
Abstract
People living with Alzheimer’s disease (PLWD) often face unmet care needs, which may arise as caregivers and PLWD differ in their perceptions of PLWD’s needs. To understand how these discrepancies vary by caregivers’ perspective taking (i.e., their ability to understand PLWD’s thoughts and feelings), we conducted a sequential mixed-methods study with 67 couples managing Alzheimer’s disease. Both spouses completed semi-structured interviews to describe PLWD’s needs and discussed how they communicated about needs. Caregivers’ perspective taking was negatively associated with discrepancies in PLWD’s needs. Thematic analysis of a subgroup parallel sample demonstrated that, when caregivers reported high perspective taking, couples described navigating PLWD’s needs through open dialogue and caregivers adopted respectful communication practices. When caregivers reported low perspective taking, couples described misaligned expectations and communication efforts; caregivers initiated communication to identify PLWD needs and acknowledged employing insensitive language. Findings can inform interventions to improve the quality of dementia care and promote health.
• This study illustrates how and why caregivers’ perspective taking can direct their efforts to understand and meet the needs of PLWD. • Through mixed-methods triangulation, this study demonstrates that perspective taking facilitates couple communication and enhances caregivers’ awareness of and responses to PLWD’s needs.
• Our findings underscore the role of constructive communication between PLWD and care partners in identifying and addressing the needs of PLWD. • Our findings add to a growing body of research that has identified the role of caregiver perspective taking in dementia care. • Our findings inform interventions that may integrate perspective taking training to reduce unmet needs and optimize the quality of dementia care.What This Paper Adds
Applications of Study Findings
Introduction
People who have Alzheimer’s disease (AD) live with deteriorating mental functions and experience intensive care needs in various areas of their lives (Curnow et al., 2021). Some of their needs are satisfied (i.e., met needs) by widely available social, environmental, and clinical support, whereas others may not be sufficiently or adequately addressed (i.e., unmet needs). In mild to moderate AD, it may be possible to avoid situations where needs are persistently unmet if the people living with AD (PLWD) and their family care support system are appropriately equipped to identify and address needs. Nonetheless, PLWD commonly experience persistent unmet needs (Black et al., 2019), and PLWD and caregivers report discrepancies in their understanding of PLWDs’ unmet needs (Mazurek et al., 2019). Unmet needs in PLWD exacerbate their behavioral problems and functional declines, predict nursing home placement, increase caregiver burden, and compromise both parties’ health-related quality of life (Gaugler et al., 2005; Monin et al., 2020; Read et al., 2021; Wammes et al., 2024). Unmet needs emerge for various reasons, and the current study examined one situation in which PLWD and caregivers differ in their perceptions of what PLWD need and how their needs can be addressed (Mazurek et al., 2019; Monin et al., 2020; Wammes et al., 2024).
Framed by the theory of dyadic illness management (Lyons & Lee, 2018), discrepancies in perceived needs reflect a lack of shared appraisal of AD between PLWD and caregivers and pose challenges to cooperative efforts to manage the disease (Shrout et al., 2024). Thus, identifying factors underlying these discrepancies is critical for enhancing caregivers’ ability to understand and incorporate PLWD’s perspectives into communication and decision-making, which can help reduce resistance to care, facilitate illness management, and promote optimal outcomes for both PLWD and their caregivers. We sought to address this aim and focused on couples, including a PLWD and a spousal caregiver because spouses are typically the first to attend and respond when PLWD incur needs (Zarit et al., 2019).
Perceiving PLWD’s needs may rely on caregivers’ perspective taking—their ability to put themselves in the PLWD’s shoes to consider their thoughts and beliefs. Perspective taking varies across individuals but is fundamental to identifying others’ needs and taking action to provide fine-tuned help (Batson, 2010; Davis, 2015). Prior research with partnered adults has revealed that greater perspective taking was associated with less negative help to partners (i.e., help that was perceived as unhelpful or inappropriate; Devoldre et al., 2016). Yet, it remains unclear how one’s perspective taking affects their perceptions of others’ needs, particularly in an AD care context. We addressed this gap in the context of caregiving for a PLWD and examined whether greater perspective taking in caregivers was associated with smaller discrepancies between self-reports and caregivers’ reports of PLWD’s needs.
Further, we integrated the Systemic-Transactional Model to explore dyadic communication as a pathway by which caregivers’ perspective taking affects spousal discrepancies in perceived needs of PLWD. This model emphasizes communication patterns as key predictors of how dyad members perceive and appraise the nature and severity of illness symptoms (Bodenmann et al., 2016). It is possible that perspective taking facilitates effective communication approaches as couples cope with stress (O’Brien et al., 2009), which in turn contributes to greater understanding within couples. Indeed, an observational study with 50 Belgian married/cohabiting couples aged 22–76 coded both partners’ behaviors when one talked about a problem the couple had. They found that participants scoring higher on perspective taking were less likely to engage in negative behaviors (e.g., criticize spouse, minimize problem, be inattentive) during couple interactions (Verhofstadt et al., 2016). In the context of severe illnesses, high-quality communication can lead to greater agreement on symptom interference and severity, as has been reported in a recent study with dyads managing glioma (Whisenant et al., 2024). In the context of AD specifically, it remains unclear what communication patterns may promote dyads’ shared understanding of the PLWDs’ needs, warranting inductive exploration.
The Current Study
This study utilized a mixed-methods approach to describe discrepancies in self-perceptions and caregivers’ proxy perceptions of PLWD’s needs and examine whether and in what ways caregivers’ perspective taking is associated with these discrepancies. We tested the quantitative association between caregivers’ perspective taking and the discrepancies (between caregivers and PLWD) in perceived needs of PLWD and then drew on qualitative data to understand dyadic processes underlying this association. The qualitative component was intended to contextualize and describe potential differences in communication patterns observed across couples in which caregivers reported high vs. low perspective taking.
Methods
Participants
We used data from couples who completed two interviews in the Dyadic Study on Empathy in Caregiving (see study details in Huo et al., 2024). Upon approval by the University of California, Davis (UCD) Institutional Review Board (#1531955), the project was conducted in 2022–2023 with couples in which one person was living with mild-to-moderate AD and their married spouse or cohabiting partner provided the majority of assistance (i.e., serving as the primary caregiver). All but two couples were married so we referred to all caregivers as spousal caregivers. All couples resided in the Northern California-Nevada area and the sample was recruited primarily via UC Davis Health and local support groups via mychart messages and phone calls. We screened people with AD to be age 55+ and have received a clinical diagnosis of mild or moderate AD from a neurologist. Inclusion of people with moderate AD was determined during the screening and consent process by the research team. Eligibility was determined based on whether people with moderate AD were able to verbally express their thoughts and demonstrate sufficient understanding of the study purpose, procedures, and potential risks and benefits. All people with AD included in the study demonstrated adequate understanding of the study process and provided their own written consents.
Study Design and Data Collection Procedures
In total, 72 couples participated in concurrent in-person study sessions (60–90 min long) in separate rooms at baseline, in which they completed self-report questionnaires to report on perspective taking, support exchanges, health, and demographic characteristics. The study sessions took place in participants’ homes, or, if they preferred, in a family house on the UCD campus. They were then invited to complete additional semi-structured interviews to elaborate on couple communication and PLWDs’ needs, which were audio recorded and transcribed verbatim for qualitative coding (transcripts were not returned to participants). The two interviews were conducted on the same days or a few days apart depending on participant schedule. No data analysis was completed between interviews. The final sample for this study included 67 couples who completed all study components. Interviewers (RTT, MDH, JD, SH, EW, AC) were trained graduate and undergraduate students at UCD and had no prior relationship with participants. Participants were told the interviewers’ roles and purpose of the study.
We applied an explanatory sequential mixed methods design (Creswell et al., 2003) to address our aims. Quantitative and qualitative data were collected simultaneously, and the analysis of the quantitative data dictated our approach to developing a subsample and research questions for qualitative analysis. This sequence allowed us to use our qualitative data to explain processes underlying our quantitative findings.
Quantitative Data Collection
Perspective Taking
Caregivers self-rated their perspective taking using the partner version of the Interpersonal Reactivity Index (Péloquin & Lafontaine, 2010), which adapted the perspective taking subscale from the original index (Davis, 1983) to focus on couples. We omitted 3 items from the subscale to avoid fatigue and referred to spouses using their names, per participant preferences (Huo et al., 2024). Caregivers indicated how well each item described them. An example item is “I try to look at [spouse name]’s side of a disagreement before I make a decision.” Responses were coded from 1 (not at all) to 5 (a great deal). We calculated a mean score for perspective taking (α = .76).
PLWD Needs
PLWD and their spousal caregivers completed a modified version of the Camberwell Assessment of Need for the Elderly (CANE; Hoe, 2021). The original CANE assesses older adults’ needs in 24 areas, but to avoid fatigue and agitation, we removed areas that were (a) not relevant to or common in people with early dementia (e.g., deliberate self-harm), and (b) not applicable to our participants screened to be community-dwelling with their spouses (e.g., accommodation: whether the PLWD has an appropriate place to live). We kept 16 items in the assessment and divided them into three categories: physical, psychological, and social needs.
Physical needs included: self-care, eyesight, hearing, communication, mobility/falls, continence, physical health, and drugs. Eyesight, hearing, and communication were considered as one area in the original CANE, but we assessed them as separate areas of needs in this project. Psychological needs included: memory, psychotic symptoms, psychological distress, and behavior. Social needs included: daytime activities, information on condition and treatment, company, and intimate relationships.
Interviewers asked a series of probe questions for each area of need. Based on participant responses, interviewers determined in real time whether PLWD perceived having no need, met need, or unmet need in each area and whether caregivers perceived no need, met need, or unmet need in their spouses with AD. For example, to assess a caregiver’s perception of the PLWD’s need in mobility/falls, we asked whether the PLWD had trouble getting around or moving about home; how often the PLWD fell; what forms of walking assistance was the PLWD using (e.g., cane, assistive walking device, wheelchair); whether the PLWD felt the assistance was helping, and whether, even with assistance, the PLWD still felt they had poor mobility. Two trained research assistants independently coded need based on transcripts and audio interview recordings while blinded to interviewers’ original coding. Coding decisions were compared automatically using Excel functions and disagreements were resolved through weekly discussions. We compared across areas and calculated a sum score counting the number of areas where spousal discrepancies occurred (e.g., the PLWD reported no need in self-care but the caregiver reported met need in PLWD’s self-care).
Background Characteristics
We considered some background characteristics that might be associated with caregivers’ perspective taking and perceptions of PLWD’s needs. Caregivers reported background information for themselves and PLWD, including age in years, sex as 1 (male) and 0 (female), education in categories from 1 (less than high school) to 6 (post-college), physical health rated from 1 (poor) to 5 (excellent), and racial/ethnic identities recoded as 1 (racial/ethnic minority) and 0 (non-Hispanic White). Caregivers and PLWD self-rated the quality of their relationships with each other on a scale from 1 (not at all) to 5 (a great deal). The relationship quality items were taken from the Psychosocial and Lifestyle Questionnaire in the Health and Retirement Study (Smith et al., 2023). We replaced one item “how much does [spouse name] really understand the way you feel about things” with “how much does [spouse name] love and care for you” from the Family Exchanges Study (Fingerman et al., 2011) because the original item overlapped with perspective taking. We reverse-coded the negatively worded items and calculated a mean score for each participant (α = .74 for caregiver ratings and α = .83 for PLWD ratings).
Qualitative Data Collection and Sample
To capture couple communication about PLWD’s needs, participants responded verbally to a series of questions posed by an interviewer, and this discussion was audio-recorded. The prompts were modified twice during data collection to elicit more detailed responses. For example, we asked PLWD: “how do you think [spouse name] knows when you have needs? What do you typically do? What does [spouse name] do?” We also asked participants to describe times when caregivers did something helpful or when PLWD were not getting sufficient support as they would want. Caregivers completed corresponding questions reflecting on how they detected and responded to PLWD’s needs. We transcribed participant responses verbatim and de-identified the data for storage.
To capture distinct communication approaches in this dataset, we applied a subgroup parallel extreme case sampling design (Onwuegbuzie & Leech, 2007). Specifically, we examined couple communication among couples where caregivers reported the highest and lowest levels of perspective taking through the Interpersonal Reactivity Index described above. We developed the two groups: couples where caregivers self-reported an average score of (a) 4 or higher (top 33%) and (b) 3 or lower (bottom 29%) on the perspective taking scale. In total, 22 couples were identified for the high caregiver perspective taking group and 20 were identified for the low perspective taking group, allowing us to include 62% of the study caregivers in our qualitative analyses.
Data Analysis
We conducted preliminary analyses using descriptive statistics to describe the sample of 67 couples and compared the two subgroups of caregivers on select descriptive characteristics, and spousal discrepancies in perceived needs of PLWD.
For the hypothesis testing quantitative analysis, we examined how caregivers’ perspective taking was associated with spousal discrepancies in perceived needs of PLWD (i.e., the number of areas in which caregivers and PLWD disagreed on whether the PLWD had no need, met need, or unmet need). No background characteristics (e.g., age, sex, education) were associated with discrepancies in reports of needs, so we present bivariate correlations.
We then applied an inductive codebook thematic analysis to examine how PLWD and caregivers communicated about PLWD’s needs within couples in which caregivers reported (a) high perspective taking and (b) low perspective taking. Codebook thematic analysis was selected because it is well suited for efficient, applied, team-based qualitative research. This approach emphasizes the development of a shared codebook to guide analysis while allowing the research team’s interpretive engagement with the data to inform theme development (Braun & Clarke, 2022). The team consisted of three female researchers with complementary backgrounds: MH is a PhD-trained social gerontologist with expertise in empathy and couple relationships, ELM is a PhD-trained behavioral health researcher and gerontologist with expertise in qualitative methods and dementia-caregiving, and RTT was a MS student when the study was conducted with extensive experience in qualitative research. Together, the team identified the research questions that closely guided analysis.
We followed the six-phase framework for thematic analysis (Braun et al., 2023). First, RTT led a team of trained undergraduate research assistants (2 females and 2 males) to complete data familiarization through repeated reading of transcripts and memoing (taking notes of any observations). Second, RTT and research assistants conducted independent line-by-line coding of seven transcripts and then each coded subsets of transcripts from the sample to produce initial codes (i.e., small units of meaning). Coding was conducted using Microsoft Office (Word and Excel). Third, these initial codes and coded data provided a foundation for preliminary theme development; the team examined patterns in these codes to develop descriptions of the initial themes. Fourth, the team inspected additional transcripts to develop the individual themes and considered how themes were related. In this phase, the team examined similarities and differences in how themes were expressed across couples in each group (high and low perspective taking) to refine the scope and boundaries of themes. Both confirming and disconfirming cases were incorporated into the development of all themes. Fifth, the team applied the themes back to the data to ensure the final set of themes formed a complete picture of the findings. Exemplars from transcripts were incorporated into theme descriptions, with lengthy excerpts occasionally split and coded in conjunction with multiple themes. MH and ELM reviewed the preliminary themes and a subset of transcripts and provided feedback on the theme names, descriptions, and scope, leading to a final set of themes. Throughout the process, the team discussed code and theme development during weekly meetings to ensure that resulting themes captured patterned meaning across the dataset. Analysis indicated that thematic saturation was achieved, with later transcripts contributing additional examples but no substantively new ideas. Finally, we produced the analytic narrative and carefully selected exemplars to support our refined themes and address the study aims.
Results
Sample Descriptives and Within-Couple Comparisons
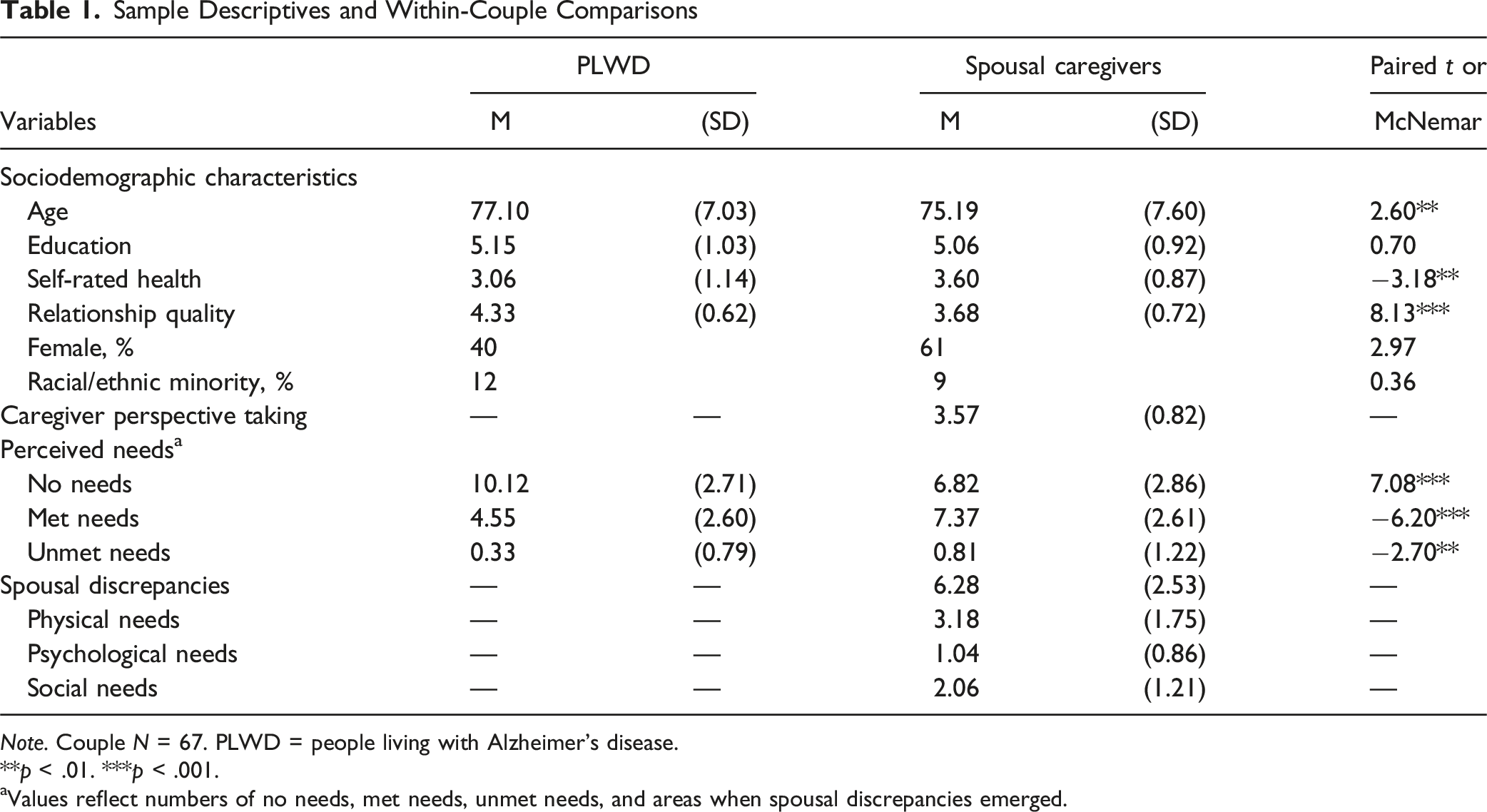
Note. Couple N = 67. PLWD = people living with Alzheimer’s disease.
**p < .01. ***p < .001.
aValues reflect numbers of no needs, met needs, unmet needs, and areas when spousal discrepancies emerged.
We found that greater caregiver perspective taking was associated with fewer areas of discrepancies in perceived needs (r = −.29, p = .019). Additional analyses for separate domains of needs showed that greater caregiver perspective taking was particularly associated with fewer areas of discrepancies in perceived psychological needs (r = −.35, p = .004).
Characteristics Comparisons Between Subgroups of Caregivers
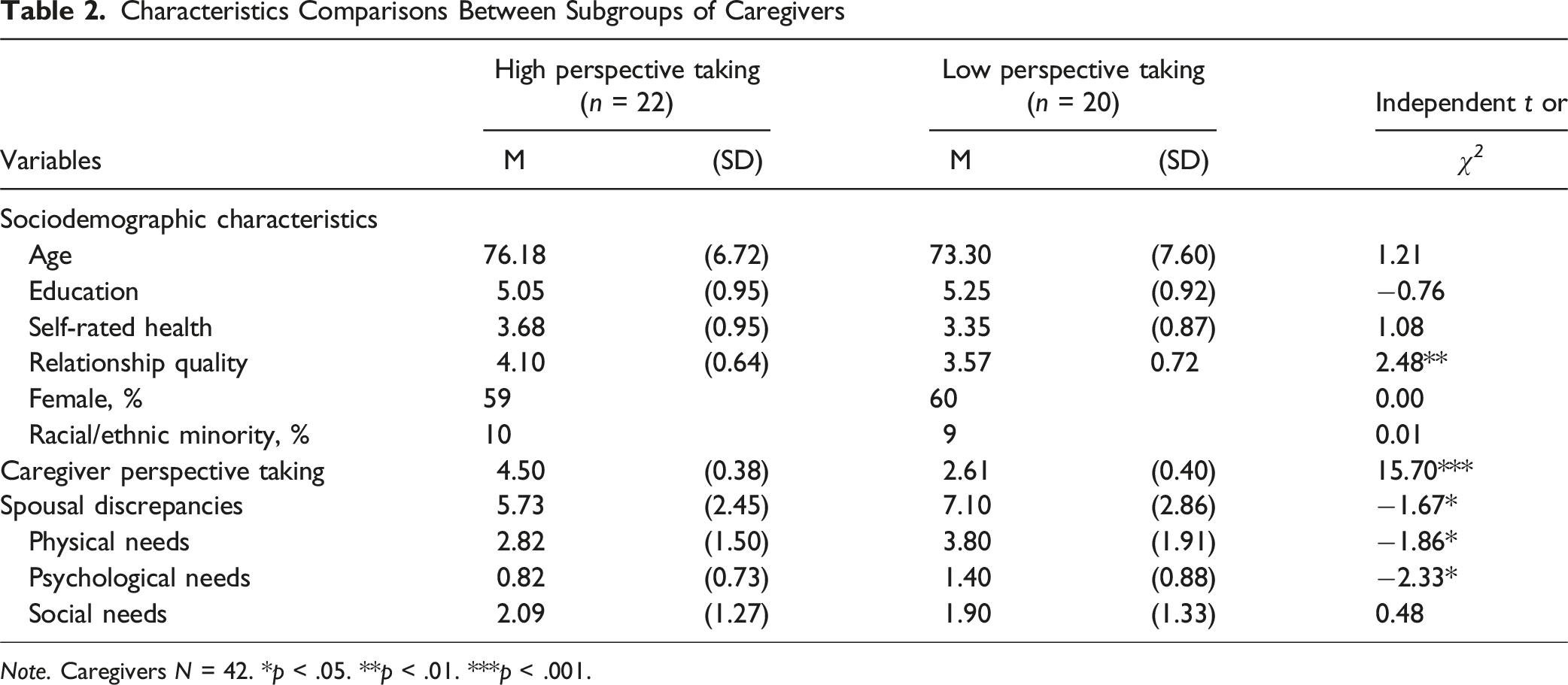
Note. Caregivers N = 42. *p < .05. **p < .01. ***p < .001.
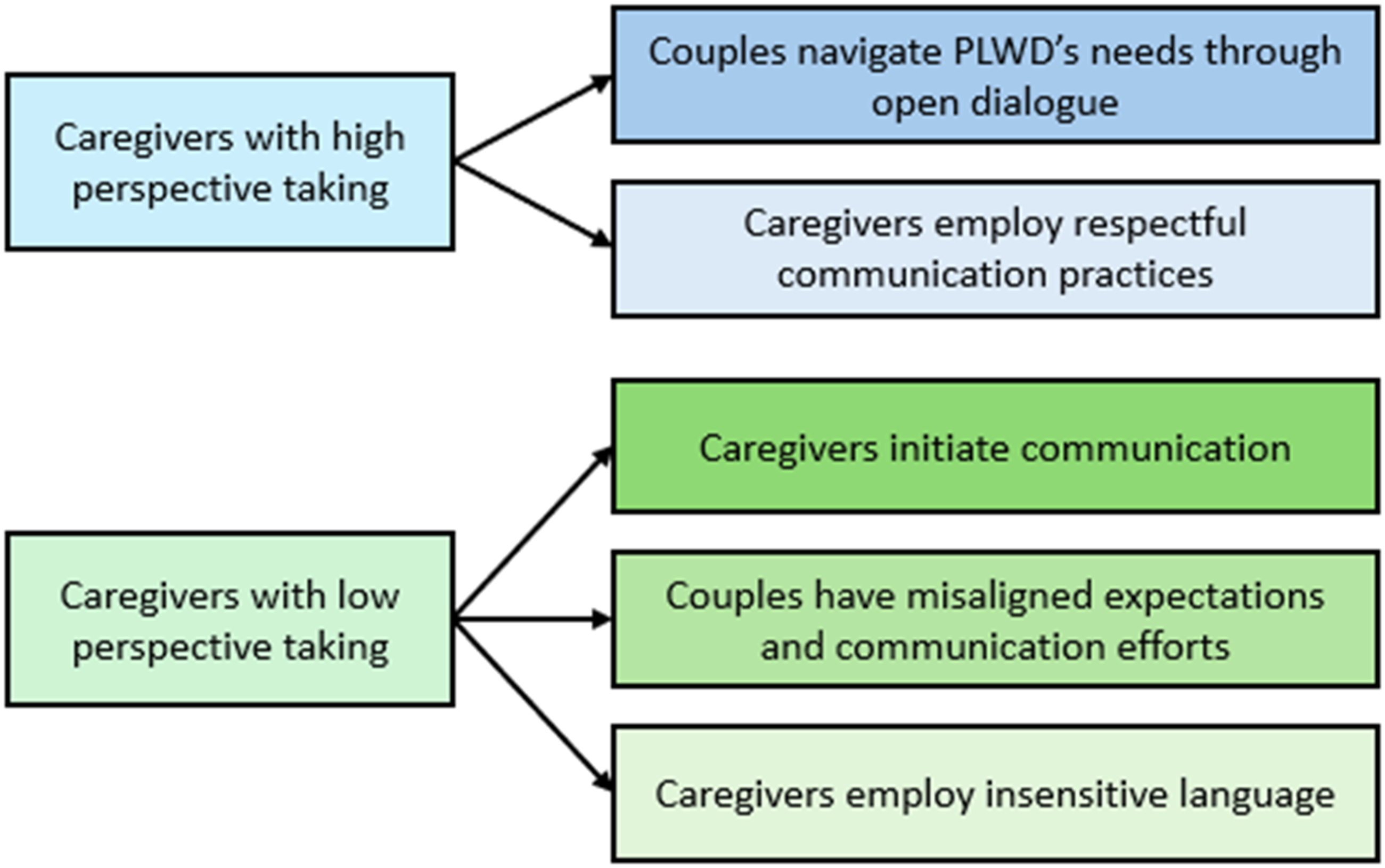
Themes and subthemes of communication patterns when caregivers reported high and low perspective taking
Couple Communication When Caregivers Reported High Perspective Taking
Two themes emerged describing how PLWD and caregivers in the high perspective taking subgroup communicated about PLWD’s needs. These themes revealed how: (1) couples navigated PLWD’s needs through open dialogue and (2) caregivers employed respectful communication practices.
Couples Navigate PLWD’s Needs Through Open Dialogue
Some couples discussed that they engaged in direct, collaborative conversations about PLWD’s needs and how to deal with those needs together: “We don’t keep secrets from each other, and I think that’s important. Have open communication.” While the tone and examples varied across couples, most of them highlighted open communication and joint problem-solving, in which neither party reported feeling bothered or upset. PLWD felt comfortable voicing their needs and opinions to caregivers, for example, “If I have a need, I let her [caregiver] know.” and “If I have pain, I tell her [caregiver].” Many PLWD described how they requested help explicitly should needs arise and had “no problem asking.” They felt assured that their needs would be addressed, as demonstrated by a PLWD who explained that she had “no problems saying I need this” since knowing “he will help me with whatever I want.”
Caregivers’ responses confirmed the presence of open dialogue about PLWD’s needs. Some caregivers expressed confidence that “I think if he [PLWD] felt any, any kind of problem…he would communicate it with me.” Caregivers also took initiative in identifying PLWD’s needs, such that some discussed if they thought something was wrong, they would go directly to PLWD and ask, “is there something wrong?” This kind of inquiries, according to a PLWD, made her “feel that he’s [caregiver] aware of it and tries to be supportive.” Further, caregivers actively engaged in conversations to further understand PLWD’s needs. For example, a caregiver described how “for the most part, he [PLWD] verbalizes or comes close to verbalizing what’s bothering him.” but she also mentioned that when her husband was having a not so good day, she would “pry out of him what his problem was.”
Caregivers Employ Respectful Communication Practices
Caregivers in this group also tended to adapt their communication approaches, such as by using supportive inquiries to facilitate PLWD disclosure. When trying to learn about PLWD’s needs and struggles, caregivers used probing questions that tended to encourage PLWD to share their thoughts, for example, “what can I help you with? How you doing? If you have any trouble, can I help you with anything?” A PLWD mentioned if his wife thought he was sad, “she’d come up and say ‘I’m sorry, what’s wrong with you?’”
It is worth noting that both PLWD and caregivers discussed how caregivers showed attention to PLWD’s distress and reassure PLWD that they were no burden. A PLWD acknowledged, “he’s [caregiver] already made it quite clear he’s not going anywhere. You know, he said ‘I’m here for you and, you know, this is not going to drive me away.’” A caregiver also emphasized how “it’s not important from the physical side as much as it is emotionally for her to know that she’s loved, cared, wanted, and that I still care enough that I would want to be close to her.”
Couple Communication When Caregivers Had Low Perspective Taking
Analysis also revealed three themes describing couple communication when caregivers had low perspective taking. The communication (a) was often initiated by caregivers, (b) reflected misaligned expectations and communication efforts in couples, and (c) involved caregiver language that might be insensitive towards PLWD. Examples of misaligned communication efforts and insensitive language are presented descriptively and should be interpreted in the context of caregiving demands and constraints.
Caregivers Initiate Communication
Some couples engaged in direct and supportive communication, which was primarily initiated by caregivers. PLWD were responsive and willing to disclose needs once asked but they were unlikely to initiate the conversation themselves. Instead, caregivers relied on observation, intuition, and nonverbal cues to identify potential needs in PLWD. For example, caregivers indicated that their spouses did not verbalize their needs, but they “can sort of tell his [PLWD] body language” or “try to take cues.” PLWD also agreed with their caregivers were “observant and attentive.” When a PLWD was asked how her husband caregiver knew when she was not feeling well, she said, “he [caregiver] reads my mind. I have no idea. He does know…He knows me better than I know myself.” At times, caregivers also prompted PLWD with questions such as “you want me to come in and help” or more direct inquiries like “do you need to pee? do you need to poop?”
Couples Have Misaligned Expectations and Communication Efforts
Couples described differing views regarding the recognition of needs and support behaviors, with the PLWD reporting little to no need and the caregiver feeling overwhelmed by caregiving demands. The ways they voiced their grievances often led to contentious exchanges. A caregiver explicitly stated, “I don’t have any trouble expressing what I think her needs are. We just have a problem agreeing on whether she has that need or not.” Even when needs were clear, couples described sometimes not being on the same page regarding how to address those needs, creating frustration on both sides. Although conflicts varied case by case, some of the misunderstandings appeared to originate from longstanding patterns in their relationship histories. For example, a PLWD pointed out that “he [caregiver] just doesn’t really know how to comfort me.” Whereas the caregiver felt uncertain, “I try. Sometimes it helps, sometimes, she [PLWD] says, I’m making it worse.” Another PLWD stated, “I don’t think it’s ever something that I recognize that she had to help,” whereas according to the caregiver, “communicating with him [PLWD] really, wear me out, the whole caregiving wears me out.” In another couple, both parties seemed to attribute issues to each other’s ingrained traits they saw as resistant to change, the PLWD expressed, “I would like to be closer to [caregiver] so that I could turn to him, but I can’t really. I mean, he’s there and he’s just not warm and fuzzy.” Yet, the caregiver in this couple said, “she [PLWD] gets grumpy and angry. She focuses on, you know, where objects are sitting. What’s it called? OCD kind of thing. Gets very obsessive and compulsive and everything has to be right now. She makes a big deal out of nothing kind of stuff. And she’s not very nice.”
Caregivers Employ Insensitive Language
Some participants (both caregivers and PLWD) described instances where caregivers focused on memory recall or correction, using phrases like “remember?” or “I’ve told you that already,” rather than offering simple-to-follow guidance or support. This approach prioritized being right over understanding the PLWD’s perspectives, and correction over redirection, with caregivers expressing their frustration openly. In fact, the word frustration was brought up by many caregivers during their interviews, ranging from passive-aggressive comments to more overtly harsh or demeaning remarks. For example, a caregiver described how, after responding to the same question multiple times, he started adding “you know, it’s the fourth time in less than five min.” A PLWD described how sometimes her caregiver would say things like “why don’t you remember that we just saw that blah blah blah.” Another PLWD shared some comments they have received from the caregiver, “you can’t hear nothing. I told you to take care of it. You can’t remember nothing.”
Discussion and Implications
A growing body of research has examined interventions designed to enhance caregivers’ perspective taking, but outcomes have focused primarily on caregivers’ experiences and health (Au et al., 2020; Jűtten et al., 2019; Wijma et al., 2017). The current study extends this burgeoning literature by utilizing a mixed-methods approach to examine how caregivers’ perspective taking affects their perceptions of the needs of spouses living with AD.
Consistent with prior research (Monin et al., 2020; Wammes et al., 2024), significant within-couple discrepancies exist between self-reports and caregivers’ proxy reports of PLWD’s care needs. We found that spousal caregivers tended to identify fewer areas in which PLWD reported no need and more areas in which met and unmet needs were present. This finding does not necessarily reflect caregivers’ misperceptions; rather, PLWD may face challenges in recognizing their needs due to cognitive impairment or reduced self-awareness in AD. In this context, caregivers’ broader recognition of PLWD’s needs may be protective and enable them to anticipate potential risks. While PLWD’s perspectives remain essential for person-centered care, engaging both PLWD and caregivers provides a more holistic view of AD care needs and strategies to address those needs.
It is noteworthy that participants in our study identified low rates of unmet needs among PLWD, which is in line with prior research relying on self-reports and caregiver proxy reports (Monin et al., 2020). These findings, however, do not necessarily indicate a low prevalence of unmet needs. Studies (e.g., Black et al., 2019) drawing on comprehensive clinical-administered tools that include in-home assessments and environmental observation in addition to interviews may be more sensitive to unmet needs that PLWD or caregivers may not recognize or prioritize themselves. Also, because PLWD in our sample were in the early stages and able to provide self-reports, our findings may reflect the perspectives of relatively better functioning PLWD.
Our quantitative data revealed that greater caregiver perspective taking—a malleable ability that can be enhanced—was associated with fewer areas of discrepancies in perceived needs of PLWD across members of the dyad. This observation is synergistic with prior concept analysis that linked perspective taking to caregivers’ congruent perceptions of care recipients’ illness experiences (Lobchuk, 2006) and confirms perspective taking as a viable intervention target to promote congruent appraisal of AD within the dyad. In other words, based on our findings, we assert that perspective-taking interventions may support alignment between dyads’ perspectives of PLWDs’ needs, ultimately allowing caregivers to better identify and meet these needs. Indeed, this study offers empirical evidence to extend the heterogeneity of dyadic appraisal that has been illustrated in the theory of dyadic illness management (Lyons & Lee, 2018). Research has primarily focused on variation by symptom severity and distress, but our study extends the work by identifying caregiver perspective taking as a key malleable antecedent of dyadic appraisal that is central to optimizing cooperative illness management efforts and health.
Some existing perspective-taking interventions are promising candidates to use to address these outcomes within dyads. For example, researchers recently established the efficacy of a photo-captioning caregiver intervention, whereby caregivers take photographs of the PLWD each day and caption them from the perspective of the PLWD, for improving caregiver perspective taking (Mroz et al., 2025; Rilling et al., 2024). A secondary analysis of caption content revealed that those caregivers who experienced the highest empathy gains wrote captions that captured the everyday intentions of PLWD, as well as their strategies to overcome personal challenges (Mroz et al., 2025). By writing captions in these ways, caregivers may gain a deeper understanding of PLWDs’ daily interactions with their environments, thereby gaining more context about PLWDs’ needs.
Further, we relied on qualitative interview data to derive themes describing communication among couples in which the caregivers reported high perspective taking and those with caregivers reporting low perspective taking. Our analysis of couple communication extends existing perspective taking literature that has primarily examined broader relationship patterns such as overall marital quality (Cahill et al., 2020) by delineating pathways through which caregiver perspective taking affects spouses’ perspectives, and the concordance of those perspectives, of the needs of PLWD. When caregivers reported high perspective taking, both caregivers and PLWD described collaborative communication to identify and address PLWDs’ needs. Caregivers expressed confidence that PLWD would communicate with them whenever needs arise, but they also described actively reaching out to PLWD to clarify needs. PLWD, in turn, felt comfortable turning to caregivers for assistance and believed that their caregivers would help with whatever they needed.
In contrast, we observed largely unilateral efforts to communicate about needs when caregivers reported low perspective taking. That is, caregivers in this group described often interpreting nonverbal cues to identify needs in their PLWD. Such efforts can obscure perceptions of needs and elicit recurring conflict that fosters further disagreements and perpetuates a cycle undermining dyadic illness management. However, we speculate that these patterns may reflect, in part, differences in how caregiving conversations unfold under varying levels of caregivers’ perspective taking and caregiving context. While caregivers with high perspective taking tended to show care and encourage PLWD to disclose needs, caregivers with low perspective taking often expressed frustration during these conversations, which may hinder the disclosure of needs or even general communication. It is not uncommon for caregivers to adopt a critical or aggressive communication tone (Leggett et al., 2019), particularly if they have not received communication skills training or had experience communicating with PLWD in the past. As such, our study underscores the value of communication training programs, along with the caregiver perspective taking intervention mentioned above, in supporting both parties to develop constructive habits for self-expression, expression of challenges, and identification of needs. Notably, these findings are intended to identify areas where additional resources may be needed, rather than to evaluate caregivers’ intent.
Limitations
This study relied on self-reported and interview data that described each spouse’s perspective on couple communication, which limited our ability to capture linguistic features such as caregivers’ tone when speaking to PLWD. Future research should use observational data to offer additional insights into how couples communicate about PLWD’s needs. Additionally, we required a clinical diagnosis of AD during recruitment, which likely led to a sample with low diversity because individuals from racial/ethnic minority groups are less likely to receive timely diagnosis of AD (Tsoy et al., 2021). Despite the heterogeneity that we observed in couple communication, we acknowledge that this study may have presented a more positive view on couple relationships in AD. Prior research suggests that couples participating in dyadic studies tend to report better relationships and well-being than individual participants (Barton et al., 2020). This study is cross-sectional in nature and the qualitative component was descriptive, so our findings do not infer causality. Longitudinal research is needed to understand how caregivers’ perspective taking affects couple communication and perception of needs in the context of progressive cognitive decline.
Conclusion
The current study characterizes couple communication about PLWD needs and identifies additional benefits of perspective taking as couples jointly cope with mild to moderate AD. While existing interventions have primarily focused on promoting caregiver health, we present empirical evidence linking caregivers’ perspective taking and their perceptions of PLWD needs—a central feature of high-quality caregiving—and delineating how dyadic processes may underlie the benefits. Findings help us identify the risk and resilience of dyadic communication in caregiving couples and leverage perspective taking interventions to promote dementia care.
Footnotes
Acknowledgments
We want to thank all couples participating in the Dyadic Study on Empathy in Caregiving and undergraduate research assistants from the UC Davis Social relationships, Health, and Altruism REsearch (SHARE) lab who helped with interview transcription and qualitative coding. We thank Rose T. Tran, Misha D. Haghighat, Joyce Do, Sophie Huang, Evelyn Wong, and Ashley Covarrubias for conducting participant interviews and assisting with data collection.
Ethical Considerations
The Institutional Review Board (IRB) Committee at University of California, Davis approved our interviews (approval: 1531955) on July 26, 2021.
Consent to Participate
Participants (both people living with Alzheimer’s disease and their spousal caregivers) gave written consent for review and signature before starting interviews.
Author Contributions
Meng Huo planned the study, performed quantitative analyses, supervised qualitative coding, revised qualitative codebooks, and wrote the paper. Emily L. Mroz helped to plan the study, guided qualitative coding, validated and revised qualitative themes, and revised the paper. Rose T. Tran conducted qualitative coding, wrote the initial draft of themes, and revised the paper. Oanh L. Meyer contributed to the original study design and revised the paper. Karen S. Lyons provided critical revisions to the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging under Grants R21AG069045-01A1, P30 AG072972, and K22 AG088144-01.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All de-identified data, analytic methods or materials can be made available to other researchers for replication purposes. Please contact the corresponding author for details.