
Abstract
Family caregivers of persons living with dementia (PLWD) are often expected to coordinate and manage all aspects of a loved one’s day-to-day care across settings with limited modern, user-friendly resources to support them. We developed CareMOBI, a mHealth app prototype that aims to support improved care coordination and communication between care team members. A concurrent mixed-methods triangulation design was used to assess the acceptability and likelihood of adopting CareMOBI among family caregivers of PLWD. Caregivers (n = 13) completed the Technology Acceptance Model questionnaire (quantitative) and semi-structured interviews (qualitative). Integration occurred using the four themes of the Technology Acceptance Model. There was strong agreement among family caregivers that CareMOBI had a high perceived value for care (M = 6.23/7), was easy to use (M = 6.20/7), and enhanced current workflows (M = 5.86/7). However, training in utilizing mHealth apps and the need for a Spanish-language version were cited as necessary enhancements to increase the widespread adoption of CareMOBI.
Introduction
More than 16 million Americans are providing 17 billion hours of unpaid care to persons living with dementia (PLWD) in the United States (Centers for Disease Control and Prevention, 2023). About 67% of family caregivers of PLWD (children, spouses) assume caregiving responsibilities that involve complex medical tasks such as personal care, giving injections, diet management, addressing behavioral challenges, and ensuring safety and supervision; all of which are complicated by behavioral changes, multiple chronic conditions, and limited cognitive function of care recipients (Lee et al., 2019; Vipperman et al., 2023). Yet, family caregivers of PLWD often lack adequate support and resources to meet expectations, resulting in costly and avoidable adverse health outcomes (Vipperman et al., 2023).
Family caregivers may face challenges coordinating and managing the healthcare for a PLWD. Over one-fourth of family caregivers (26%) from a nationally representative sample report difficulty coordinating their loved one’s care which includes scheduling and attending medical appointments, communicating with healthcare professionals, and maintaining medical records (AARP, 2020). Our previous research has shown that family caregivers serve as brokers of communication across community settings (which often lack electronic health records systems) and formal healthcare systems, resulting in delays or inaccuracies in information exchange (Zhong et al., 2022). However, a systematic review highlighted that a major area of need among family caregivers of PLWD is timely, tailored, centralized information sharing that allows them to adapt to care recipients’ ever-changing needs (Bressan et al., 2020).
Navigating the healthcare system is complex for family caregivers because of ineffective care coordination, limited care options, and a lack of access to resources. Mobile health (mHealth) describes public health and medical practice using smartphones, sensors, personal digital assistants, wireless monitoring devices, or other wireless devices (Istepanian, 2022). mHealth applications (apps) are considered an effective intervention for developing disease-specific management skills among community-dwelling older adults and hold the potential to facilitate seamless communication and centralize care coordination between family caregivers and healthcare providers (Wong et al., 2020). Family caregivers can use mHealth apps to share messages, updates, and pose questions which eliminates the need for in-person visits (Yousaf et al., 2019). However, barriers to family caregivers’ ease and level of usage of technology in dementia care include poor knowledge of available technologies and skills to utilize them (Boyle et al., 2022). In addition, mHealth apps designed to improve care navigation tend to be introduced to family caregivers in later stages of dementia where they may be less effective in preventing adverse outcomes (Boyle et al., 2022). Well-designed mHealth apps may promote comprehensive care for PLWD by facilitating effective communication between family caregivers and healthcare providers, providing timely access to resources, medication management, monitoring health conditions, and proactive planning to address potential emergencies (Sala-González et al., 2021). However, the creation of mHealth apps must consider barriers to technology adoption in dementia care, while also evaluating whether caregivers find them practical and appealing to encourage their widespread use.
We developed CareMOBI (mHealth for Organizations to Bolster Interconnectedness), a mHealth app prototype (see Figure 1), to address the consistent need for improved care coordination and communication between members of a care team. CareMOBI is a low-cost, centralized platform for exchanging information between family caregivers, healthcare providers, and community-based organizations. CareMOBI’s features are designed to support critical early identification of clinical issues to reduce costly, traumatic, and avoidable emergency department care or hospitalizations, as well as overall care management for individuals with complex care needs. The CareMOBI app is an attempt to be responsive to the needs of family caregivers managing complex medical tasks.

A visualization to showcase the CareMOBI application.
Our specific research questions included:
How do family caregivers of PLWD rate the acceptability of the CareMOBI prototype according to the four domains of the Technology Acceptance Model Questionnaire?
How do family caregivers describe their experience interacting with the CareMOBI prototype and its potential impact on their caregiving needs?
The purpose of this mixed-methods study was to examine the feasibility and acceptability of CareMOBI through surveys and interviews with family caregivers of PLWD to meaningfully inform future iterations of the app.
Methods
We used a concurrent mixed-methods triangulation design to (a) assess the acceptability of the CareMOBI prototype among caregivers of PLWD and (b) identify factors contributing to the eventual likelihood of adoption.
Setting and Sample
Participants were eligible if they (a) were currently caring for or had previously cared for a PLWD, (b) were over the age of 18, and (c) owned a smartphone. Individuals who did not speak English were excluded because the prototype was only available in English. In addition, the perspective of healthcare providers was not included as they are addressed in a previous manuscript (Zheng et al., 2024). This previous study interviewed 22 adult day staff members (e.g., nurses, physicians) to assess the feasibility and acceptability of CareMOBI as the effectiveness of CareMOBI for care coordination relies on their participation alongside family caregivers (Zheng et al., 2024). Eligible participants were purposively recruited with the help of administrators at participating adult day centers in New York and California who were in contact with family members of PLWD. A research assistant contacted them by email and/or phone, described the study, confirmed participants’ eligibility, and obtained informed consent. All enrollees received a $50 gift card for their participation. The New York University Committee on Activities Involving Human Subjects (UCAIHS) provided Institutional Review Board approval for this study.
Procedures
Data collection consisted of one-on-one semi-structured interviews and completion of the Technology Acceptance Model Questionnaire (Gagnon et al., 2012). One week before the interview, participants received a confirmation email with a link to an interactive prototype of CareMOBI and a 2-min informational video that could be accessed from a smartphone, tablet, or computer. Participants were asked to spend about 10 min navigating through the prototype to complete tasks including logging in, using filters to locate information, adding a new medication, and recording the typical day-to-day activities and health-related progress notes of a PLWD.
Qualitative Data Collection and Analytic Procedures
Online interviews were scheduled based on participants’ availability and conducted virtually via a secure online platform. UX (user experience)/UI (user interface) design professionals in user testing at the product development firm that built the CareMOBI prototype provided input to develop a semi-structured interview guide (see Supplemental Material). Participant interviews were approximately 30 min in length. Interviews were conducted by either the principal investigator (TS) who has received formal training in mixed-methods research and published extensively using qualitative methods or a junior research scientist (JB) with a Master’s in Public Health. Member checking took place informally during data collection. The interviewer would pause after major questions to summarize and confirm their interpretation of a participant’s responses. Open-ended questions allowed participants to elaborate on their reaction to the CareMOBI app and allowed the researchers to elicit information on factors influencing their perceptions of the app, aspects regarding its usability, potential barriers, and facilitators of eventual adoption. All interviews were recorded, professionally transcribed, and reviewed for accuracy. Field notes by the interviewer supplemented recorded interviews. Given the possibility of response bias, both interviewers maintained an audit trail/reflexive journal to document observations and reflections throughout the data-gathering process. This included decisions about follow-up questions asked and reactions to responses. Interviewers met regularly to review transcripts and discussed whether they may have influenced participant responses which supported an honest and reflexive process.
Qualitative data were analyzed using directed content analysis to provide a systematic coding process, and an a priori codebook was utilized as a coding scheme for all transcripts (Hsieh & Shannon, 2005). Codes were summarized within cases and then categorized within the four domains of the Technology Acceptance Model: likelihood of adoption, perceived ease of use, perceived value in clinical care, and fit within the existing workflow for initial coding categories (Gagnon et al., 2012). The research team (MFC, AZ, KBS, TS) discussed any text that could not be categorized within the codebook to determine if a new category or code needed to be defined or aligned with an existing category or code. Two coders who were PhD (MFC) and undergraduate nursing students (KBS) independently coded in Dedoose, a web-based platform for qualitative and mixed-method coding. The principal investigator (TS) analyzed a subset (20%) of transcripts to ensure reliability and rigor. The research team regularly debriefed to discuss and validate the analysis results, select illustrative quotes from a range of participants, update the codebook to reflect this iterative process, and saturation occurred when no new categories were identified (Hsieh & Shannon, 2005).
Quantitative Data Collection and Analytic Procedures
Upon finishing the interview, participants provided demographic information and completed an online adapted version of the Technology Acceptance Model Questionnaire, which was previously validated for use in healthcare settings (Gagnon et al., 2012). Responses to the 33 survey items enabled further examination of factors that could influence the eventual adoption of CareMOBI, and the anonymous nature reduced the potential for social desirability bias. Participants rated each item on a seven-point Likert scale ranging from “totally disagree” to “totally agree.” Each domain-specific question was averaged to determine scores and higher scores corresponded to higher perceived feasibility and acceptability. Descriptive statistics were used to characterize the sample, measures of central tendency and spread for continuous measures, and frequencies and percentages for dichotomous or categorical variables were performed in Qualtrics.
Integration of Qualitative and Quantitative Data
Qualitative and quantitative data were integrated in the third and final phase of analysis. We sought to align with the Technology Acceptance Model: perceived ease of use, perceived value in clinical care, fit within existing workflows, and end-users’ overall likelihood of adoption. Using the four themes as anchors, we developed an informational matrix (see Tables 2–5) in which qualitative data were embedded and compared to quantitative data. Using triangulation methods, we sought to understand the overall likelihood of end-users’ adoption of the app (quantitatively) and factors underpinning this across cases within each stakeholder group (qualitatively).
Results
The primary goals of this study were to (a) assess the acceptability of the CareMOBI prototype among family caregivers of PLWD and (b) identify factors contributing to the eventual likelihood of adoption or non-adoption of the mHealth app. We evaluated the feasibility and acceptability of CareMOBI use among family caregivers quantitatively and qualitatively based on four overarching themes: perceived ease of use, perceived value in clinical care, fit within caregiver workflow, and likelihood of adoption.
Study Sample
The total sample (n = 13) of caregivers of PLWD was majority White (53.85%) and between the ages of 50 to 59 years (30.77%) and 60 to 69 years (30.77%) (see Table 1). More than half of the respondents identified as female (61.54%), and the majority (53.85%) identified as children of PLWD for whom they were caring.
Demographic Characteristics of Dementia Caregivers.

Perceived Ease of Use
Perceived ease of use refers to the level of difficulty related to navigating and using CareMOBI. There were six questions within the Technology Acceptance Model Questionnaire presented to the caregivers that assessed perceived ease of use: overall ease, flexibility, technological skills, and general user comfortability with the mHealth app (see Table 2). The mean score of this theme was 6.23, indicating a high perceived ease of use for CareMOBI among caregivers. Within the quantitative survey, the question with the highest mean score was “I think I will find it easy to acquire the necessary skills to use this app” (M = 6.62 or strongly agree). “I think that the proposed app is a flexible technology to interact with” and “I feel comfortable with information and communication technologies” (M = 5.92 or agree) were questions with the lowest mean score.
Caregiver’s Perceived Ease of Use of CareMOBI.


The qualitative interviews revealed specific aspects of CareMOBI that made it easy for caregivers to manage and care for a PLWD. Aligned with the quantitative data, many of the participants reported that the design and setup of the app were user-friendly, which they found helpful in managing the care and healthcare information of PLWD. Caregivers also reported comfortability with technology, reflecting the mean score of 5.92 on the quantitative data, as they “[grew] up with computers and apps and phones . . . ” (CG-LW). Despite the positive reviews of CareMOBI’s design and ease of use, the qualitative interviews further revealed potential challenges such as no additional language options that could affect diverse caregivers’ ability to navigate and efficiently use the app to complete their caregiving duties. For example, one participant stated having a “Spanish version” of the app is warranted (CG-ESD).
Perceived Value for Clinical Care
The perceived value for clinical care describes the degree to which CareMOBI enhances or improves the ability of caregivers to care for and manage the health and records of PLWD. The Technology Acceptance Model Questionnaire had seven questions that pertained to this quality of CareMOBI (see Table 3). The overall mean of this theme was 6.20, indicating that most caregivers agree that CareMOBI has significant value for clinical care. The question with the highest mean score was “In my opinion, the use of the proposed app will have a positive impact” (M = 6.45 or strongly agree). The question with the lowest mean score was “I find it interesting to use the proposed mHealth app for the monitoring and management of my patients” (M = 5.85 or agree).
Caregiver’s Perceived Value in Clinical Care of CareMOBI.


The qualitative data from caregiver interviews highlighted how the features of the app benefited the caregivers’ roles in caring for PLWD. Caregivers expressed that the app’s features helped enhance communication, organization, and coordination of care for PLWD. One caregiver viewed CareMOBI’s ability to keep them more organized and “on top of things” as invaluable (CG-FT). This aligns with the quantitative data where caregivers agreed that CareMOBI will make it easier to perform tasks needed to manage the care of PLWD. CareMOBI’s ability to provide healthcare information at the point of service and inform others how to care for PLWD in emergencies (e.g., advance directives) was found to be vital for caregivers. In addition, CareMOBI provides positive value for care through real-time communication of the health progress of and information on PLWD. CareMOBI’s features allow the care team to be “on the same page” (CG-ESD) regarding the health of patients and may be conducive to coordinating dementia care. For instance, one caregiver stated, “if family members had access to this information, or at least be able if you, as a caregiver, can share that with them, it’s a helpful tool so people have a snapshot of what’s happening with your loved one at any given time” (CG-FT).
Fit Within the Caregiver Workflow
The development of new mobile apps such as CareMOBI must enhance or continue the established workflow family caregivers maintain for patient care. Nine questions assessed the extent to which CareMOBI fits into the caregiver’s routine around monitoring, managing, and supporting the care of PLWD (see Table 4). The mean domain score (5.86) indicated that CareMOBI fits within most caregiver’s day-to-day workflow. The item with the highest average score was “I think it is a good idea to use the proposed mHealth app to monitor/manage my loved one” (M = 6.54 or strongly agree). The item with the lowest average score was “My loved one will welcome the fact that I use the proposed mHealth app” (M = 4.77 or neither agree nor disagree).
How CareMOBI Will Fit Within the Workflow of Caregivers.


Qualitative data aligns with the quantitative data; however, explicit statements from caregivers describe how CareMOBI may be integrated into the current workflow. Several caregivers noted that they were aware of existing mobile apps, but presently rely on separate notes, cameras, and calendar apps to manage a PLWD care. Participants discussed that CareMOBI was a centralized application that could link other apps to conform and improve the management of caregiving duties. Participants were also unanimous in agreeing that medication management would be streamlined more easily. For example, one participant (CG-TN) stated, “As far as scanning the labels of the medication is fantastic.” Family caregivers noted that CareMOBI may prevent errors in medication administration and reduce the time spent inputting medications by hand due to scanning. This is consistent with the quantitative data that CareMOBI could efficiently manage a PLWD care, especially with medication management. Many participants also conveyed the difficulties of having minimal guidance or support as family caregivers of a PLWD, but found CareMOBI to be a modern intervention that could facilitate care coordination and reduce caregiver burden.
Likelihood of Adoption
This domain assessed the extent to which family caregivers intend to adopt and include CareMOBI in the care management of PLWD. Nine questions assessed this domain with a mean score of 5.46, suggesting most respondents agreed that they intended to use CareMOBI once released (see Table 5). The highest average item was “I often use smartphone apps in my work or daily life” (M = 6.45 or strongly agree) and the lowest average item was “I have already used a smartphone app to manage my loved ones” (M = 3.46 or disagree).
Caregiver’s Likelihood of Adopting CareMOBI.
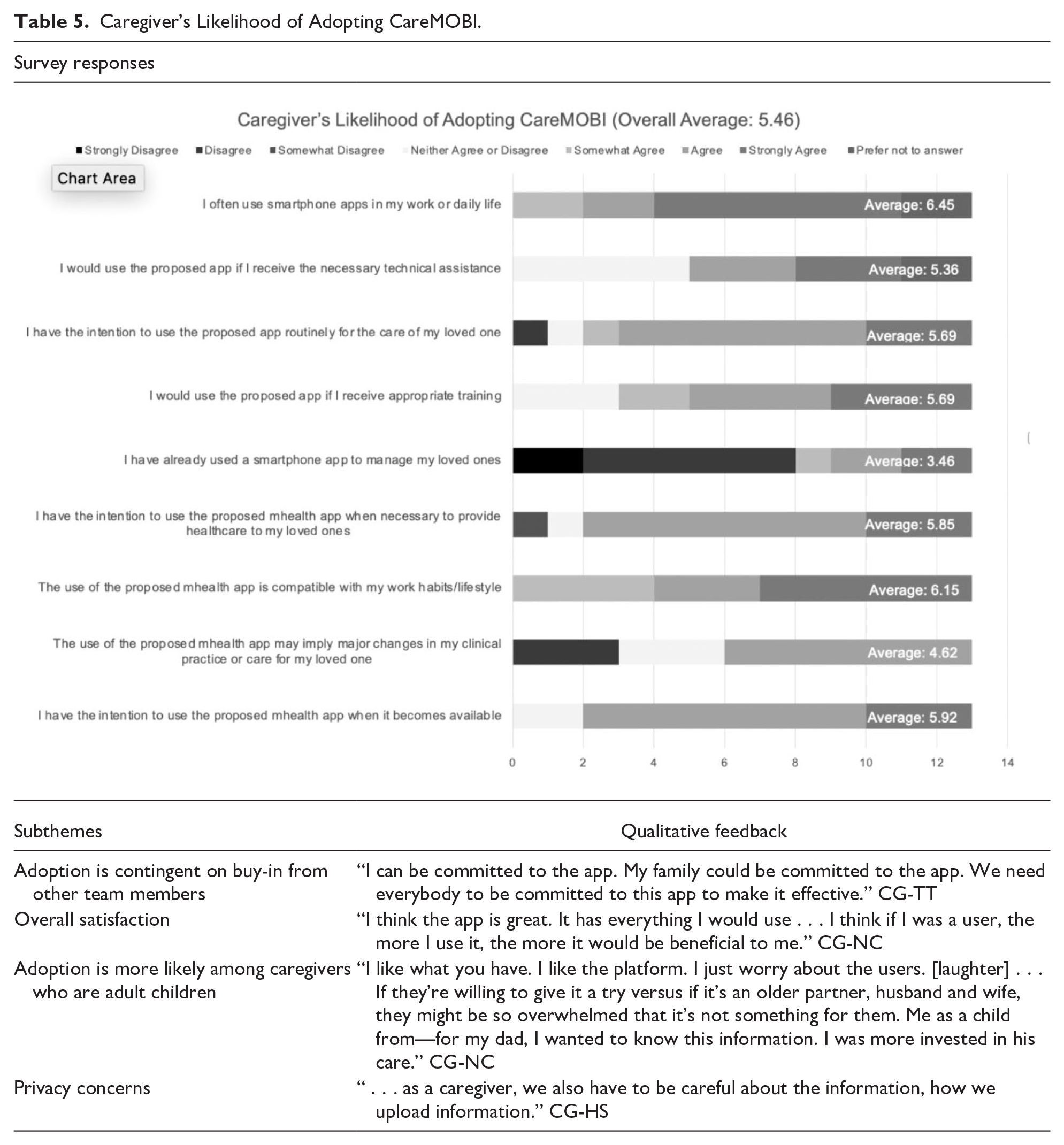

The qualitative data revealed that caregivers believed CareMOBI would be beneficial and enhance their current workflow, but some concerns precluded the adoption of the app. One participant (CG-TT) stated, “It’s getting all the partners that are involved in caretaking to use the app . . .. I thought of that as a potential challenge.” Wariness about family members and healthcare professionals’ involvement and commitment to utilizing CareMOBI existed. Furthermore, caregivers were apprehensive of the targeted population for CareMOBI due to generational differences such as age, which reflects the lowest quantitative score of not having used a mHealth app to manage the care for PLWD. Lastly, some participants emphasized the importance of confidentiality of patient health data and for information in CareMOBI to only be accessed by the care team. To increase the likelihood of adoption, caregivers suggested additional training and support for family caregivers in utilizing CareMOBI for the care management of PLWD.
Discussion
The purpose of this mixed-methods study was to assess the acceptability and likelihood of adopting CareMOBI, a novel mHealth app to improve care coordination and communication among family caregivers of PLWD and those who support them in providing care (e.g., adult day centers, primary care providers). Though the quantitative and qualitative data were primarily positive in terms of the perceived value for clinical care, ease of use, and enhanced current workflow, the CareMOBI prototype must fully address the needs of family caregivers.
Our quantitative data shows despite the widespread use of smartphones in caregivers’ daily lives (6.45), the qualitative responses reveal that no single app or method is widely used to manage care for PLWD. Family caregivers are currently improvising with multiple apps or using paper and pencil to manage and organize health information. This is consistent with a prior content analysis that found the availability of mHealth apps catering to caregivers was sparse and not comprehensive in integrating multiple functions (e.g., safety, medication management, family communication; Grossman et al., 2018). Our findings suggest that CareMOBI is an innovative mHealth app that addresses an unmet need among family caregivers for support with the day-to-day management of PLWD.
CareMOBI particularly enhances family caregivers’ medication management. Studies have demonstrated that family caregivers often assume multiple and complex medication management roles, such as administering multiple medications, creating medication administration schedules, and avoiding medication errors and possible drug reactions which may be overwhelming (Gillespie et al., 2014; Look & Stone, 2018). Furthermore, medication non-adherence is associated with a greater number of emergency department visits and hospitalizations (Roebuck et al., 2018). CareMOBI enables family caregivers to maintain up-to-date medication lists alongside reminders and push notifications. Family caregivers unanimously agreed that CareMOBI would simplify medication management by allowing for organization, maintenance, and access to updated lists of all medications to ensure patient safety, optimize therapeutic outcomes, and may support greater medication adherence.
Family caregivers view CareMOBI as having tremendous value by supporting timely communication and enhancing efficiency for caregivers who have little time. By providing real-time communication of health information from various healthcare professionals, CareMOBI serves as a tool to help caregivers “stay organized and on top of things” (CG-FT). Moreover, family caregivers have information available at the point of service, instead of struggling to identify pertinent information or questions to share during healthcare appointments that are often short. For example, primary care appointments with physicians last around 18 min, and appointments that are scheduled to last around 30 min, tend to end earlier than expected (Neprash et al., 2021). With shorter wait times, only 14% of physicians feel as if they have time to provide care that is of high quality (Prasad et al., 2020). Furthermore, family caregivers have less time to discuss and understand the current health concerns of caregivers of PLWD. CareMOBI’s ability to present comprehensive healthcare information about the patient at the point of service, during short primary care visits, may allow caregivers to share imperative information and remember to ask specific questions they have about a PLWD during the visit.
The survey results suggest that family caregivers found the app to be compatible with their current practices and have high intentions to use the app once available to support the care of a PLWD. The quantitative data also showed that family caregivers were highly likely to use CareMOBI if they received training. The qualitative data showed that given the generational differences in technology use, training is warranted. The use of and access to technological devices is not a significant barrier to overcome, and many caregivers expressed intent to use CareMOBI. Rather, CareMOBI must be presented in a form that is easy to navigate, and training must be provided for older and middle-aged adult caregivers for whom mHealth apps may be new. Our findings support the need to familiarize caregivers with using CareMOBI and are consistent with a scoping review which found that caregivers receive insufficient support and education to properly utilize mHealth apps (Park et al., 2022). With proper training, family caregivers may effectively use mHealth apps like CareMOBI to regularly improve care coordination and management of PLWD.
The likelihood of adopting CareMOBI was high. Past research has shown that mHealth apps are primarily used by early adulthood adults (under 35 years) and that family caregivers tend to be spousal partners (Paradis et al., 2022; Pinquart & Sorensen, 2011; Wang & Qi, 2021). However, our sample was primarily children of PLWD and the majority were above 50 years of age, which aligns with recent findings of lower spousal availability and more adult children managing a PLWD care (Choi et al., 2021). In addition, security and privacy are paramount concerns among people adopting mHealth apps (Schroeder et al., 2022). CareMOBI incorporates the highest security standards including secure and encrypted servers that allow for secure data storage and exchange that align with standards set forth by the Health Insurance Portability and Accountability Act (HIPAA). Further, there is a gap in accessibility as CareMOBI is only available in English, and the population of PLWD is diversifying. mHealth apps like CareMOBI must provide pertinent designs that meet users’ cultural and language needs to enhance the likelihood of adoption and utilization rates to achieve participation and health equity for all caregivers of PLWD. Adapting CareMOBI for Spanish-speaking caregivers will be a priority, given the projected sevenfold increase in Latinos and Hispanics with dementia by 2060 (Matthews et al., 2019).
CareMOBI was developed as a reaction to the overwhelming sentiment that care coordination and methods of communication between care team members in home and community settings need to be modernized and streamlined to provide optimal care for PLWD. Overall, our results from prototype testing show a high level of feasibility and acceptability among family caregivers of PLWD. Recognized by many of the study participants, CareMOBI’s greatest strength is its ability to provide centralized care management functions and communication between healthcare providers, caregivers, patients, and adult day services staff. Improved care coordination is needed for family caregivers as our traditional healthcare system is not well suited to manage the complex care of PLWD due to limited routine monitoring and appropriate technology that facilitates communication among care team members that enables real-time updates and support that CareMOBI aims to provide (Hughes et al., 2017).
While the results suggest a high likelihood of adoption for CareMOBI, the study had certain limitations. The study had a small sample size (n = 13), and the participants were only furnished with a prototype of the CareMOBI application with limited capabilities. In addition, our purposive sampling strategy may have resulted in a relatively young sample of family caregivers with higher socioeconomic status and education levels. CareMOBI may also be more attractive to family caregivers who are more familiar and proficient with using technology. While the study sample may not reflect the broader caregiver community and limits the generalizability of our findings, we followed design-thinking principles which involve frequent cycles of feedback and improvement according to end-users which strengthened our final prototype (Micheli et al., 2019).
Conclusion
We assessed the acceptability of the CareMOBI prototype for family caregivers of PLWD and the factors affecting their likelihood of adopting this application. Our findings indicate that family caregivers of PLWD are highly likely to utilize CareMOBI once it is available; however, the qualitative interviews highlighted important barriers to successful implementation that will be considered as the research team moves to the next phase of CareMOBI’s development.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214241275638 – Supplemental material for Exploring Family Caregivers’ Likelihood of Adopting a Novel App That Connects Care Teams of Persons Living With Dementia: A Mixed-Methods Study
Supplemental material, sj-docx-1-ggm-10.1177_23337214241275638 for Exploring Family Caregivers’ Likelihood of Adopting a Novel App That Connects Care Teams of Persons Living With Dementia: A Mixed-Methods Study by Moroni Fernandez Cajavilca, Amy Zheng, Kehinde Bamidele-Sanni and Tina Sadarangani in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
We thank Jonelle Boafo for assisting with qualitative data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication is supported by the National Institute on Aging (NIA) of the National Institutes of Health (NIH) under Award Numbers: (1) R21AG069801; (2) U54AG063546, which funds NIA Imbedded Pragmatic Alzheimer’s and AD-Related Dementias Clinical Trials Collaboratory (NIA IMPACT Collaboratory); (3) K23AG071948.
Ethics Approval and Consent to Participate
The New York University Committee on Activities Involving Human Subjects (UCAIHS) provided Institutional Review Board approval for this study. Informed consent was obtained from all study participants for study participation before interviews.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.