
Abstract
Objective
The neurological causes of suicide remain poorly understood. This study sought to ascertain whether there is a correlation between amygdala volume and suicidal behavior.
Methods
This case–control retrospective study included 193 participants—108 healthy controls and 85 individuals with a history of suicide attempts. Sagittal magnetic resonance imaging was conducted for each participant, and cross-sectional areas of the left and right amygdala were determined independently using freehand tracing. The total volume of the amygdala was determined by multiplying the thickness of the slices by the sum of the regions.
Results
Patients with a history of suicide attempts had significantly decreased amygdala volumes on both the right (p = 0.018) and left (p = 0.036) sides compared with controls. Receiver operating characteristic analysis determined a cutoff value of 1825 mm³ for both hemispheres. The cutoff sensitivity and specificity for the right amygdala were 30.6% and 88%, whereas the values for the left amygdala were 31.8% and 84.3%, respectively.
Conclusions
This is the first study to show that individuals who had attempted suicide had considerably decreased left and right amygdala volumes, with receiver operating characteristic analysis indicating good specificity (84.3%–88%). According to these findings, a reduced amygdala volume might be a useful biomarker for identifying those who are at risk of attempting suicide.
Keywords
Introduction
One of the main causes of death worldwide is suicide, which is the deliberate taking of one’s own life. 1 Over 700,000 people worldwide lose their lives to suicide each year, and a higher number of individuals attempt suicide, making it a serious public health concern. 2 Suicide attempts, even when they are not deadly, can cause serious harm and place a significant financial burden on healthcare systems.3–5
Suicide risk has been linked to a number of factors, including substance abuse, major depressive disorder (MDD), schizophrenia, other serious mental illnesses, and the use of psychotropic medications.6–11 However, rather than being the result of an externally imposed aim, many suicide attempts seem to be the result of self-directed activity that has the potential to be fatal. 12 Therefore, determining the underlying mechanisms that can enable preventive interventions is becoming increasingly important. 13
Currently available suicide prevention strategies primarily rely on the identification and evaluation of suicidal thoughts and behaviors. However, adequate research has not been conducted on the role of any organic etiology.14,15
Researchers may explore the anatomical causes of mental illnesses owing to recent developments in neuroimaging.16,17 Individuals with suicidal behavior and related disorders have been found to exhibit both structural and functional abnormalities in limbic system components.18,19 The dentate gyrus, amygdaloidal complex, septal area, hypothalamus, and fornix are among the interrelated structures that constitute the limbic system. 20 These structures work together to control instinctual behaviors, aggression, impulsivity, emotion, cognition, and action. 21
In this system, the amygdala is particularly important, which regulates social cognition, emotional memory, fear conditioning, anxiety, and aggression. Individuals who have attempted suicide in the past have less gray matter density in the orbitofrontal 22 and superior temporal cortices than individuals who have not, according to Aguilar et al. 23 Recent studies have revealed that people with a history of suicide attempts had higher resting-state functional activity in the amygdala than healthy controls, particularly showing increased functional connectivity in the right amygdala–bilateral paracentral lobule/precuneus circuit. Moreover, stress exposure may have an impact on amygdala volume.24,25
The amygdala plays a crucial role in functions such as emotional regulation, threat perception, and stress response, and it is frequently subject to structural and functional changes in mood disorders. 22 We intended to determine if there were any notable differences in amygdala volume between those with a history of suicide attempts and healthy people, as these mental illnesses are intimately linked to suicidal conduct. 26 After identifying these amygdala structural variations, we may be able to develop more effective prevention strategies that can save lives. 26 Despite these above findings, there are only a few thorough studies that explicitly examine the connection between amygdala volume and suicidal behavior, which leaves the underlying mechanisms mainly unknown. The purpose of this study was to use sagittal magnetic resonance imaging (MRI) evaluations to ascertain whether individuals who had attempted suicide showed volumetric changes in the amygdala region compared with healthy controls.
Materials and methods
Study design and participants
The study was approved by the Non-Invasive Local Ethics Committee of Firat University with reference number 2023/04-37 (Meeting Date: 09.03.2023). This case–control retrospective study adhered to the moral standards set forth in the latest version (2024 revision) of the Declaration of Helsinki. The reporting of this study conforms to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines. 27
A total of 110 patients, aged 18–55 years, who attempted suicide were referred for psychiatric consultation after presenting to the Elaziğ Fethi Sekin City Hospital between June 2023 and May 2025. The brain MRI results of these patients were examined. Brain MRI results of people who visited the hospital for nonsuicidal reasons over the same period were also analyzed as a control group. Each participant in this study was chosen at random.
Individuals who had a history of intracranial surgery, cranial trauma, aberrant intracranial masses, comorbidities, and substance use or technical flaws on their MRI were excluded from the study. Eighty-five patients were still eligible for the suicide attempt group after applying these exclusion criteria. For comparison, 108 age- and sex-matched healthy controls were chosen.
Patient records provided demographic information such as age and sex. To guarantee that no person could be identified in any manner, all data were completely deidentified. As this retrospective study was conducted using previously collected imaging data, no direct patient contact occurred, and signed informed consent was not obtained, as it was not required according to our institutional review board guidelines. A Philips Prodiva 1.5T CX MRI scanner was used for imaging. Coronal T2-weighted slices were obtained for independent assessments of the left and right amygdalae using sagittal T2-weighted images as references. The amygdala’s boundary was manually drawn using a freehand method for every coronal slice. To calculate the total amygdala volumes, the areas from each slice were added together and multiplied by the thickness of the slice. 28
Statistical analysis
Statistical analyses were conducted using SPSS (Statistical software for Social Sciences; SPSS Inc., Chicago, IL, USA) 22 software. The study used mean ± SD values for continuous data and n, % values for categorical data to provide descriptive data. Chi-square analysis (Pearson chi-square) was utilized to assess the normal distribution features of continuous variables using the Kolmogorov–Smirnov test when comparing variables between categories and groups. Independent samples t-test was used to compare data between two groups, and one-way analysis of variance (ANOVA) was used to compare data between more than two groups. To investigate the interval associations of continuous variables, Pearson’s test of changes was employed. Amygdala volumes in suicide attempts were used to determine the diagnostic value based on receiver operating characteristic (ROC) curves. p < 0.05 was considered to indicate statistical significance in the analyses.
Results
The study comprised 193 participants—85 people with a history of suicide attempts and 108 healthy controls. There were 37.6% more men and 62.4% more women in the suicide attempt group compared with 55.6% more women and 44.4% more men in the control group. The distribution of sexes among the groups did not differ significantly (p = 0.341) (Table 1).
Comparison of the clinical and demographic traits between the control and suicide attempt groups.
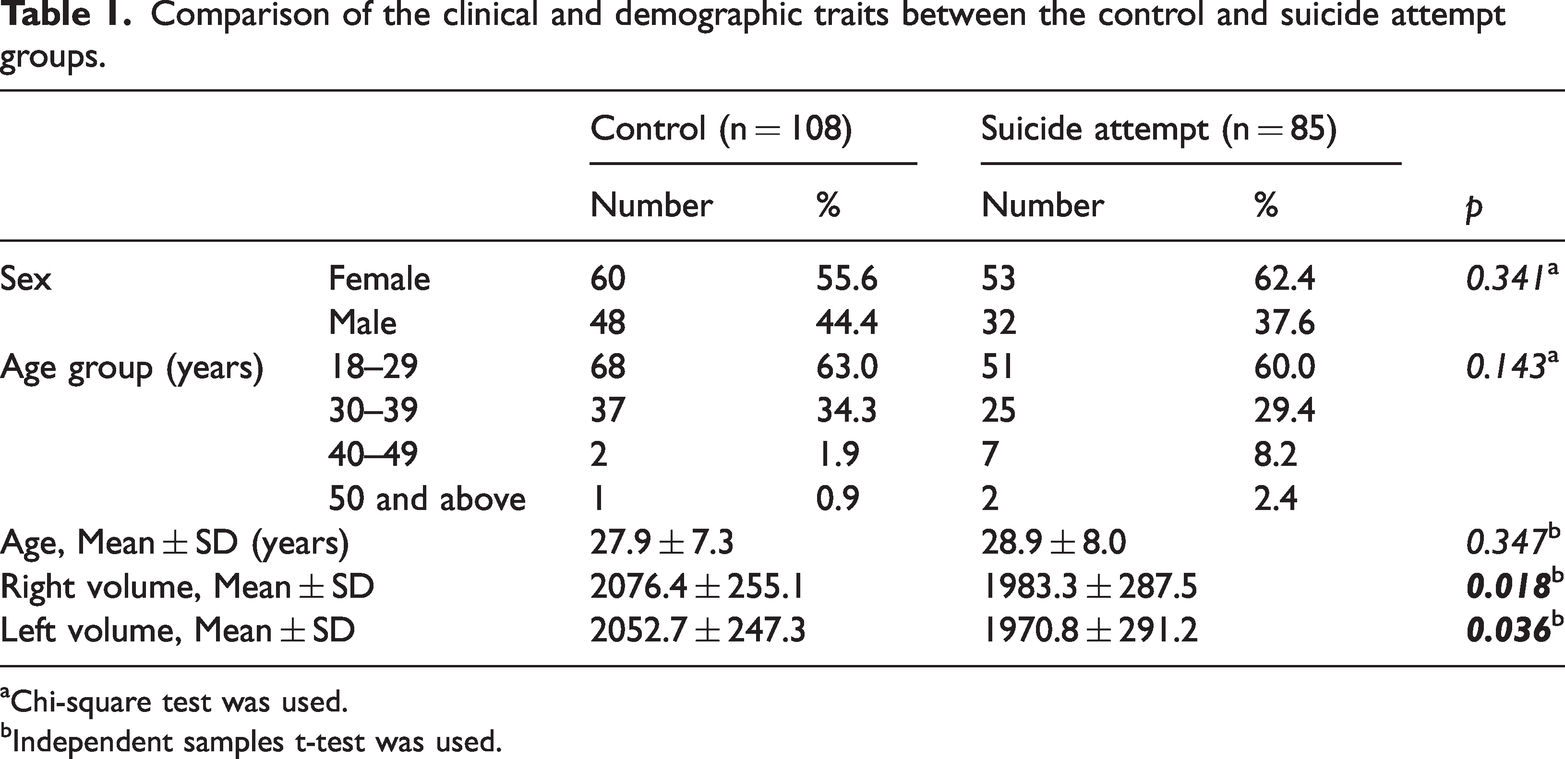
Chi-square test was used.
Independent samples t-test was used.
The mean age of the participants in the suicide attempt group was 28.9 ± 8.0 years, with 60% of them being between the ages of 18 and 29 years. The control group’s mean age was 27.9 ± 7.3 years, and 63% of them were between the ages of 18 and 29 years. Age group distributions (p = 0.143) and averages (p = 0.347) did not show any significant differences (Table 1). MRI results showed that the control group’s right (p = 0.018) and left (p = 0.036) amygdala volumes were considerably greater than those of the suicide attempt group (Table 1, Figure 1).
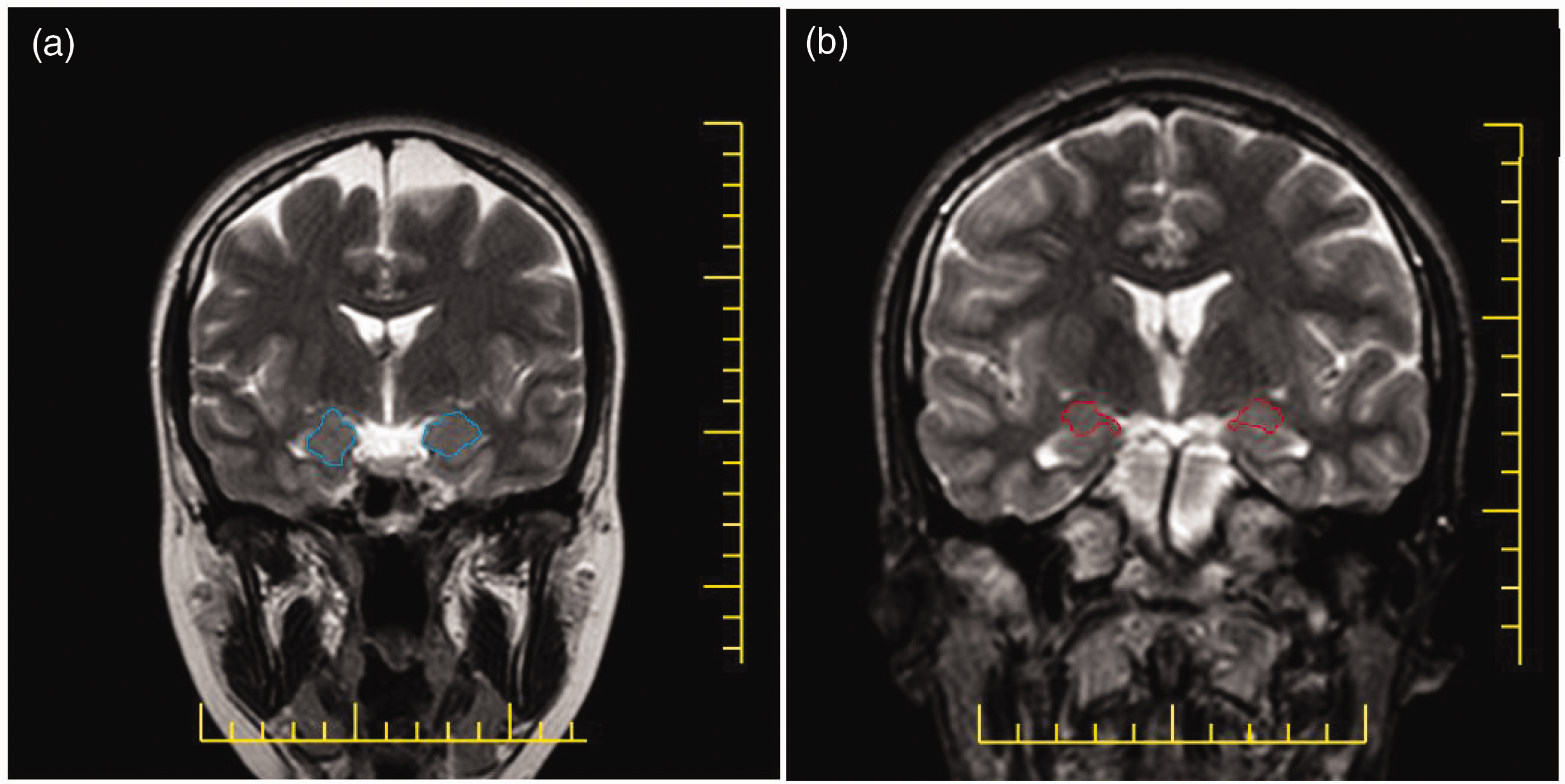
Representative amygdala cross-sectional images. (a) Control group and (b) suicide attempt group.
The right (p = 0.019) and left (p = 0.015) amygdala volumes of men in the control group were significantly higher than those of men in the suicide attempt group (Table 2).
Sex-based comparison of amygdala volumes.
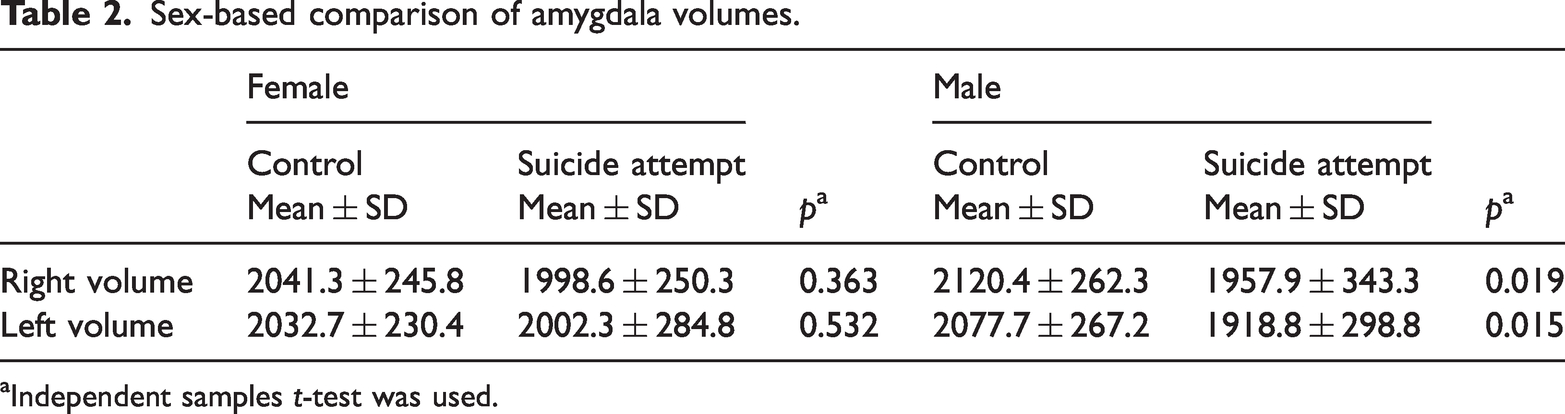
Independent samples t-test was used.
A cutoff value of 1825 mm³ was found via ROC analysis for both left and right amygdala volumes. The sensitivity and specificity for the right amygdala were 30.6% and 88%, respectively, with an area under the curve (AUC) of 0.583 (p = 0.047). The left amygdala had a sensitivity of 31.8%, specificity of 84.3%, and AUC of 0.593 (p = 0.025) (Table 3, Figure 2).
ROC analysis of amygdala volumes according to the state of suicide attempts.
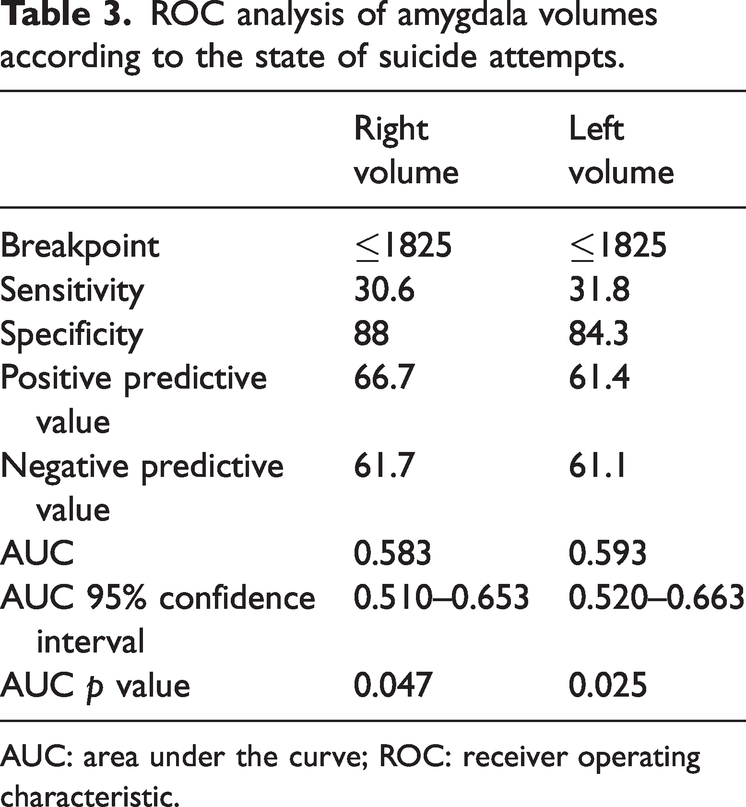
AUC: area under the curve; ROC: receiver operating characteristic.

Amygdala volume ROC curves for suicide attempt prediction. AUC: area under the curve; ROC: receiver operating characteristic.
There were no significant sex-related differences in the right (p = 0.530) or left (p = 0.202) amygdala volumes of the suicide attempt group (Table 4). Moreover, no significant age-related variations in amygdala volume were observed when participants in the control and suicide attempt groups were evaluated by age group (Table 5).
Sex-specific comparison of age and amygdala sizes in the suicide attempt group.

Independent samples t-test was used.
Comparison of amygdala volume by age group.

Independent samples t-test was used.
Discussion
Women constituted 62.4% of the suicide attempt group in our sample, which is consistent with other studies showing that the rate of suicide attempt is higher in women than in men. In particular, previous studies have shown that women are 1.78 times more likely than men to attempt suicide in their lifetime. However, it remains unclear if amygdala volume and suicide attempts in either sex are related. 29
This is the first study to demonstrate that the right and left amygdala volumes of individuals with a history of suicide attempts are smaller than those of healthy controls and that this difference is independent of age or sex. Additionally, prior research has demonstrated that younger people are more likely to attempt suicide. 30 Only 10.6% of those in our sample who attempted suicide were over the age of 40 years, compared with 60% who were aged ≤29 years.
Despite the fact that suicide is known to be more common in younger age groups, no previous study has determined whether amygdala volume and age are related in this situation. As there was no statistically significant variation in amygdala volume between age groups, our findings imply that early-life amygdala volume could be used as a baseline indicator for subsequent neurodevelopmental paths (Table 5). According to published research, the volume of the entire brain peaks at the age of 15 years and thereafter drops nonlinearly. According to reports, the amygdala volume peaks between the ages of 30 and 40 years and then gradually decreases. 31
The observed trends were in line with earlier research, despite the fact that our findings about age-related changes in amygdala volume were not statistically significant. Suicidal thoughts and actions have been linked to more structural alterations in the brain, especially in the amygdala. According to a previous study, variations in the right amygdala and right middle temporal gyrus that are seen before and after suicide attempts may even be biomarkers for the risk of suicide. 32
A study including 158 patients with MDD suggested that suicide attempts may be linked to decreased amygdala function. Functional dysregulation between the prefrontal brain and amygdala was identified by researchers as a potential contributing factor. 33 Cong et al. 34 also found that patients with MDD have bilateral decreases in the size of the central and medial amygdala nuclei.
In another study, the amygdala sizes of 44 schizophrenia patients with a history of suicide attempts were considerably smaller than those of 44 patients without such a history and 44 healthy controls. 35 However, there is a disagreement, as one study found that individuals with schizophrenia who attempted suicide had larger right amygdala volumes. 36
Although our study did not find a statistically significant difference in amygdala volume between men and women who attempted suicide, there are numerous neuroimaging studies and meta-analyses in the literature showing that men generally have larger amygdala volumes than women, and these differences are observed even when variables such as intracranial volume are controlled for. 37 The fact that such a difference was not detected in this study may be due to limitations such as sample heterogeneity or sample size. Therefore, further studies are needed to investigate sex-related structural differences in the brain associated with suicidal behavior.
In this study, people who had tried suicide had smaller left and right amygdala sizes. The available evidence indicates a potential connection between suicidal conduct and decreased amygdala volume, excluding contradictory results in patients with schizophrenia. With a sensitivity of 30.6% and specificity of 88% for the right amygdala and a sensitivity of 31.8% and specificity of 84.3% for the left amygdala, our ROC analysis indicated that amygdala volume may have biomarker potential. Moreover, older age is a distinct psychological and neurobiological risk category for suicide. Furthermore, hospital records do not always reflect the most recent psychiatric diagnosis at the time of suicide attempt.
Limitations of study
It is important to recognize the various limitations of this study. First, there was no longitudinal monitoring of amygdala volume changes over time. However, our study did not examine functional imaging (functional MRI, positron emission tomography) or neurochemical indicators such as serotonin and noradrenaline, which may be important for understanding the biology of suicide. As this is a retrospective study, the lack of information that could affect the participants’ mental state, such as history of brain trauma, psychiatric diagnoses, or substance use, is another important limitation. Another limitation is that amygdala volume was not normalized according to variables such as total brain volume or intracranial volume. Unfortunately, as total brain volume and intracranial volume data were not calculated in our study sample, these variables could not be evaluated as covariates in statistical models. People between the ages of 18 and 55 years were included in the study, while older people were not.
Conclusion
Notwithstanding these drawbacks, our research is the first to show that people who have attempted suicide had a significantly lower amygdala volume. Early detection of decreased amygdala volume may help physicians provide early psychological support and caregivers keep a closer eye on at-risk individuals. Future research that employs multimodal imaging techniques, broadens the age range to cover older age groups, or assesses comprehensive clinical and psychiatric data, including participants’ comorbidities and drug use history, should be guided by the findings of this study. This approach might help reduce the frequency of suicide attempts, particularly among people with MDD, and be a beneficial contribution to public mental health initiatives.
Footnotes
Acknowledgements
We extend our heartfelt gratitude to all those who have contributed to the successful completion of this present project.
Author contributions
Conceptualization, E.E., S.Y., A.R.Y.B., and S.A. (Suna Aydin); methodology, E.E., S.Y., G.K., S.A. (Suna Aydin), and S.A. (Suleyman Aydin); software, G.K., E.P.A., and S.A. (Suleyman Aydin); validation, G.K. and S.A. (Suleyman Aydin); formal analysis, S.Y., G.K., and S.A. (Suna Aydin); investigation, E.E., S.Y., G.K., S.A. (Suna Aydin), and S.A. (Suleyman Aydin); exercise training, E.E., S.Y., G.K., and S.A. (Suleyman Aydin); biochemical analyses, E.E., E.P.A., and S.A. (Suleyman Aydin); preparation and storage of tissue supernatants, E.E., G.K., S.A. (Suna Aydin), E.P.A., and S.A. (Suleyman Aydin); writing—original draft preparation, E.E., S.Y., S.A. (Suna Aydın), and S.A. (Suleyman Aydin); writing—review and editing, E.E., A.R.Y.B., E.P.A., B.S.E., İ.S., and S.A. (Suleyman Aydin); visualization, E.E., G.K., S.A. (Suna Aydin), and İ.S.; supervision, E.E., and S.A. (Suleyman Aydin); project administration, E.E., S.Y., and S.A. (Suleyman Aydin). All authors have read and agreed to the published version of the manuscript.
Data availability statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Declaration of conflicting interests
The authors declare no conflicts of interest with respect to this article.
Funding
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.