia, delayed speech, unclear speech, stuttering, and limited vocabulary), which has been linked to speech and language delay in first-degree relatives.35,52 Furthermore, it is consistent with the current understanding of the genetic and familial components of language development. Several studies have shown the importance of genetic predispositions in impacting speech and language difficulties, with heritable factors frequently contributing to delays in speech acquisition.53–55 Finally, multilingualism was less common among SLD cases, contradicting assumptions that multilingualism inherently delays language acquisition. 56 Rather, this may reflect that multilingual households tend to have higher education levels, offering enriched linguistic environments and structured language input.
The limitations that must be acknowledged when analyzing the results. The case–control design restricts the capacity to ascertain causal links between the identified risk factors and SLD. Secondly, selection bias may have occurred, as cases were sourced from specialized institutions predominantly situated in urban areas, whereas controls were obtained from schools and daycare centers, thus resulting in an underrepresentation of rural participants in the control group. This disparity, especially regarding residence, may have affected the observed correlations. Third, data collection was partially dependent on self-reports from parents or caregivers, which may be prone to recall bias or mistakes, particularly with history or behavioral characteristics. Fourth, despite attempts to incorporate a comprehensive array of socio-demographic, biological, and environmental factors, several potentially pertinent variables—such as the quality of parent–child connection, specific linguistic exposure, and the severity of SLD—were not evaluated. Moreover, this study included a broad age range (2–10 years), which may introduce developmental heterogeneity, as language abilities and clinical characteristics vary across age groups. Although all cases were previously diagnosed by specialists and age was considered in the analysis, residual confounding related to developmental stage cannot be fully excluded. Future studies may benefit from age-stratified analyses. The employment of a structured questionnaire featuring primarily categorical variables may constrain the analytical depth and hinder the capture of subtle differences in exposure. The study was conducted in a specific cultural and geographic context (Palestine), perhaps restricting the generalizability of the findings to other groups. Nevertheless, despite these constraints, the substantial sample size and incorporation of several contributing factors yield significant insights on SLD in this little-explored context.
Conclusion
The study provides novel insights into the factors contributing to speech and language delay in Palestinian children, being one of the first assessments of SLD determinants within a Palestinian clinical population, hence contributing original data to the field. Highlighting the significance of social and regional disparities. The results emphasize the necessity of improved early screening and equitable access to intervention programs, especially in marginalized groups. The strong correlation with familial history indicates potential genetic influences. These findings emphasize the necessity of integrating early developmental surveillance into healthcare systems and implementing tailored therapies.
Supplemental material
Supplemental material - Children with speech and language delay aged 2–10 Years in Palestine: A case-control study of socio-demographic, biological, familial, and environmental factors
Supplemental material for Children with speech and language delay aged 2–10 Years in Palestine: A case-control study of socio-demographic, biological, familial, and environmental factors by Sa’ad Al-Lahham, Raghad Dweikat, Tala Nazzal, Nada Abo Shama, Aya Bishara, Nabaa Khaskia, Maimana Jbara, Adan Haj Yahia, Mustafa Ghanim, Majdi Dwikat, Mohammad Abuawad, Samar Alkhaldi, Anas Hamdan, Wafa Abdel Jalil, Laith El-lahham, Maha Rabayaa, Malik Alqub in Sage Open Medicine.
Footnotes
Acknowledgments
We are grateful to everyone who gave their time to make this initiative a reality. Similarly, we appreciate the partnership with the An-Najah National University faculty of medicine and allied medical sciences and the department of audiology and speech pathology.
Ethical considerations
The Institutional Review Board (IRB) of An-Najah University granted ethical approval for this work (BioMed. Dec. 2024/63). Official permission was obtained from all participating institutes, schools, kindergartens, and daycare centers prior to data collection. Before participating in the study, all minor participants’ legally authorized representatives (parents or guardians) provided written informed consent; individuals who did not sign the consent form were unable to participate. The consent form delineated the study’s objective and guaranteed anonymous and voluntary involvement, with no penalties for nonparticipation. Prior to inclusion in the study, all individuals provided signed informed consent.
Consent for publication
The authors grant permission to the publishers to publish the work.
Author contributions
SAL and MA: Conceptualization, methodology, investigation, formal analysis, writing – review & editing. RD, TN, AH, and MR: Formal analysis, and writing – review & editing. NAS, AB, NK, MJ, AHY, WAJ, and LEL: Methodology, and writing – original draft preparation. MG, MD, MA, and SA: Methodology, investigation, formal analysis, and writing – original draft preparation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.