
Abstract
Objective. To characterize early risk factors of moderate/severe hepatotoxicity in a pediatric population with acetaminophen overdose, due to suicide attempt, admitted to a general secondary-level pediatric department. Methods. A retrospective case study of 107 patients, 11 to 15 years old. Results. There was a highly significant relationship between the number of episodes of prehospital vomiting and several elevated hepatologically relevant biochemical parameters, for example, maximum aspartate aminotransferase (P = .0001). The duration of the latency time before initiation of N-acetylcysteine treatment was significantly related to the elevation of several hepatologically relevant biochemical parameters (eg, maximum γ-glutamyl transferase; P = .0001). Patients suffering from illness prior to their suicide attempt had significantly greater elevations of their hepatologically relevant biochemical parameters, for example, maximum alanine aminotransferase (P = .01) levels than healthy patients. Conclusion. By use of risk factors, it is possible to identify pediatric patients at increased risk of moderate/severe hepatotoxicity at an early stage of admission.
Introduction
Acetaminophen (paracetamol) is a widely used and readily available analgesic that has the potential to cause serious liver injury when taken in overdose. 1 It is the drug of choice in suicidal attempts in Western societies. In Denmark, more than 275 of 100 000 children aged 10 to 15 years are admitted to hospitals each year because of suicide attempts, primarily by means of acetaminophen. 2 Thus, hepatotoxicity and potential liver failure caused by acetaminophen in childhood and adolescence is a dominant problem. Children who overdose on acetaminophen typically have a good prognosis even if severe hepatotoxicity has developed—few are referred to a tertiary specialized pediatric department, and the majority of pediatric patients are discharged from a general secondary-level pediatric department with intact liver function. 3 An age-associated difference in the conjugation of acetaminophen metabolites may explain the lower morbidity among pediatric patients compared with suicide attempts by adult patients.4-6 Moreover, children have a larger hepatic cell mass and greater capacity for hepatic regeneration. 7
When consumed in therapeutic doses, acetaminophen is metabolized by the liver through 2 pathways (Figure 1). Specifically, 90% of the drug is conjugated with glucuronic acid or sulfates, yielding nontoxic conjugates that are excreted by the kidneys. Approximately 5% is metabolized into the reactive intermediate N-acetyl-p-benzoquinone imine (NAPQI), by the cytochrome P450 system 8 (if gluthathione stores are intact). When acetaminophen is ingested in excessive doses, the gluthathione stores are depleted, and the highly reactive toxic metabolite, NAPQI, is produced in excessive amounts. N-acetylcysteine (NAC) acts as an antidote to acetaminophen toxicity by enhancing the glutathione stores, providing glutathione substitution and enhancing disposition by nontoxic sulfate conjugation. 9
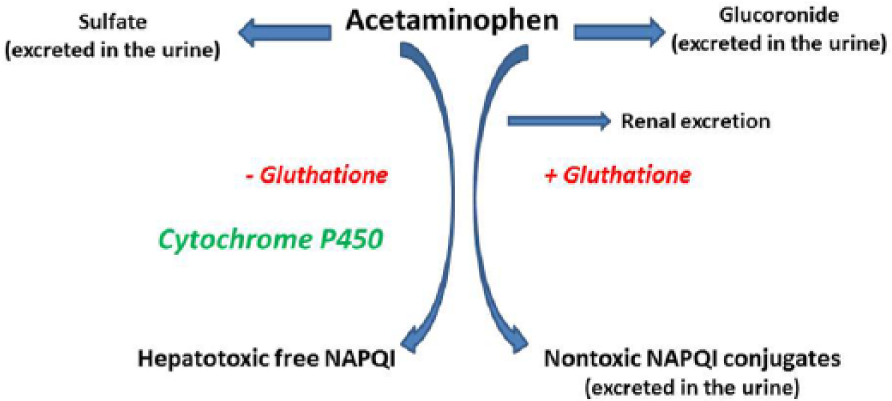
The conjugation of acetaminophen by glutathione and cytochrome P450.
Studies in adults have shown that acetaminophen-poisoned patients with a high frequency of vomiting tended to have a worse liver outcome than patients with a low frequency of vomiting. 10 Furthermore, several studies in adult patients have demonstrated the importance of early initiation of NAC treatment in cases of acetaminophen overdose.11,12 Finally, a recent animal study has shown that concomitant viral infections or fasting could potentially aggravate the hepatic toxic effects. 13 One pediatric study from 1995 also discussed whether a viral infection could lower the threshold for hepatotoxicity.14,15
In our opinion, none of the above-mentioned possible early risk factors of hepatotoxicity have been thoroughly studied in a pediatric population. The general purpose of the present study was, therefore, to identify early risk factors of hepatotoxicity in pediatric patients admitted to a general secondary-level pediatric department after the ingestion of an acetaminophen overdose as a part of a suicide attempt. We focused on the following possible early risk factors: prehospital vomiting, in-hospital vomiting, the latency time before NAC treatment, and illness prior to the suicide attempt. We have chosen to focus on patients admitted to a general secondary-level department, since the majority of patients are admitted, treated, and discharged from such departments. It is of outmost importance that clinicians know about and are aware of early risk factors of acetaminophen-induced moderate/severe hepatotoxicity that pediatric patients may exhibit during hospitalization at a general secondary-level pediatric department—in order to secure urgent specialized care for these patients.
There are, to the best of our knowledge, no similar reports on this issue in a pediatric population.
We have previously published a study of possible early risk factors of severe hepatotoxicity in a population admitted to a specialized tertiary pediatric department due to suicide attempt with acetaminophen. 16
We also previously published a study of the social pediatric characteristics, trends, and risk factors in the same group of patients. 17
Methods
Overview
This retrospective study was performed on 11- to 15-year-old patients admitted to the Department of Pediatrics and Adolescent Medicine, Nordsjællands Hospital, Denmark, because of suicide attempts with acetaminophen, during the period from January 2006 to July 2011. A computer search of ICD10 diagnoses at discharge (DT39, DT390, DT398, and DT398A) identified the relevant medical records.
All data were collected from medical records, including standard questions concerning acetaminophen intake, number of episodes of vomiting, time of intake, and so on.
At the time of this study, the Danish NAC regime was weight-guided, with a minimum duration of 36 hours, if the estimated intake was greater than 125 mg/kg 18 —without respect to the ingested dose, symptoms, or postabsorptive s-acetaminophen levels. Truncated periods of treatment were based on repeated evaluations of the coagulation status (international normalized ratio [INR]) and the levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST).
Inclusion Criteria
Children, aged 10 to 15 years, admitted to the Department of Pediatrics and Adolescent Medicine, Nordsjællands Hospital, Denmark, because of suicide attempt by means of acetaminophen were included. The patients were only included if they had answered all the standard questions. We only included those patients whose parents, at time of admission, were able to confirm the ingested dose of acetaminophen.
Exclusion Criteria
Patients with known liver disease prior to their suicide attempt were excluded. Patients taking medication that enhance the induction of the cytochrome P450 system, increase the production of toxic metabolites, or aggravate the hepatotoxicity, such as ethanol, rifampin, isoniazid, barbiturates, and carbamazepine, were excluded.
If a patient had several suicide attempts during this time period, only the first suicide attempt was included.
During the study period, 177 patients fulfilling the inclusion criteria were identified. Of these, 70 patients were excluded because of insufficient medical records (n = 24), insufficient biochemical parameter data (n = 30), or because of suicide attempts using agents other than acetaminophen (n = 16). A total of 107 patients were included in the final analysis.
To assess the prevalence of episodes of pre- and in-hospital vomiting, 4 categories that were based on the number of vomiting episodes were defined: 0, no vomiting; 1, one episode of vomiting; 2, two episodes of vomiting; and 3, three or more episodes of vomiting. If the patient or the parents were in any doubt about the number of episodes of prehospital vomiting, we registered “no episodes of prehospital vomiting” to eliminate any overestimation.
The initial and maximum levels of the following biochemical parameters were registered from the electronic biochemistry files of each patient: γ-glutamyl transferase (GGT), basic phosphatase (BP), INR, ALT, AST, and s-acetaminophen.
Illness prior to the suicide attempt was defined as any type of illness up to 48 hours prior to the suicide attempt, including flu, colds, gastroenteritis, and tonsillitis. Because of the limited number of ill patients, they could not be subcategorized based on the different types of illness.
Because of limited space, only significant results are shown in the tables.
We have excluded one single outlier in Figures 2 and 4 to increase the legibility.

Episodes of prehospital vomiting versus maximum ALT, maximum AST, maximum GGT, and maximum INR.

Latency time before initiation of NAC treatment versus maximum ALT, maximum AST, maximum GGT, and maximum INR.
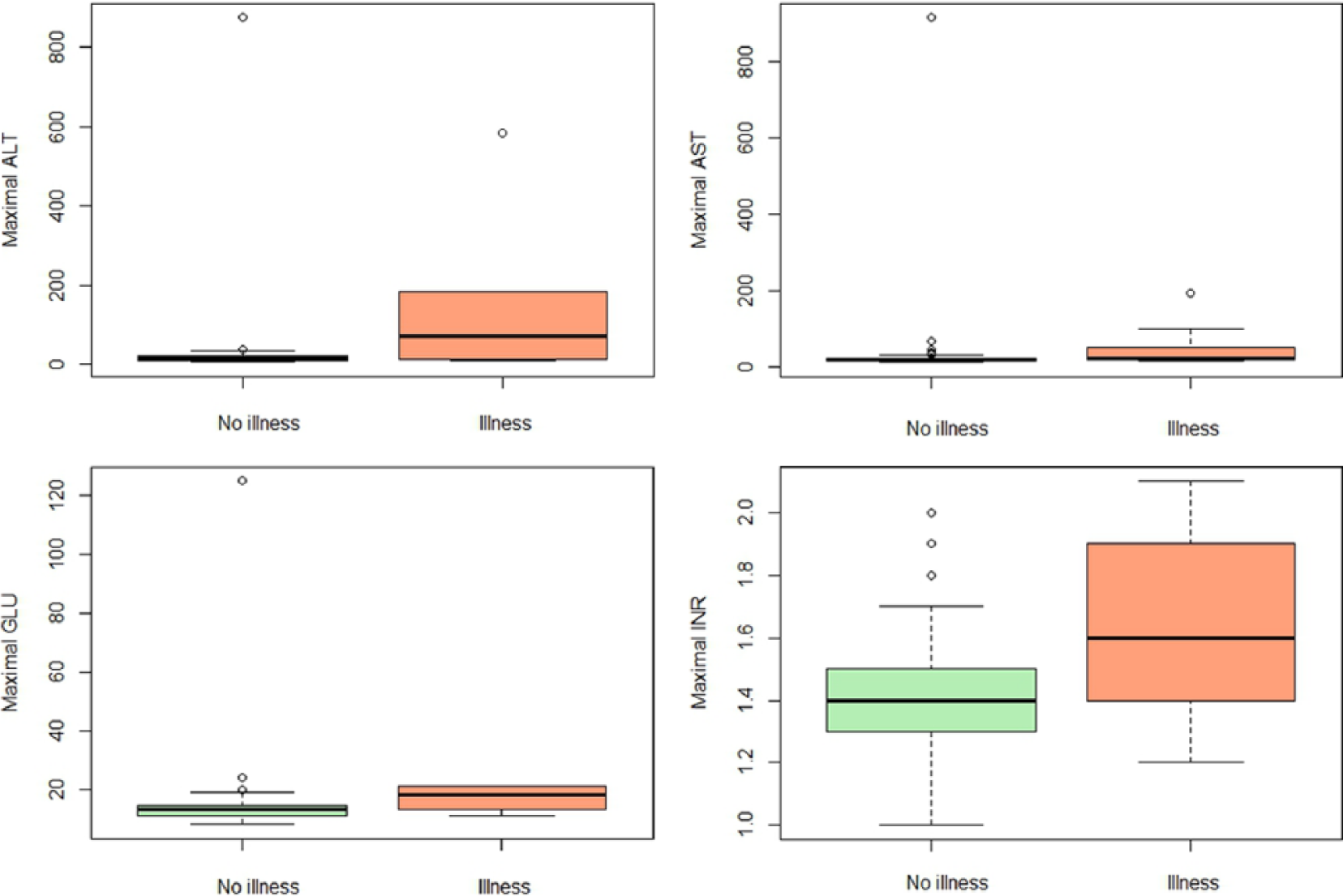
Illness/absence of illness prior to the suicide attempt versus maximum ALT, maximum AST, maximum GGT, and maximum INR.
Statistical Analysis
Linear regression analyses were used to quantify the strength of the relationship between continuous outcomes (responses) and continuous risk factors, and categorical risk factors, to assess which levels of the categorical risk factors had significant/insignificant effects on the outcomes. To obtain a better fit, natural logarithm transformation was used to transform the responses. All unstandardized coefficients from these models were back-transformed to the natural scale. The back-transformed differences between levels of categorical variables are given as relative ratios. Furthermore, the statistical relationship between binary outcomes and explanatory variables was assessed by using logistic regression. All models were statistically tested with α = 5%. The analyses were performed using SAS 9.2 and R i386 2.15.2 software programs.
Results
Of the 107 patients included in the study, 7.5% were boys (n = 8) and 92.5% were girls (n = 99). The mean age was 13.5 years (range = 11-15 years). In total, 95% received charcoal treatment (n = 101), and 99% received NAC treatment (n = 106).
Of the 107 admitted patients, 104 patients with mild/moderate hepatotoxicity were discharged with improved liver function from a general secondary-level department. Three patients with severe hepatotoxicity were referred to a tertiary pediatric department, specialized in children’s liver diseases, all with INR >1.5 and elevated transaminase levels. None of the patients required transplantation.
Acetaminophen Intake
All the medical records included self-reported information on the dose intake. The mean intake of acetaminophen was 10.4 g (range = 2.5-45 g)/0.20 g/kg (range = 0.02-0.9 g/kg). There was no difference between genders (P = .1). Seven patients also consumed ibuprofen (0.6-14.8 g); on its own, ibuprofen had no influence on the outcomes. There was a significant relationship between acetaminophen intake (g or g/kg) and the following hepatologically relevant biochemical parameters: INR initial (P = .0310), INR max (P = .0037), and AST max (P = .0360; Table 1). When comparing the acetaminophen (g or g/kg) intake and biochemical parameters, adjusting for time before initiation of NAC treatment, none of the relationships remained significant.
Acetaminophen Intake Versus Hepatologically Relevant Biochemical Parameters.

Abbreviations: CI, confidence interval; INR, international normalized ratio; AST, aspartate aminotransferase.
Each unit increase in acetaminophen increases the biochemical parameter by the given estimate (the estimate indicates the slope of the linear model).
Prehospital Vomiting
There was an incidence of prehospital vomiting of 26.2% in the population—12.2% only experienced 1 or 2 episodes of prehospital vomiting, and 14% experienced 3 or more episodes of prehospital vomiting. There was a significant relationship between the number of episodes of prehospital vomiting and the total acetaminophen intake, and for each unit acetaminophen intake increase, the odds of prehospital vomiting was increased by a factor of 1.13 (95% confidence interval [CI] = 1.04-1.22; P = .0036). Bodyweight (body volume of distribution) had no influence on the number of episodes of prehospital vomiting.
Several highly significant relationships were found between the number of prehospital vomiting episodes and the following relevant biochemical parameters: GGT initial (P = .006), GGT max (P = .002), INR max (P = .0190), AST initial (P = .0001), AST max (P < .0001), and ALT max (P = .0014; see Table 2 and Figure 2).
Episodes of Prehospital Vomiting Versus Hepatologically Relevant Biochemical Parameters.

Abbreviations: CI, confidence interval; GGT, γ-glutamyl transferase; INR, international normalized ratio; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
The unstandardized coefficients are the back-transformed unstandardized coefficients from the linear regression model with the response log (biochemical parameter). The difference between groups ≥3 and 0 indicates the relationship between the back-transformed coefficients for (group ≥3/group 0), that is, the relative ratio of the 2 groups.
There was no significant relationship between the number of episodes of prehospital vomiting and the latency time before initiation of NAC treatment.
In-Hospital Vomiting
There was an incidence of in-hospital vomiting episodes of 40.2% in the population—15% only experienced 1 or 2 episodes of prehospital vomiting, and 25.2% experienced 3 or more episodes of prehospital vomiting. There was a significant relationship between the number of in-hospital vomiting episodes and the following hepatologically relevant biochemical parameters: INR max (P = .0122), AST max (P = .0144), ALT max (P = .0072), and s-acetaminophen (P = .0055; Table 3).
Episodes of In-Hospital Vomiting Versus Hepatologically Relevant Biochemical Parameters.
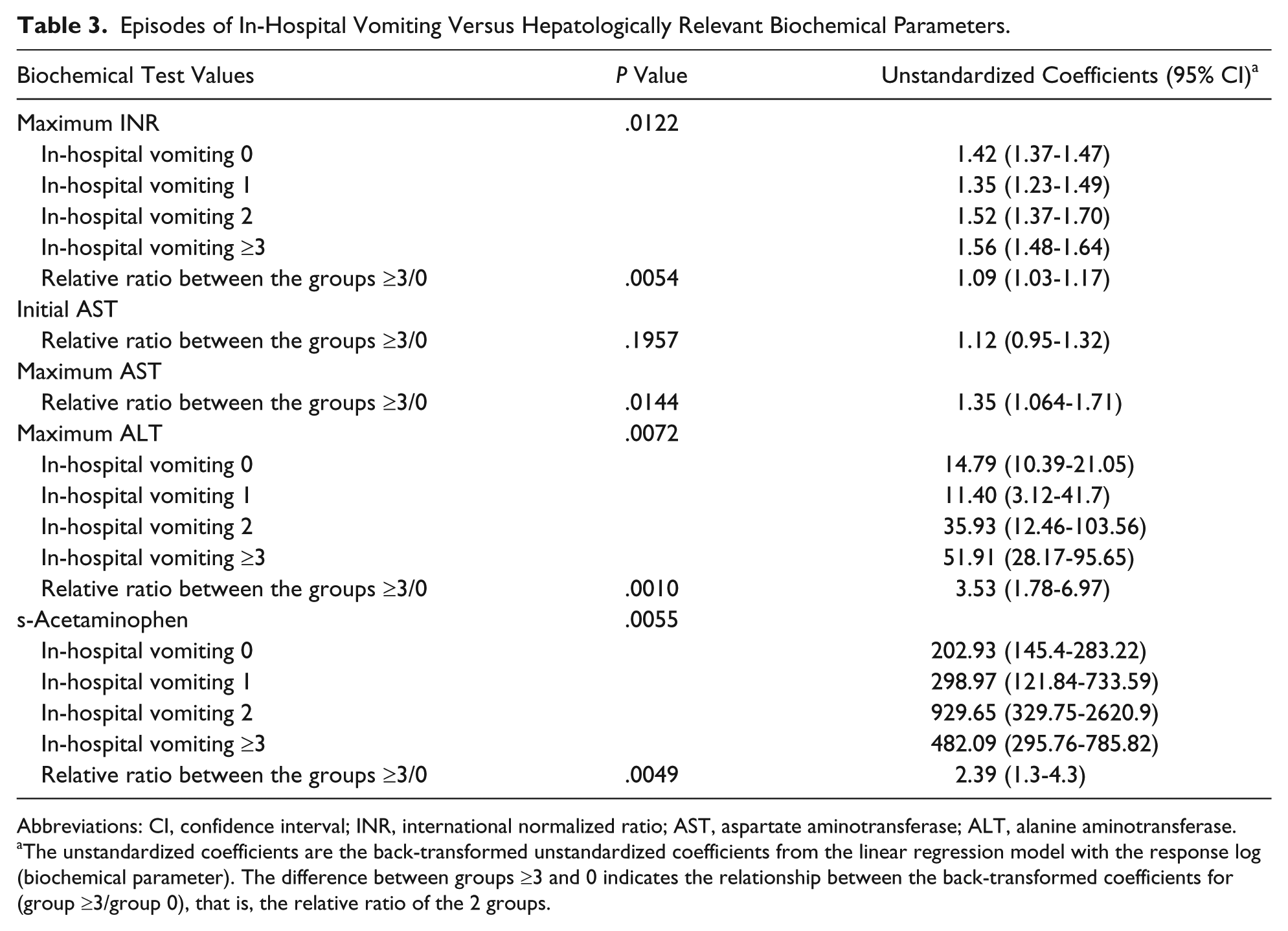
Abbreviations: CI, confidence interval; INR, international normalized ratio; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
The unstandardized coefficients are the back-transformed unstandardized coefficients from the linear regression model with the response log (biochemical parameter). The difference between groups ≥3 and 0 indicates the relationship between the back-transformed coefficients for (group ≥3/group 0), that is, the relative ratio of the 2 groups.
There was also a significant relationship between the number of in-hospital vomiting episodes and acetaminophen intake; for each unit acetaminophen intake increase the odds of in-hospital vomiting increased by a factor of 1.07 (95% CI = 1.01-1.15; P = .03). Bodyweight (body-volume of distribution) had no influence on the number of episodes of in-hospital vomiting.
Latency Time Before Initiation of NAC Treatment
The majority of the patients (70%) were admitted within the first 6 hours after acetaminophen intake (n = 74). There were highly significant relationships between the latency time before initiation of NAC treatment and the following hepatologically relevant biochemical parameters: GGT max (P < .001), INR max (P = .001), AST initial (P = .001), AST max (P < .00001), ALT initial (P = .0009), and ALT max (P = .0021; see Table 4 and Figure 3).
Latency Time Before Initiation of NAC Treatment Versus Hepatologically Relevant Biochemical Parameters.

Abbreviations: NAC, N-acetylcysteine; CI, confidence interval; GGT, γ-glutamyl transferase; INR, international normalized ratio; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
The unstandardized coefficients are the back-transformed unstandardized coefficients from the linear regression model with the response log (biochemical parameter).
Illness/No Illness Prior to the Suicide Attempts
Overall, 10% of the patients reported illness up to 48 hours prior to their suicide attempts (n = 11). There was no difference in the mean intake between the 2 groups, which was 10.01 g in the group with no illness prior to intake and 11.29 g in the group with illness prior to intake. There were significant relationships between illness prior to acetaminophen intake and the following biochemical parameters: INR initial (P = .0453), INR max (P = .0130), AST max (P = .0154), and ALT max (P = .0122; see Table 5 and Figure 4).
Illness Prior to the Suicide Attempt Versus Hepatologically Relevant Biochemical Parameters.

Abbreviations: CI, confidence interval; INR, international normalized ratio; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
The unstandardized coefficients are the back-transformed unstandardized coefficients from the linear regression model with the response log (biochemical parameter). The difference between groups ≥3 and 0 indicates the relationship between the back-transformed coefficients for (group ≥3/group 0), that is, the relative ratio of the 2 groups.
Discussion
The present study shows that it is possible, at an early stage of admission, to predict subsequently elevated levels of, for example, transaminases, INR, and other hepatologically relevant biochemical parameters. We found that especially episodes of prehospital vomiting, but also episodes of in-hospital vomiting, latency time before initiation of NAC treatment, and illness prior to a suicide attempt, by means of acetaminophen, could be important early clinical risk factors of underlying evolving moderate/severe hepatotoxicity in a pediatric population.
James et al found that the best low-risk predictors of acetaminophen-induced hepatotoxicity were normal values of prothrombin, AST, and ALT within 48 hours of ingestion. 19 They conclude that all patients with acetaminophen poisoning should be observed for 48 hours to identify possible hepatotoxicity. We believe that our results demonstrate the identification of several parameters that significantly were able to predict moderate/severe hepatotoxicity at an earlier stage of admission. It is of major importance that clinicians at general secondary-level pediatric departments know and are aware of the early risk factors of hepatotoxicity, in order to secure optimal monitoring and referral of these patients to a specialized tertiary pediatric department. We have focused our study on patients admitted to a general secondary-level department, since the majority of patients are admitted, treated, and discharged from such departments.
In our pediatric study, unlike several adult studies,7,20 there was only a sparse relationship between the hepatologically relevant biochemical parameters and the ingested amount of acetaminophen overdose. This finding is in accordance with the results of the studies by Mahadevan et al 21 and James et al, 19 who found no relationship between the median dose ingested and the severity of the subsequent liver outcome. In a study of 25 pediatric patients with severe hepatotoxicity admitted to a tertiary specialized department, we found no relationship between any of the biochemical parameters and the ingested amount of acetaminophen. 16
Our results show that an increased number of prehospital vomiting episodes after an acetaminophen overdose in a pediatric population that attempted suicide is an important early clinical risk factor that indicates that pediatric patients, who have been vomiting intensively, should be observed more carefully. We found a highly significant relationship between the number of episodes of prehospital vomiting and the hepatologically relevant biochemical parameters; the number of prehospital vomiting episodes increased as the biochemical parameters became increasingly affected. In contrast, we did not find a similar significant relationship between the amount of acetaminophen ingested and the hepatologically relevant biochemical parameters. In a study of pediatric patients with severe hepatotoxicity due to acetaminophen poisoning, we likewise found similar highly significant relationships between the number of episodes of prehospital vomiting and the relevant biochemical parameters. 16 We assume that a possible explanation of the lack of linear dose–response relationship could be that patients who develop severe hepatotoxicity or liver failure may have a different expression of cytochrome P450 than the age-adjusted background population, which results in higher levels of the hepatotoxic-free NAPQI compound at lower acetaminophen doses. Polymorphisms in genes encoding the acetaminophen glucuronosyltransferase enzymes have also recently been found in adults and have been related to the risk of acetaminophen-induced liver injury. 22 Because the expression of cytochrome P450 in pediatric populations has not yet been established, the age-adjusted activities in a pediatric population are not understood as well as those in adults. The disparity in morbidity between an adult and a pediatric population could be explained by an age-associated difference in the conjugation of acetaminophen metabolites.4-6 Moreover, children have a larger hepatic cell mass and a greater capacity for hepatic regeneration. 7 None of our patients were candidates for liver transplantation, and only 3 patients required referral to a tertiary pediatric department specialized in children’s liver diseases.
Rumack and Rosen 23 previously reported that the incidence of vomiting in an adult population was 33.3%. Additionally, Clark et al 24 found that the prevalence of vomiting was 12.5% in all adult patients, whereas Zyoud et al 10 found the prevalence to be 65%. These differences in the prevalence of vomiting are likely due to different registration methods, study populations, treatment protocols, amounts of intake, and latency time before NAC treatment. None of the studies distinguished prehospital vomiting from in-hospital vomiting, and most did not differentiate among the number of vomiting episodes.
In accordance with our findings, Zyoud et al found that patients with a high frequency of vomiting tended to have more affected hepatologically relevant biochemical parameters than patients with a low frequency of vomiting. 10 However, in their study, only 64% of the study population received NAC treatment compared with 99% in our study population. Furthermore, they did not distinguish between pre- and in-hospital vomiting. Thus, episodes of in-hospital vomiting that were due to the charcoal treatment were also included. In our study population, 39.5% experienced in-hospital vomiting, possibly partly due to the charcoal treatment. The degree of in-hospital vomiting was significantly related to several of the relevant biochemical parameters, although the P values were higher than those associated with prehospital vomiting. The identification of patients who experience episodes of in-hospital vomiting due to an underlying evolving hepatotoxicity and perhaps a possible distinct configuration of the cytochrome P450 genes is difficult, because many patients vomit due to the emetogenic effect of the charcoal treatment. Thus, prehospital vomiting appears to be a much more valid clinical predictor than in-hospital vomiting.
Current pediatric NAC regimes are based on studies of adults, and the importance of early initiation of NAC-treatment in case of acetaminophen overdose has been proved in several adult studies.11,12 Our study results confirmed these finding in a pediatric population. There was a highly significant relationship between the different hepatologically relevant biochemical parameters and the latency time before initiation of NAC treatment, which is in line with the general concept that NAC treatment should be initiated as early as possible in all patients who have had an acetaminophen overdose.9,25 In Denmark, the gold standard for treating acetaminophen overdose is weight-adjusted charcoal treatment followed by intravenous antidotal NAC. Several other countries use an oral NAC treatment and the Rumack-Matthews nomogram (eg, the United States), which, unfortunately, makes it complicated to compare data and effects of the different regimens.
Overall, 10% of our study population reported illness in up to 48 hours before their suicide attempt. The patients with illness prior to their suicide attempt had significantly more affected transaminases and INR than the group without illness prior to their suicide attempt, even though they had ingested similar amounts of acetaminophen. Whether a viral infection or possible ingestions of therapeutic doses of acetaminophen on their own, or perhaps synergistically, lower the threshold for hepatotoxicity remains unclear.14,15 A recent animal study has shown that concomitant viral infections or fasting could potentially aggravate the hepatic toxically effects. 13 We assume that patients suffering from illness may have consumed acetaminophen in therapeutic doses, which could have reduced their glutathione levels or marginally elevated their liver enzymes, leaving the patient more vulnerable to an overdose of acetaminophen. There may possibly be a synergistic effect between the number of days with acetaminophen being used at therapeutic doses resulting in depleted glutathione levels and a subsequent acetaminophen overdose. This possible relationship could not be established in the present study due to its retrospective design but is a part of a large prospective study that was initiated in 2012.
Conclusion
In conclusion, we found a highly significant relationship between the degree of prehospital vomiting and elevated hepatologically relevant biochemical parameters. In contrast, there was only a sparse relationship between acetaminophen intake and these biochemical parameters. Our findings indicate that the number of episodes of prehospital vomiting is a much more sensitive risk factor of moderate/severe hepatotoxicity than the amount of acetaminophen ingested. The latency time before the initiation of NAC treatment was significantly related to higher transaminase levels and lower coagulation levels, as observed in studies of adults. Patients suffering from illness prior to their suicide attempt had significantly more affected hepatologically relevant biochemical parameters than did patients not suffering from illness prior to their suicide attempt.
To the best of our knowledge, this study is the first to describe these potential early risk factors of moderate/severe hepatotoxicity in a pediatric population. These clinical and biochemical risk factors may enable the optimization of treatment, thereby reducing the number of pediatric patients with hepatic sequelae.
Future large longitudinal studies are needed to validate the early risk factors of hepatotoxicity and establish the risk factors found in our study, including studies of pediatric patients with fulminant liver failure. Such a study is part of The Danish Pediatric Acetaminophen Database, which began in 2012.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support from Nordsjællands Hospital.