
Abstract
Background
Caregiving for a spouse living with Alzheimer's disease and related dementias (ADRD) is incredibly stressful, which puts caregivers at risk for developing health problems themselves.
Objective
To develop an intervention that supports caregivers and helps mitigate the stress associated with caregiving.
Methods
In Part I, we used qualitative methods (e.g., data collected via focus groups with people caring for a spouse living with ADRD) to identify opportunities for targeted treatment and potential barriers to a cognitive-based online expressive writing (EW) intervention tailored to spousal caregivers. In Part IIa, we conducted a second wave of focus groups, throughout which we iteratively adapted a mobile app-based writing intervention for stress and grief among spousal caregivers, while continuously monitoring caregivers’ perceived acceptability and feasibility of each proposed feature. Finally, to prepare for app development, we conducted preliminary usability testing (Part IIb), during which caregivers interacted with a prototype of the future app to complete a number of proposed task flows.
Results
Caregivers reported having dynamic needs and requested an intervention that was efficient, mobile, and readily accessible. Further, people caregiving for a spouse living with ADRD have specific motivations for writing (e.g., needing an outlet to release their emotions) as well as unique barriers to the intervention (e.g., lack of time, security concerns).
Conclusions
A mobile-based writing intervention catering to the specific needs of these individuals may be a helpful coping resource for caregivers.
Introduction
Nearly seven million Americans aged sixty-five or older are living with Alzheimer's disease. 1 This number is only expected to grow in the coming decades as the population ages. Further, Alzheimer's disease and related dementias (ADRD) are a top contributor to disability and mortality later in life; indeed, one in three older individuals dies with a diagnosis of ADRD. 1 The responsibility to care for people living with ADRD often falls on an individual's spouse. Spousal caregivers reflect 60% of overall caregivers, who often provide continuous care for their spouse without adequate respite. 1
ADRD caregiving is often an extremely stressful and drawn-out process, lasting a median of 7 years from age at onset—though this period may last anywhere from 4 to 8 years according to recent estimates. 2 This span of time serves as a period of “living bereavement,” or a time of grieving the loved one an individual once knew before the onset and progression of ADRD symptoms. 3 Caregivers for a spouse living with ADRD live with an often-ambiguous disease trajectory and a sense of confusion about when life really ends with their loved one, 4 which may make it more difficult for them to process their emotions related to the loss. Further, differing types of dementia present different symptoms, thus posing unique challenges to one caregiver relative to another.
In addition to the emotional toll of caregiving, the cumulative burden of daily stressors (e.g., medical costs, interpersonal conflict with their partner, lack of caregiving resources) 5 can also take a toll on caregivers’ own health. Indeed, caregivers aged 65 and older are more likely to experience chronic conditions themselves, such as hypertension, arthritis, and heart disease, compared to spousal caregivers of individuals without ADRD. 6 Further, the stress associated with caregiving puts spousal caregivers at a higher risk for mental health issues (e.g., depression) and reduced overall quality of life. 7 More broadly, the risks are especially concerning for caregivers who report high levels of strain, as they are at a greater risk of mortality than their non-caregiving counterparts. 8 Thus, developing interventions that support this population and help mitigate the stress associated with caregiving is critical.
Research on ADRD spousal caregiving interventions has identified cognitive behavioral therapy (CBT)-based programs as an effective way to reduce stress and depressive symptoms among caregivers. 9 Cognitive-behavioral programs specific to grief include methods such as exploring dysfunctional thoughts, questioning automatic irrational thinking, enabling positive memories of the spouse with ADRD, formulating a new identity and activating social support networks. 10 However, these programs often require one-on-one therapy with a certified mental health counselor, which can be expensive and difficult to implement. 11 Further, the accessibility of CBT is limited for many caregivers, especially those who face barriers to accessing traditional forms of mental health care. 12
Expressive writing (EW) programs, on the other hand, can be conducted without a mental health counselor, and have been shown to be effective in improving people's health. 13 Early EW programs had the sole intention of providing an outlet for people to express their emotions. 14 EW can improve self-regulation of physiological responses, emotional experiences, and behaviors, which thereby lead to better physical and mental health outcomes, 15 especially among people who have experienced stressful life events (e.g., caregiving for a spouse with ADRD). More recently, researchers have found that EW interventions that include more structured and directed components seem to work better for grieving individuals. 16 Importantly, researchers can integrate components of CBT into EW prompts contained in online interventions to further enhance EW's efficacy. 17
EW is associated with a myriad of improved health benefits, including reduced stress and depression, after other loss-related experiences (e.g., marital separation from a spouse), particularly when participants are asked to cognitively restructure or create a coherent narrative of their relationship loss experiences. 18 In a writing study among family caregivers of physically frail and cognitively impaired older adults, those who wrote objectively about how they spent their time experienced more mental and physical health improvements than comparison groups. 19 One study even found that older adults who wrote about upsetting life events demonstrated improved physical wound healing compared to those who wrote about everyday topics. 20 However, to our knowledge, no EW interventions exist that incorporate evidence-based tools such as CBT and are specifically tailored to spousal caregivers of people living with ADRD. Given that the often-prolonged caregiving process can be described as a period of “living bereavement,” we turn to the bereavement and EW literature to consider how we might utilize EW to support spousal caregivers in the form of an online EW intervention.
Results of using EW interventions among bereaved samples are mixed, likely due to many of these studies lacking a direct focus on writing but rather asking people to express their deepest thoughts and feelings in general.21–24 However, more structured and directed interventions appear to work better at improving outcomes among the bereaved. For example, bereaved participants who engaged in directed writing that focused on sense-making or benefit-finding (both associated with adjustment to loss) reported improved prolonged grief disorder, depressive, and post-traumatic stress symptoms 3 months post-intervention. 19 Different forms of EW have been recommended as a method for supporting caregivers of those with ADRD. 25 However, few studies have empirically developed EW interventions specifically for caregivers of a spouse living with ADRD. Specifically, acceptability and feasibility of EW interventions among this population is still unknown. A virtual EW intervention may be one alternative format through which we can deliver facets of CBT to caregivers in an accessible, convenient, and supportive way, providing a possible solution to the feasibility and cost barriers associated with conducting traditional CBT.
Methods
Participants and design
This study draws on the Discover, Design & Build and Test framework which centers users’ experience and feedback in the development and design of a health intervention and uses qualitative methods to collect and analyze information throughout the process.26,27 This research was approved by the Institutional Review Board at Rice University and completed in accordance with the Helsinki Declaration of 1975. Twenty-seven participants (20 female, 7 male) who were caregiving for a spouse living with ADRD participated in this intervention development study; 92.9% identified as White, 3.5% as Black/African American, and 3.6% identified as more than one race. Additionally, 3.6% of participants identified as Hispanic/Latinx. This caregiving sample was made up of participants from 7 states in the U.S. (i.e., Texas, Oklahoma, New York, Arkansas, Tennessee, Oregon, and Wisconsin). Our sampling procedure used a combination of criterion 28 and convenience sampling. 29 We used criterion sampling to select individuals who were caregivers of spouses with ADRD. Convenience sampling was used to recruit thirteen of our participants, who were drawn from a caregiver database from a collaborators’ NIA R01 study conducted in Houston, TX. 30 These caregivers participated in this previous study between 2020–2024. To recruit for this current study, we contacted caregivers in waves between June 2023 and April 2024 to share information and invite participation in focus groups. Caregivers were only contacted after their participation in the collaborator's study had concluded. Participants in the R01 project already met the following eligibility criteria: (1) self-identify as the principal person taking care of the spouse with a physician-based diagnosis of ADRD, (2) devote at least four hours of daily care to the spouse for at least the last three months, and (3) have been married (or self-defined as long-term committed partner) to their spouse living with ADRD, for at least three years. Notably, we did not exclude caregivers who had engaged in some form of writing before (e.g., journaling, expressive writing, note-taking), and were naive to the proportion of caregivers with previous writing experience, at the time of recruitment. To reduce the likelihood of bias (i.e., that participant feedback may be influenced by previous relationships with the research team or a related project), we also recruited 14 new participants between June 2023 and April 2024. A nationwide community outreach method was utilized for this purpose, beginning with “cold calls” to organizations that may have access to people caregiving for a spouse living with ADRD. 30 After hearing about the study from one of these organizations, interested participants completed an eligibility screening over the phone. These participants were required to meet the same eligibility criteria as those recruited from the collaborator's database. Then, eligible participants completed a medical release form, which the research team then faxed to their spouse's doctor's office. Once the team received written confirmation of their spouse's diagnosis via fax, participants were scheduled for an online information session with a member of the research team, who guided them through the informed consent process and told them what to expect during the focus groups. After the information session, participants engaged in at least one 90-min focus group, moderated by the senior author and a research assistant via Zoom. 31
Conducting focus groups
In order to create a more intimate group setting that would encourage open and comfortable dialogue, as well as better support more meaningful participation from all group members, we limited each group to 4–6 participants. 32 The senior author of this article moderated all focus groups, following focus group guides designed by the research team (see the Supplemental Material).
We structured focus groups to unfold in 2 “waves,” with each wave convening 4 separate focus groups. Our aim for Wave 1 of the focus groups was to determine whether the intervention idea was desirable and feasible for caregivers. We assessed this aim by asking participants to discuss their interest in EW as well as opportunities that EW might provide. In contrast, we also asked caregivers about their concerns related to the intervention, as well as challenges and potential barriers they could anticipate facing if asked to engage in an online EW intervention (see the Supplemental Material [S1-S2] for Focus Group Interview Guides).
Wave 2 focus groups asked participants to provide their feedback on more specific components (e.g., actual writing topics/prompts) we created based on existing EW interventions for stress, grief, and ADRD familial caregiving,16,33,34 as well as existing components of EW interventions specific to grief, which also integrate cognitive behavioral components. 10 In addition, we asked about their preferences for writing reminders (e.g., push notifications), the features and aesthetics of writing screens within the app, having access to a writing timer, having an ability to take brief “notes” in between writing sessions, and comfort with varying levels of security and data sharing. To follow up with previous focus group participants from Wave 1, as well as gain a fresh perspective from people unfamiliar with the idea of an EW intervention for caregivers, Wave 2 included two focus groups comprised of returning participants from Wave 1, as well as two focus groups of new caregivers who were unaccustomed to the intervention. Previous participants were organized into Wave 2 groups 1 and 3, and new participants were organized into Wave 2 groups 2 and 4. At the beginning of Wave 2 focus groups, we shared with participants the results of our qualitative analyses from Wave 1. Between each focus group of Wave 2, our product designer applied principles for designing and conducting iterative qualitative research, to analyze participant feedback and refine wireframe designs and focus group questions. Notably different than Wave 1 focus groups, we iteratively updated Wave 2 focus group stimuli (e.g., wireframes of app designs), based on feedback from the previous focus group (see the Supplemental Material [S2a-d]). Focus groups were audio recorded, transcribed verbatim, and de-identified.
Qualitative analysis of wave 1 and 2 focus group data
We analyzed the transcripts of Wave 1 focus groups to consider general group sentiment and common thinking about the desirability and feasibility of an EW intervention. To analyze focus group data, we conducted content analysis,35,36 without preconceived categories or a priori codes. 37 We used two independent coders to ensure data integrity and reduce the likelihood of interpretation bias. For each wave of focus group data, these two trained coders (co-authors on this paper) independently studied (i.e., repeatedly read) focus group transcripts to achieve immersion and obtain an overall sense of the content. 38 Then, the coders made notes of their first impressions of the data. Next, the coders used inductive category development, 39 highlighting the exact words from the text that appear to capture key thoughts or concepts. Codes emerged that were reflective of more than one key thought. Then, codes were sorted into categories, which were organized into meaningful clusters. 40 At this point, the senior author met with the two independent coders to discuss the themes, and helped determine the point of data saturation (i.e., when the codebook was applied across all focus group text segments, and no new themes emerged. 41 In parallel to the method conducted by the academic research team (reported, above), our industry-based product designer independently conducted affinity diagramming with the focus groups data. Affinity diagramming is another data synthesis technique commonly used in the field of product design, which helps identify patterns, connections, and themes to aid in product design-related decisions. 42 After both types of data analysis were conducted for each wave of focus group data, the senior author met with the product designer to identify points of convergence between the results of the content analysis and the results of the affinity diagramming. Across these two methods, the results revealed insights into key user needs (e.g., security features, flexible writing schedules, flexible writing options) that informed the design of the digital intervention product. These insights were then used to create wireframes to present content to participants in Wave 2 and evaluate the design's effectiveness (e.g., ease of use, perceived security, most important features).
Usability testing
Following the completion of Wave 1 and 2 focus groups, we conducted a round of usability testing to evaluate how users interact with the app prototype. Usability testing is a common next step in iterative product development and is used to assess the intuitiveness and functionality of a design, uncover areas of confusion, and refine the user experience. 43 Accordingly, in the current study, we aimed to evaluate how easily participants could complete key tasks, how they interpreted the app's layout and content, and whether any usability issues surfaced.
We invited back n = 5 of the previous focus group participants to engage directly with a prototype of the EW app for caregivers. These usability testing sessions were conducted with one participant at a time, led by two of the co-authors on the paper—a graduate student and the product designer for the app prototype. We used two established usability data collection methods: 43 the “think-aloud” method and semi-structured interviews. The combination of these two methods has been successfully applied in recent digital health studies. 44 Before beginning testing, we asked participants to pretend they were caregivers participating in a writing intervention program. Reading from a script, we set the stage, explaining the circumstances in which participants could imagine they were engaging with the app (see the Supplemental Material, Usability Test Plan Script [S3]). Then, participants were asked to complete a series of predefined tasks while narrating their thoughts and reactions aloud (i.e., the “think aloud” method): (Task 1) complete a writing session using a writing prompt, (Task 2) make a “note”, and (Task 3) complete a writing session from a note. Task 1 was selected because it is essential to facilitate an online EW program. Tasks 2 and 3 were selected specifically to test the app's Notes feature, which was identified as an essential component for the acceptability of the intervention by a significant percentage of focus group participants. To simulate the experience of a caregiver using the app at home, we limited our guidance during the task flow testing. Prior to testing, we established four markers of success: (1) the length of time to complete a task, (2) the number of users who completed the task fully, (3) participants’ verbal narration during the session, and (4) observational cues such as body language, hesitation, and facial expressions. During analysis, we added a fifth metric, whether the participant required assistance to complete the task, as this proved useful in understanding how participants progressed through the experience after encountering obstacles. After each task, we conducted a semi-structured interview to gather deeper reflections on the app's layout, how participants interpreted individual elements on the screen, what they liked, and what they felt could be improved.
Last, we conducted a focused preference test on one key visual element on the home screen: the progress indicator. Caregivers had emphasized the importance of feeling oriented and knowing where they were in the 8-session writing series, making this a critical design feature. To evaluate which design best supported this need, we showed participants two versions of the home screen—one with a progress circle, the other with a progress bar (Figure 1). All other elements remained identical to isolate the difference. We asked participants which version they preferred and why. As a final step, we synthesized user responses by reviewing behavioral patterns and participant comments by task and screens, allowing us to prioritize common usability issues.
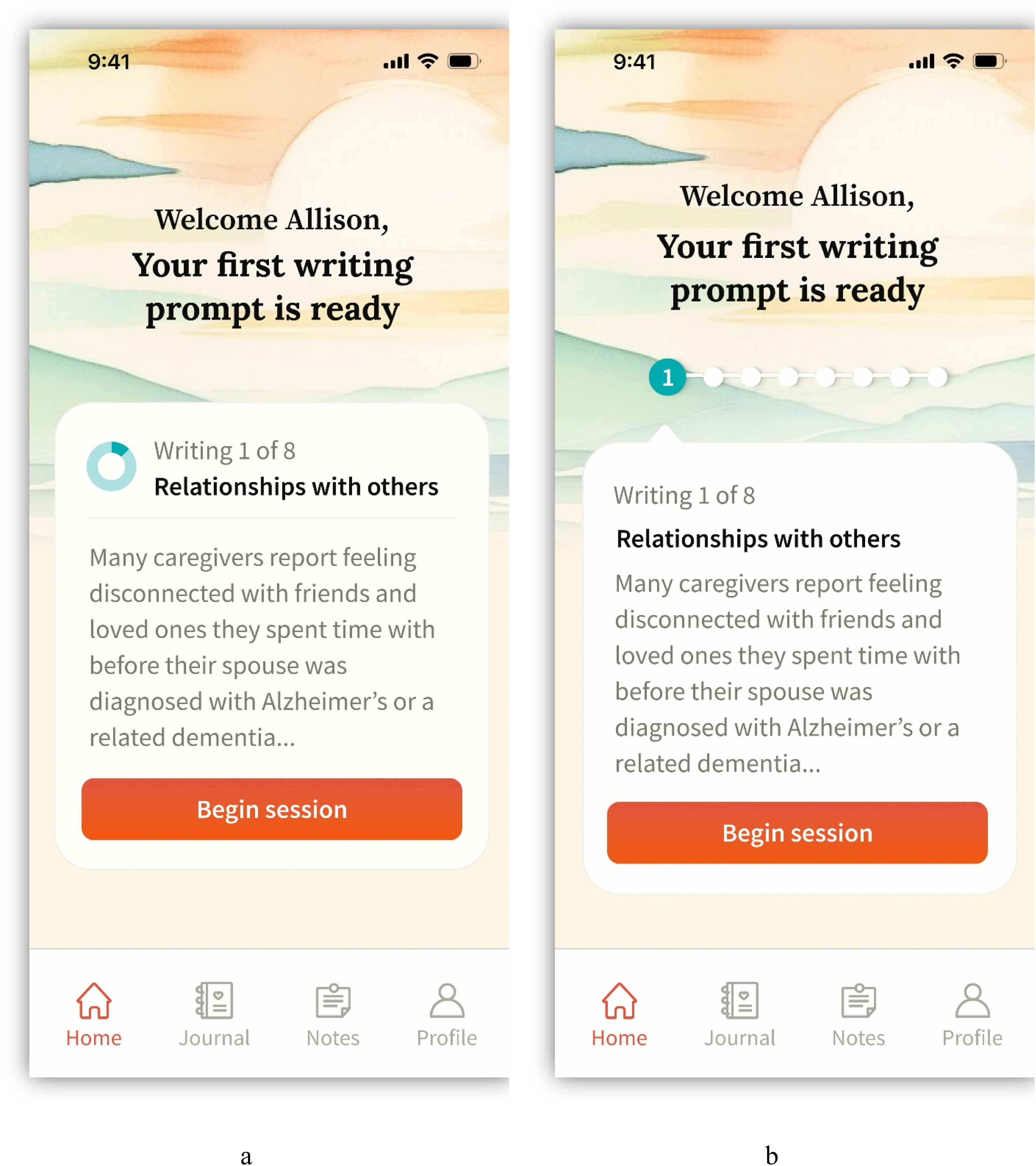
Home screens shown to participants during usability testing. Panel a is the starting point for all task flow testing. Panel a and b are identical, except panel a uses a progress circle indicator while panel b uses a progress bar.
Results
See Table 1 for an overview of themes derived from qualitative analysis of focus group data, across Waves 1 and 2.
Overview of themes identified across waves 1 and 2 focus groups.
Wave 1 focus group results
Using content analysis, we identified, described, and interpreted key patterns and themes among caregivers’ responses to our semi-structured set of focus group questions (see the Supplemental Material [S1]). We did not explicitly ask participants if they had ever engaged in a form of expressive writing before. However, 13 (48%) caregivers did report writing, in some form (e.g., journaling, keeping a record of objective notes / observations of their spouse through the disease progression), either previously, or on a regular basis, while others had little-to-no writing experience. Thus, while themes and quotes below reflect caregiver's attitudes about writing, these themes should be interpreted with consideration for participants’ varying levels of writing experience. Below, we summarize these themes as well as corresponding quotes extracted from the de-identified Wave 1 focus group transcripts.
Acceptability of an expressive writing intervention
Openness to writing
Many caregivers expressed openness to engaging in an EW program if it could positively impact their lives and help them find meaning in difficult caregiving-related experiences. For example, some hoped that writing may serve as a source of motivation and encouragement to continue onward, despite hardships.
“… maybe the writing could help you in some ways reflect on what the positive things have been that day to help you boost along a little bit …”
-Speaker 4, Focus Group A
The degree of caregivers’ openness to writing varied and was often impacted by whether the person had previous experience with writing in different forms (e.g., journaling, creative writing, note-taking). Most caregivers who already engaged in some form of writing, either currently or in the past, reported finding writing to be helpful; these avid writers were very open to the idea of engaging in an EW program– many even delighted at the idea.
“I’ve been journaling. I'm in lot of grief … I do a joy box and I try to write … something that I found joy in for the day and put it in that box and next year I wanna read all of that. Writing three times a week [wouldn’t] be a problem for me. I'm overjoyed [at the idea of] getting to do that.”
-Speaker 2, Focus Group C
Several caregivers reported using writing as a tool for keeping track of their spouse's disease progression, but not necessarily using writing to express how they felt about the events. Instead, they wrote to help stay oriented to where they were in the caregiving journey and to serve as a reference when sharing about their spouse's condition to family, friends, and medical providers.
“I write down facts … then I process internally … if there's something significant, I’ll write that down. But that's just so I can tell the doctor … [write] about how I felt? No.”
-Speaker 1, Focus Group B
“… if my son calls me who lives two thousand miles away … if he calls me and says ‘How's [Mom] doing?’ I’ve at least written it down, so I kind of have an idea of what's going on.”
-Speaker 3, Focus Group B
Indeed, very few participants outright rejected the idea of writing, suggesting that an EW intervention may be broadly accepted among caregivers of a spouse living with ADRD.
Motivations to write and expected benefits
Caregivers cited a wide range of perceived benefits that would motivate them to participate in an EW intervention. Many caregivers shared that EW may be a way to release intense emotions like anger and frustration, with some naming these emotions as being a barrier to their ability to connect with their partner in positive ways.
“… It's like knowing that I’m angry at the disease and not at the husband … but the husband is the one who gets the brunt of the anger and I would like to have diffused that before it became a problem …”
-Speaker 1, Focus Group A
Further, some caregivers expressed concern about these intense feelings negatively affecting their relationship with their spouse, but also, how they felt about themselves. Some expressed that perhaps writing earlier in their caregiving journey may have helped,
“I’m just very angry all the time and I’ve not ever been an angry person. I don’t recognize myself and I’m wondering if maybe writing some of that down might have helped take away some of that anger.”
-Speaker 1, Focus Group A
Caregivers also described needing an outlet for their anxiety and worry, with some noting that EW might provide this outlet.
“I think that the writing can diffuse umm … the big anxiety,”
-Speaker 3, Focus Group A
“… it's also a release for me … I get all tense and built up and I’m worried about her and when I can write it down it helps get rid of it.”
-Speaker 3, Focus Group B
Further, caregivers expressed the need for space and support to process the shock of unexpected turns in their spouse's disease progression.
“… sometimes all I need to do is just say how much this thing that just happened scared me.”
-Speaker 3, Focus Group A
“… something shocking happens and I’m never prepared for it … if I was gonna write and try to put my feelings on paper, that would be the time … when I’m hit with something that just throws me for a loop.”
-Speaker 4, Focus Group D
Importantly, caregivers appreciated EW as an avenue to express their feelings externally yet keep that information private.
“… it helps me get rid of some of my frustration and anger ‘cause I can write it on paper and I don’t have to say it to anybody else …”
-Speaker 3 Focus Group B
Caregivers expressed that EW may not only serve as an outlet and facilitator of stress release, but also a place where they can reflect on the positives of the caregiving journey.
“… at those random times when … I see something happy, then I’ll journal about it.”
-Speaker 3, Focus Group B
“… what have we gotten out of it, how are we stronger, what is better about our lives, what do we appreciate about our spouses …”
-Speaker 1, Focus Group C
Potential barriers to engaging in expressive writing
Lack of time
Many caregivers expressed concern that their caregiving responsibilities and daily routines left little room for additional activities. When caregivers did have moments to themselves, they reported prioritizing essential tasks like grocery shopping and household chores.
“… it's really hard to find 20 min to do anything other than give care.”
-Speaker 1, Focus Group A
“… I don’t know where I'm going to find the time, I’m trying to be a caregiver but I’m also trying to manage my own business …”
-Speaker 5, Focus Group A
When asked about the best time of day to write, caregivers agreed it was when their spouse was safely occupied, and they had sufficient energy, time, and space for reflection. This occurred most often when their spouse was sleeping, watching TV, or under the supervision of another caregiver.
“I would wait for him to go to sleep and then I would probably, you know, have that time to try and unwind and be able to reflect …”
-Speaker 4, Focus Group C
“For me it would be in the morning, because he sleeps late.”
-Speaker 1, Focus Group D
“For me, 5 or 6 o'clock when he's watching his favorite programs on the TV.”
-Speaker 6, Focus Group C
Lack of energy
Many caregivers expressed concerns about their emotional and physical capacity to engage in an EW intervention. Several participants worried writing expressively may consume what little of their energy remains after a day of caregiving.
“I don’t have the same kind of emotional energy that I’ve had in the past. So writing down my feelings … could further drain what emotional energy I do have …”
-Speaker 2, Focus Group A
Apprehensions about writing
While most caregivers were open to writing, several expressed concerns about its potential impact. Some feared that exploring negative emotions might increase their stress, undermining the intended benefits of an EW program.
“I [have] an … apprehension sometimes to writing down what I'm thinking. You know, almost … shame. You know, like how could I … put down in a notebook that you know my spouse is driving me nuts? You know what I mean, because it it's not good (laughter) but at the same time, that's kind of how I feel. So … I embrace the concept [of EW] and I understand [its] use … it's just … a struggle for me personally.”
-Speaker 4, Focus Group C
Priority features of an EW intervention
Private and secure
When asked about their preferred writing format, most caregivers primarily emphasized the importance of privacy and security. Many voiced concerns about their spouse's curiosity, the potential for their spouse to read their writing, and the lack of privacy in their immediate caregiving environment.
“… my husband will look at and read anything he comes across …”
-Speaker 1, Focus Group A
“I have no privacy, and so, you know, it's just ‘who's that?’ and ‘was that me you’re talking about?’ …”
-Speaker 2, Focus Group A
Flexible writing modality
When asking caregivers how they were most comfortable writing, responses were split between those who preferred to handwrite, use a computer, use a mobile device, or use a combination of these formats. Regardless of the preferred writing format, however, caregivers agreed the intervention tool must be familiar, accessible, efficient and easy to use. Additionally, several caregivers expressed that the easier and quicker they could access their writing instrument, the more likely they were to engage with the proposed EW program.
“… I’m so familiar with the computer and the keyboard, I would do everything on the computer …”
-Speaker 6, Focus Group B
“I’ve always got my phone with me so I just write a quick email to myself …”
-Speaker 3, Focus Group B
“I just seem to do a lot better if I just have a big notebook and I just write it all down.”
-Speaker 6, Focus Group C
Wave 1 conclusions
When participants discussed essential components of an online intervention, they cited a need for privacy and security as well as flexibility with how they could write. Previous research assessing privacy-related telehealth risks found similar concerns, with participants expressing worries pertaining to being overheard in their homes, confidentiality of their information, and concerns about the ease-of-use for online modalities, 45 To help us address these concerns, we consulted a product designer (also a co-author on this manuscript) about what type of “online” product would best fit caregivers’ needs, preferences, and motivations expressed in Wave 1. Given that caregivers expressed needing an efficient and accessible program that they could take anywhere, our product designer recommended turning our writing program into an “app”. Delivering the intervention through an app allowed us to create a single, contained environment for the entire series: one that offered privacy and a cohesive space to engage with the writing prompts. The app format made it possible to integrate supportive elements at key points in the intervention, such as gentle push notifications to encourage session completion, affirmations following emotional writing, visual orientation and nudges like progress tracking, and calming imagery alongside a personalized greeting to help caregivers feel seen and supported. Compared to other modalities (e.g., email or print-based prompts), the app offered a more effective way to address barriers identified in Wave 1.
Building on this rationale, we dedicated ourselves to ensuring the app would be user-friendly and make writing more accessible by allowing participants to write and express in several different forms, all within a single, cohesive digital space. Thus, we began Wave 2 with the intention to assess the feasibility and acceptability of an EW app for caregivers of a spouse living with ADRD.
Wave 2 focus group results
App accessibility and flexibility
Participants in Wave 2 focus groups expressed a strong desire for accessibility and flexibility in an EW intervention. Participants requested cross-platform access, with five caregivers suggesting a desire to complete writing sessions using a computer. Others were interested in the potential to handwrite or dictate responses.
“I just would like to have a place to go where I could use the computer and … I'd be able to see it all on the phone also”
-Speaker 4, Focus Group 2A
“The fact that you offered the possibility of being able to speak about it [dictate] instead of actually physically writing would also be good for people who have a problem writing it down.”
-Speaker 2, Focus Group 2B
“I think [an app] would be a good idea also because so many people use apps. But on the flip side, as of right now, a large part of the generation that's dealing with someone with dementia is going to be elderly. And how much do they use apps? So … I would like there to be another option too.”
-Speaker 2, Focus Group 2C
“Well, I'm going to say I like the app thing only because it would be an icon on my phone. All I have to do is press it and it would open up, and then I could follow through. It. That to me is something.”
-Speaker 5, Focus Group 2C
Focus group participants were also asked how often and when they would prefer to receive notifications from the app. Participants generally agreed that notifications are important and they preferred the autonomy to choose how they would receive notifications (e.g., email, text, or push). However, some caregivers suggested that we be careful that these notifications do not instill shame or guilt. Participants also preferred no more than one notification per writing session.
“I have no objection to getting reminders because, you know, like, [Speaker 2] said, my life is dictated by Post-it notes”
-Speaker 3, Focus Group 2B
“I think the reminder is really important because as you get involved in the day's activities and you're going to forget about it”
-Speaker 4, Focus Group 2B
- “… the notifications should be uplifting again. “Hey, you feel like … writing tonight?” or “hey, is this a good time for you to go write?” Or you know … something that's just not like, “hey, it's time to write.” Make it more positive. Like it's, you know, this could help …
Speaker 5, Focus Group 2B
- “I don't think you [want] to get to the point where you're, like, worrying all day long. Oh gosh, … I've got to write today … we have enough things pressing anyway …”
-Speaker 2, Focus Group 2B
Caregivers in Wave 2 focus groups appreciated the simplicity of the app design. The app prototype was intentionally designed with muted colors and easy-to-read font. Participants suggested the app would not cause additional eye strain, which may be especially pertinent to older adults.
“I think the app looks really good. user friendly, kind of a calming esthetics to it.”
-Speaker 2, Focus Group 2C
App features
When discussing specific features of the EW app, participants provided feedback on the timer function, notes section, and writing prompts/flow. The timer function, set to 15 min for each prompt, received generally positive feedback. One caregiver noted that the specific 15-min goal would be motivating. Participants suggested allowing app users to revisit prompts over a few days. This would allow caregivers time to process questions before finishing the writing prompt. Such a feature would also include a reminder to finish the prompt. Caregivers also responded positively to the presence of a notes section in the app. Participants expressed that the notes feature would be beneficial by allowing them to capture thoughts or ideas between writing sessions. Some noted that this feature is in-line with caregivers’ daily life, as they often create to-do-lists or ideas to return to at another date.
“Having a 15 min timer allows me to then want to get something accomplished”
–Speaker 2, Focus Group 2D
“I like the idea of having notes because sometimes you don't have the brain power or the bandwidth to answer those questions, but sometimes you just have something that you just want to say and it might serve as a memory refresher on the next question that comes up later. Say, hey, I kind of had some thoughts … but I don't remember. Let me go back and check my notes.”
-Speaker 5, Focus Group 2B
Writing prompts
Caregivers were also presented with a series of proposed prompts for the EW intervention. While the feedback was largely positive, some participants noted some prompts were more tailored to “new” caregivers rather than “experienced” caregivers. For example, one question asked participants to consider when their partner was first diagnosed with ADRD. This question may be best for “new” caregivers. In addition, participants in the third focus group recommended that we remove the future-focused language in the writing prompts, as it may induce caregivers’ anxiety. Finally, focus group participants noted that the intervention should include no more than two prompts per week, to enhance feasibility.
“Yeah, because I think the caregiver who's just starting a journey … they need different questions. But those of us who've been on the journey for much longer, maybe those more intense questions to help process.”
-Speaker 2, Focus Group 2B
“The future, that word is almost a trigger, I would think, because for me personally, I'm smack dab in the middle of a horrendous, difficult journey, so I have trouble looking to the end of the day. So to look to the future is really not in my realm of reality.”
-Speaker 2, Focus Group 2C
Confidentiality and privacy
Confidentiality and privacy also arose as major themes of Wave 2 focus groups. Some participants discussed a potential “delete” feature for writing prompts, since they would prefer that no one have access to past thoughts and feelings via their writing, including themselves. However, other participants were open to sharing their writing with researchers but only if the information is used to help others. These caregivers suggested sharing could be an option if anonymized.
“I'm sure we all have our personal experiences, and … we wouldn't be as free to write if we knew it wasn't secure”
-Speaker 5, Focus Group 2B
“There could be some really dark thoughts put down on paper or on the app that they don't want anyone to see.”
-Speaker 6, Focus Group 2C
Usability test results
After completing usability testing (n = 5), we analyzed the recorded sessions identifying where participants clicked, got stuck and encountered other points of confusion within each task flow. Using the data (see the Supplemental Material [S4] for more details), along with participant feedback about individual screens and their overall experiences, we arrived at the following results.
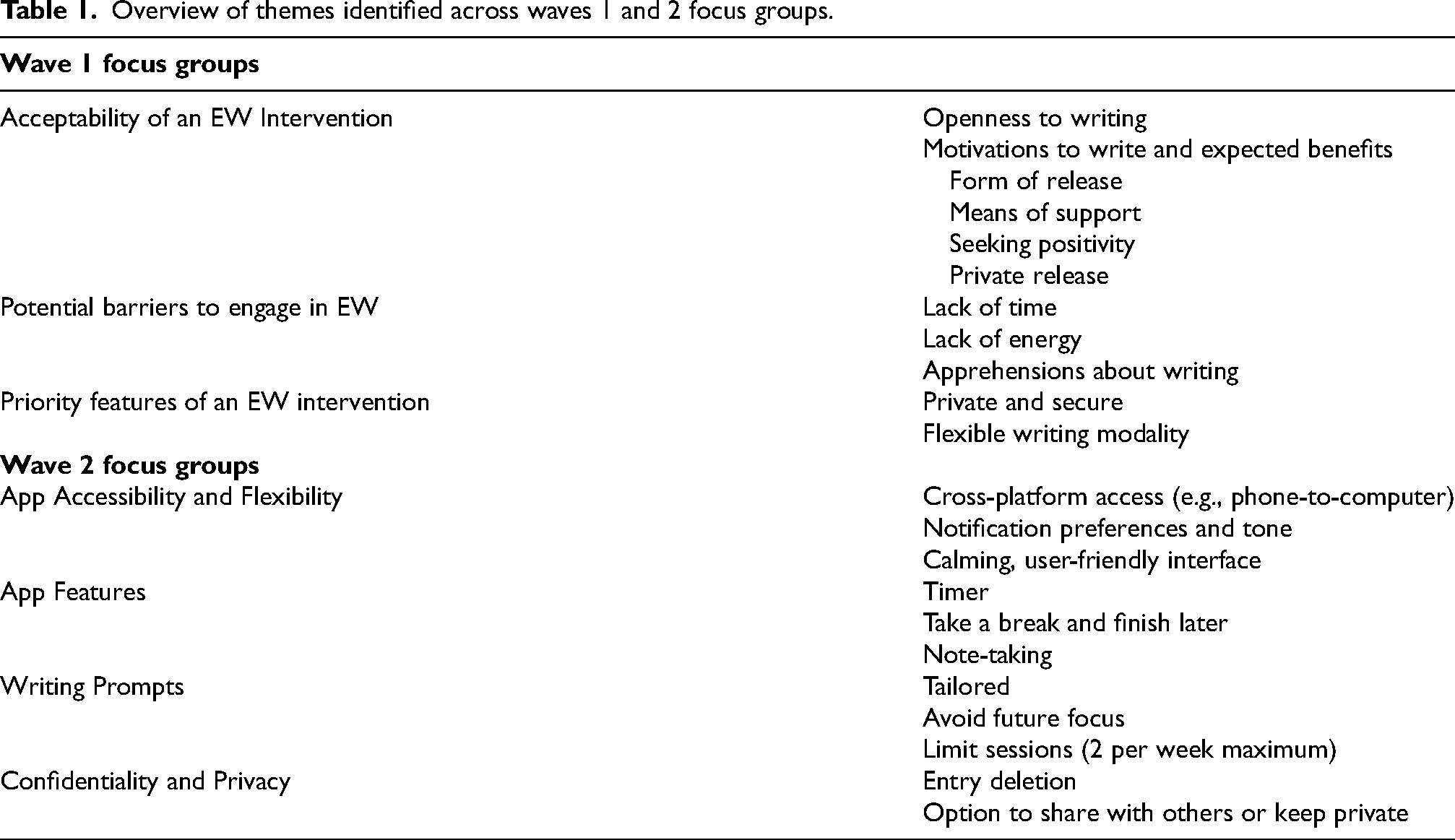
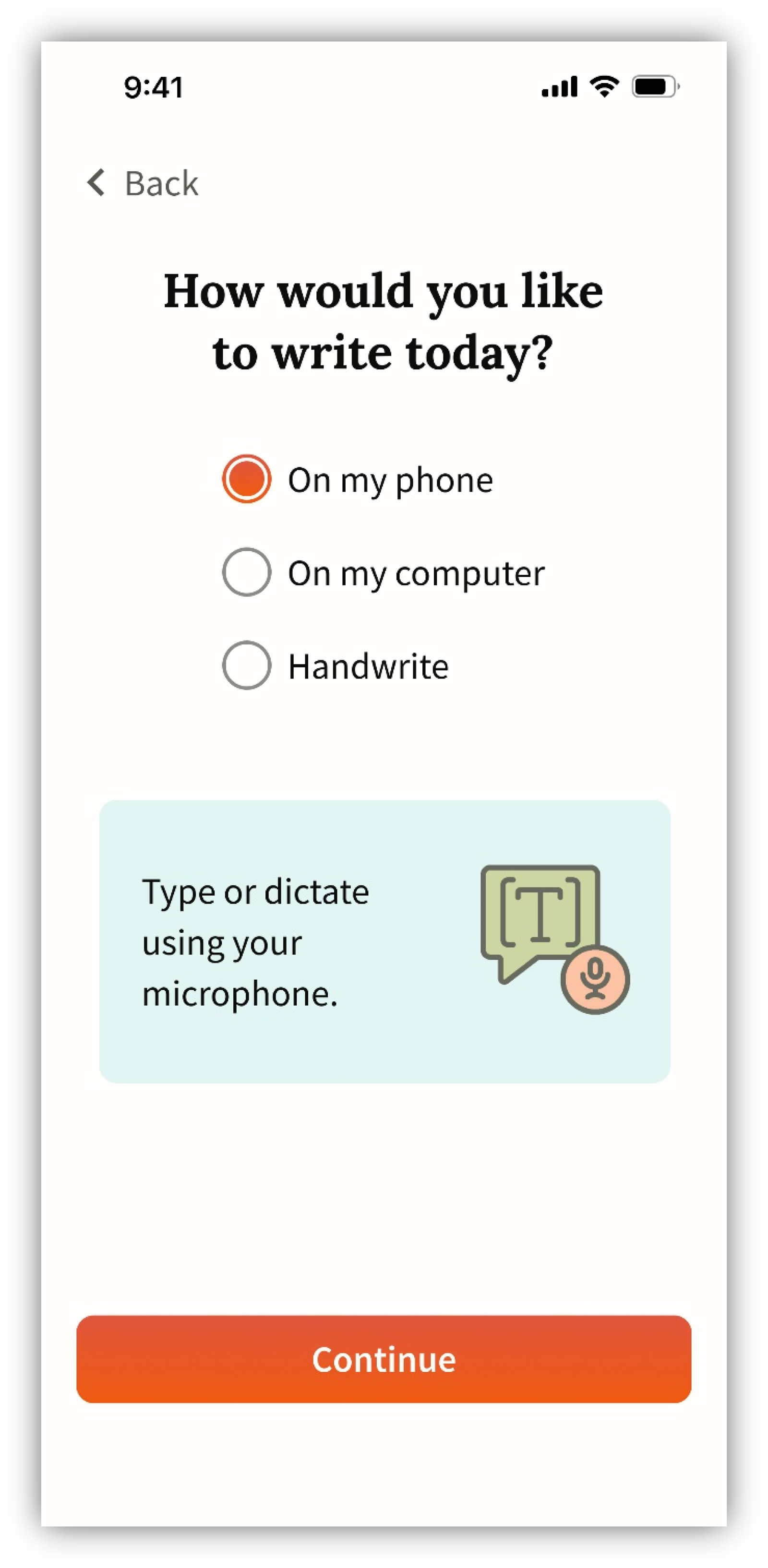
The task flow completion rate from usability testing indicated that the app design is primarily intuitive with some common points of confusion: all participants were able to complete the core writing task flow, and most completed all three task flows. The starting point for all tasks was the home screen (Figure 1), which was described as calming, but presented some minor visibility issues for some participants. The next screen asked participants how they would like to write, indicating options for typing on the phone, computer, or handwriting (Figure 2). Once a selection is made, the user is given writing instructions before they start the timer and begin writing (Figure 3). Participants indicated that more detailed writing instructions on this screen could reduce apprehension about the upcoming writing task.
Modality selection screens presented during usability testing.
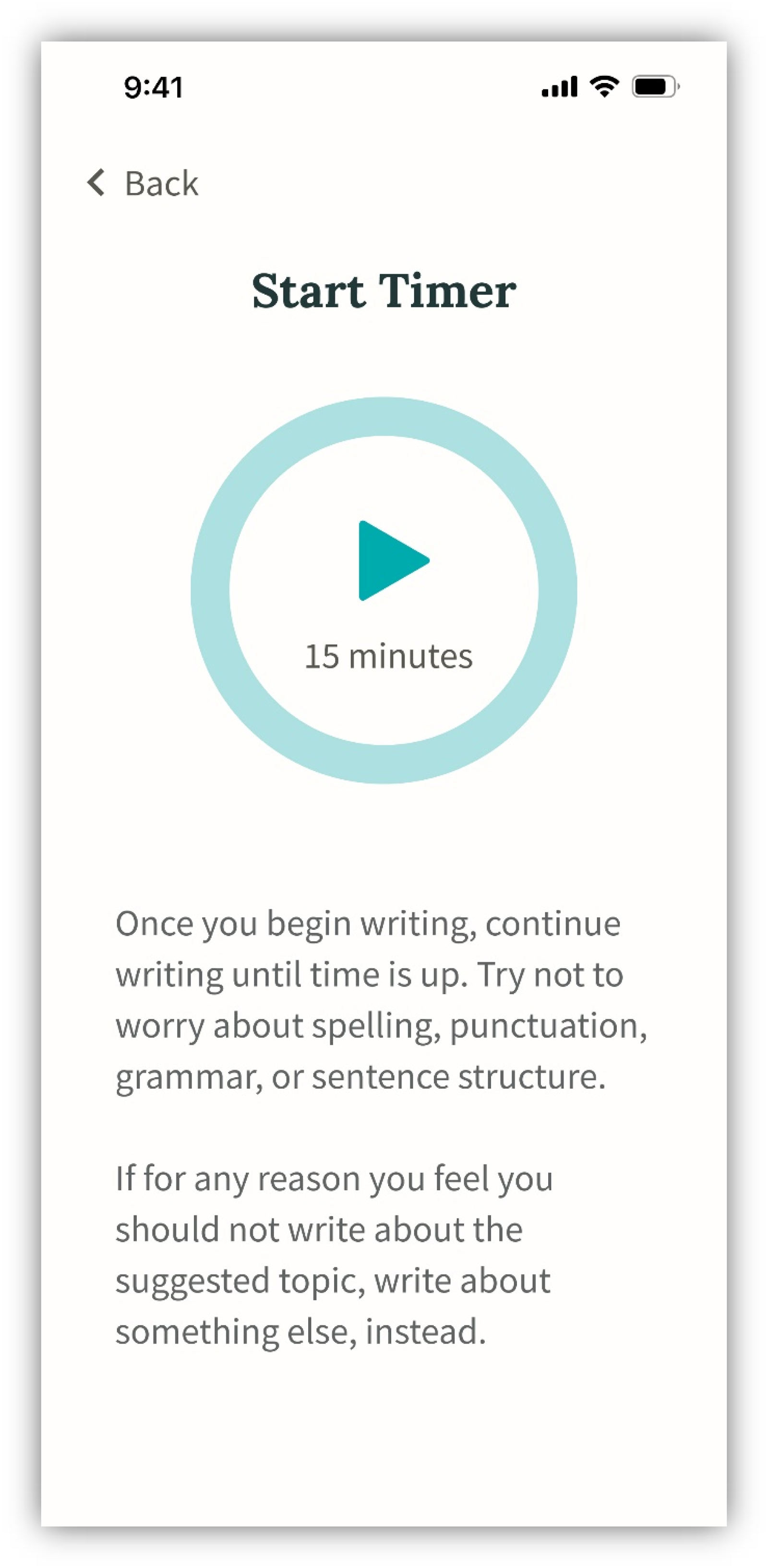
Writing instructions screen presented during usability testing.
The writing screen (Figure 4), in which participants respond to a writing prompt, posed some challenges for users. This indicates a need to further simplify the writing screen design. Following the writing session, participants are asked to rate how they feel and how meaningful the writing session was (Figure 5). The first rating question (Figure 5, panel a) was found to be unclear.
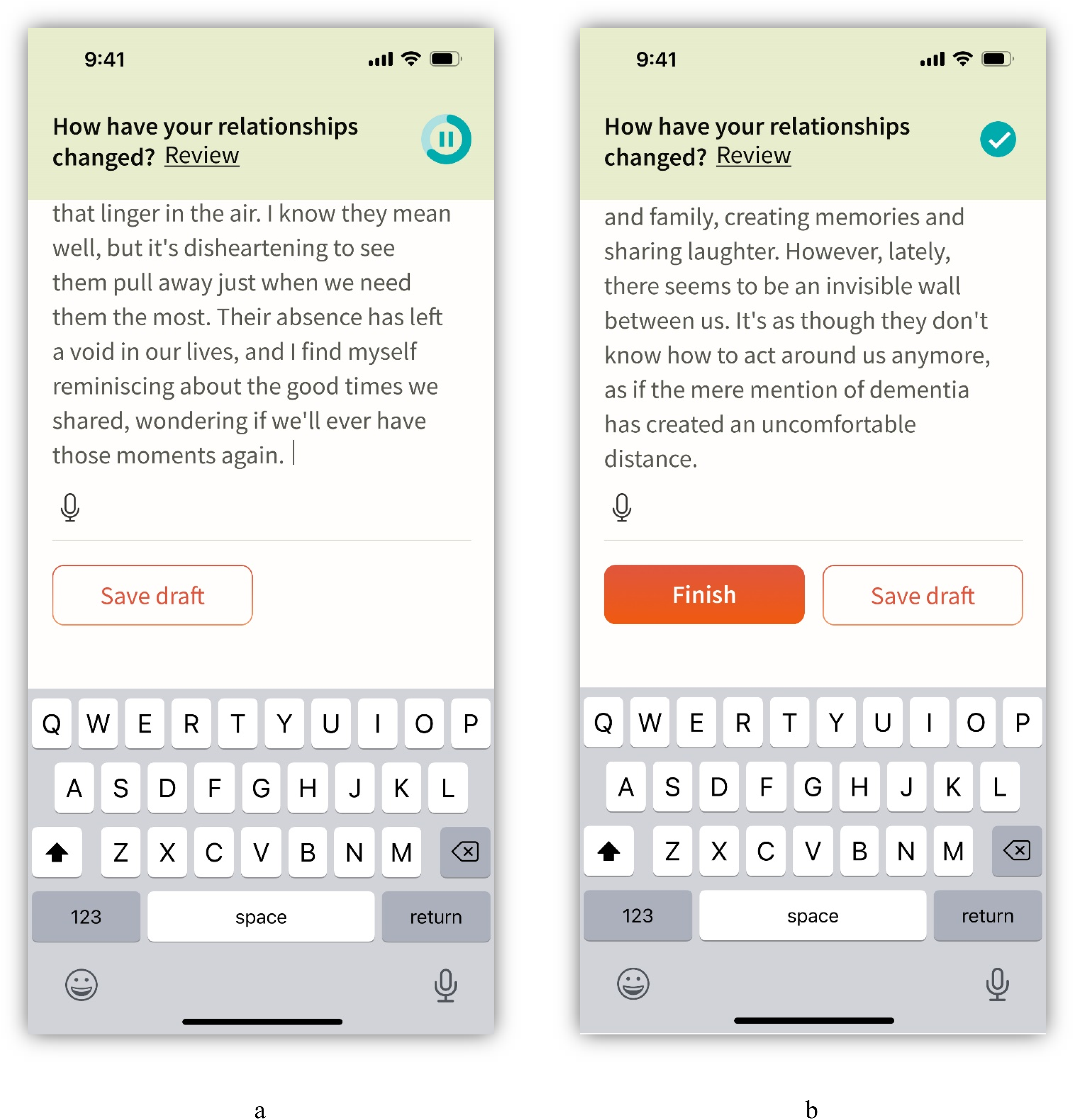
Writing screens presented during usability testing. Panel a represents 10 min of writing (i.e., an in-progress writing session); panel b represents 15 min of writing (i.e., a complete writing session).
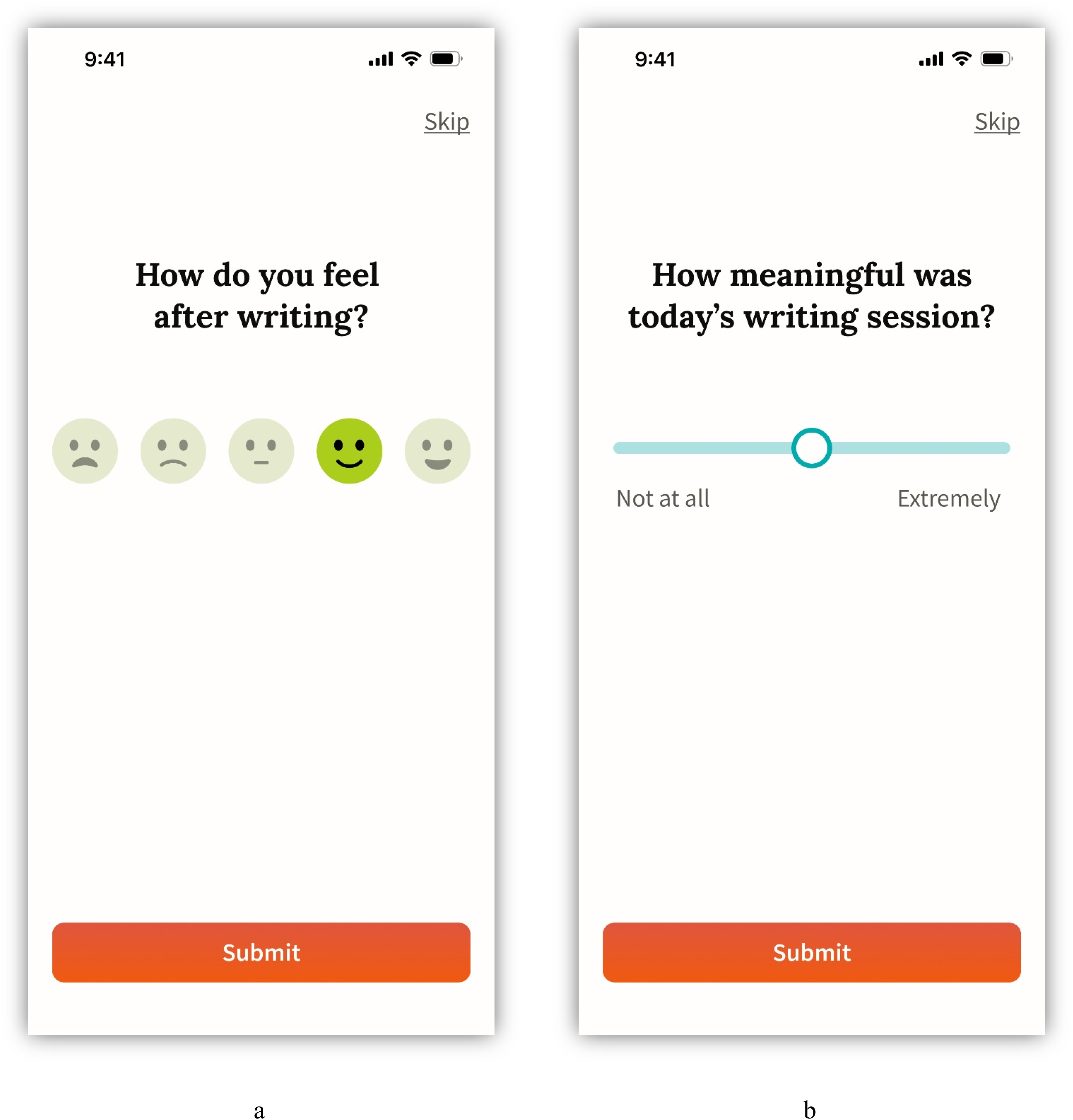
Rating question screens presented during usability testing.
Participants were also asked to interact with the journal user interface (UI). The journal screen (Figure 6), which shows completed writing entries and drafts, was intuitive. Each participant understood how to navigate to the journal from the home screen.
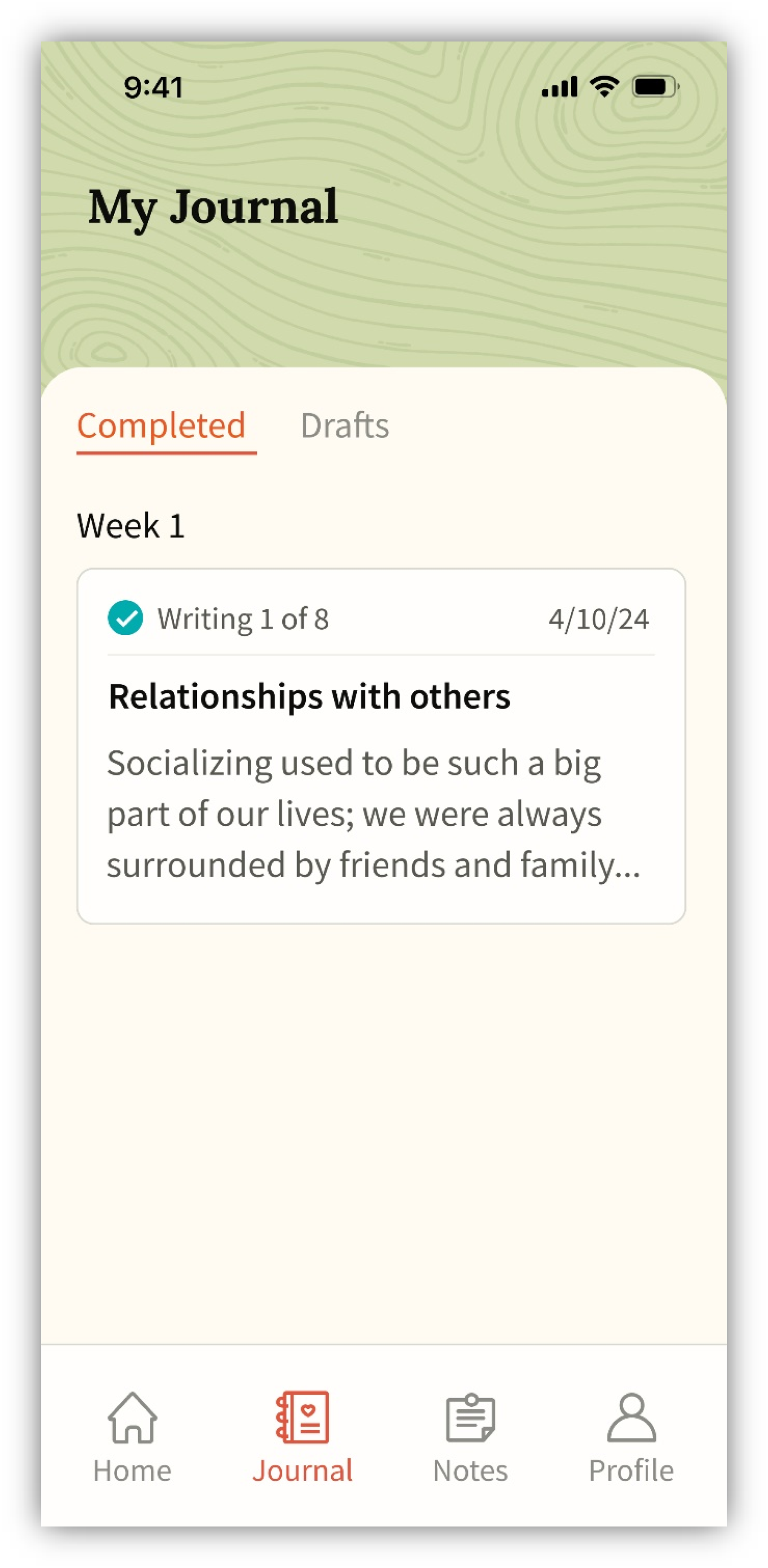
Journal screen presented during usability testing.
It was unclear whether participants understood the purpose of the Notes feature. Most had difficulty finding the Notes screen (Figure 7) from the home page, although once there, they easily created a note. When tasked with writing about a note they made previously, most participants found one of the two possible paths (Figure 8), but with enough hesitation to suggest further iteration and testing is needed.
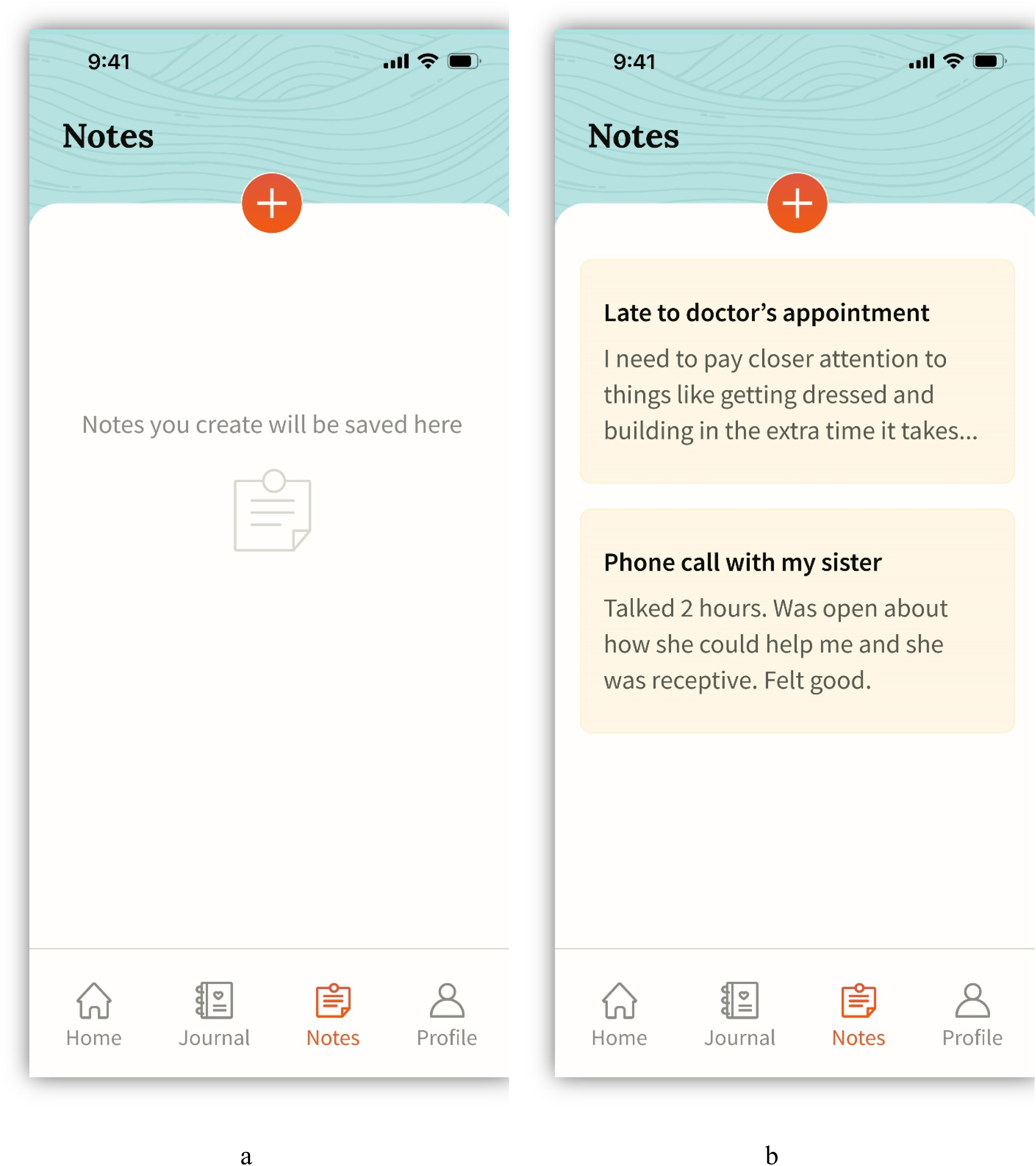
Notes screens presented during usability testing.
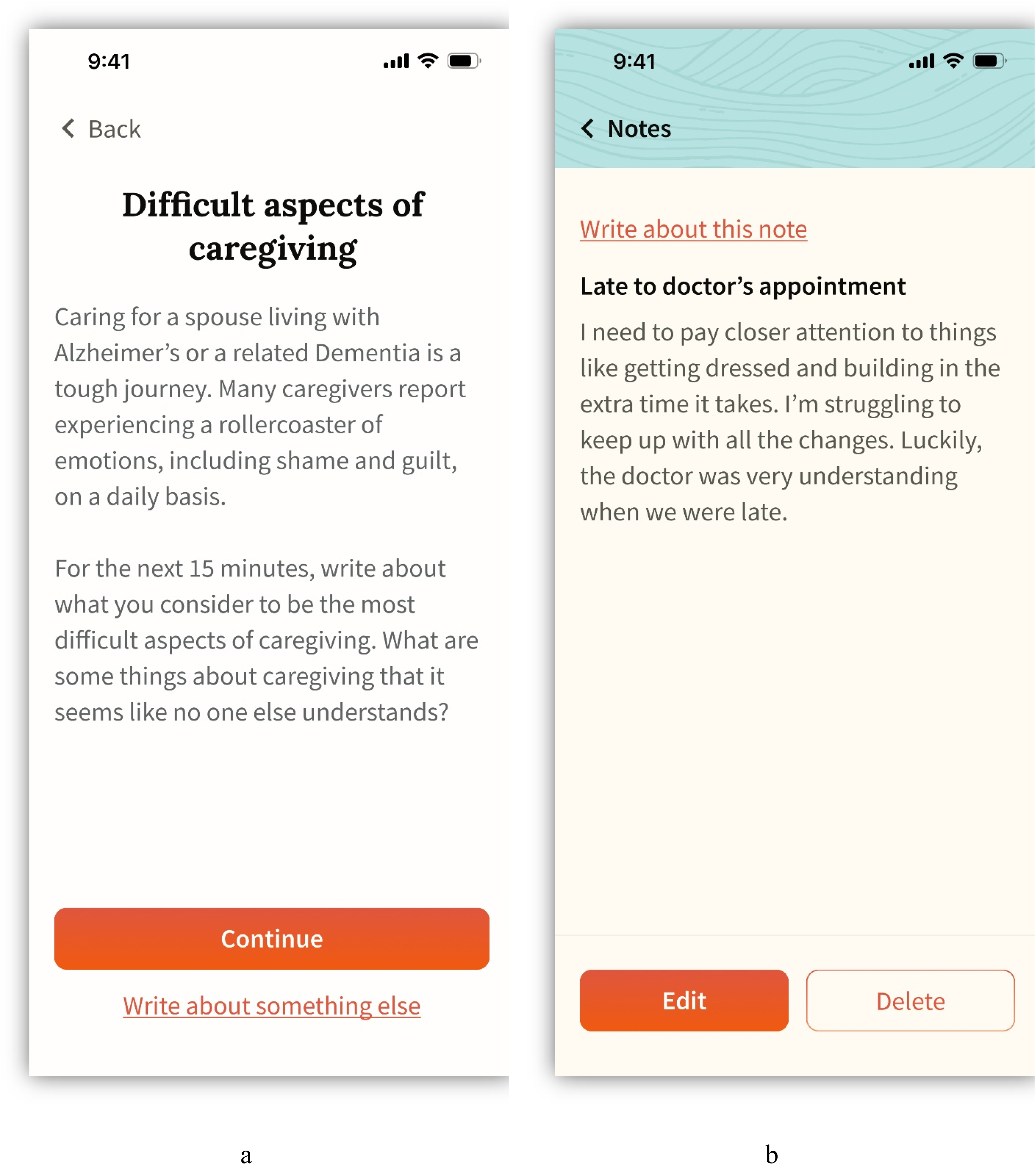
Entry point screens for the task flow, “complete a writing session from a note” presented during usability testing. Panel a represents path a, where participants start the task by tapping “Write about something else”; panel b represents path b, where participants start the task by tapping “Write about this note”.
Last, participants were presented with two versions of the home screen (Figure 1). Overall, caregivers preferred version B of the home screen over version A because they felt the progress bar was more prominent and easier to understand.
Discussion
Taken together, the results of Wave 1 and 2 focus groups indicate that an EW intervention to aid ADRD spousal caregivers and alleviate stress is acceptable and feasible. Wave 1 focus groups, which asked caregivers about the design of an online writing program as well as barriers to participation, indicated a need for an intervention that is efficient, mobile, and readily accessible. Wave 2 focus groups guided the development of an app-based prototype while testing caregivers’ perceived acceptability of potential app features. Finally, usability testing showed the proposed app's workflow is accessible and intuitive to caregivers. Thus, an app-based EW intervention may be a useful strategy for reducing the negative health consequences of stress among ADRD spousal caregivers. Further, an app could be a more cost-effective 46 option for caregivers, relative to in-person therapeutic alternatives like traditional CBT.
Conducting this research helped us identify several opportunities for targeted treatment. Tailoring an EW program as an outlet for negative emotions, as well as a place to reflect on positive events surrounding unique caregiving-related experiences, may increase caregiver adherence and acceptability to a writing intervention. Further, because the ideal time to write varies greatly by individual circumstances on a given day, a flexible EW program that allows caregivers to customize their writing schedule may be most feasible. To minimize apprehension and increase acceptability, an EW program should be welcoming, validate caregiver's emotions and experiences, provide guidance, recognize progress, and space out writing sessions to avoid overwhelming caregivers. To address the concerns of caregivers’ lack of energy, an EW program could offer guided prompts, writing reminders and encouragement. Further, caregivers may not engage in an EW program if they fear their writing may be seen by anyone else, including researchers, their spouse or other caregivers. Creation of an EW program therefore must include a feature of security and privacy regarding writing submissions. Caregivers also may be more likely to engage with an adaptable EW program that allows them to choose their preferred writing modality (e.g., handwritten, computer/desktop, or typing or dictating directly into the phone app). This would include the ability to take notes on-the-go, a feature uniquely supported by a mobile device. Overall, these sentiments expressed by caregivers indicate a need for flexibility and accessibility regarding writing modality, providing strong justification for implementation of an EW program via a mobile app and/or web browser. To overcome time constraints, an EW program should be flexible, self-paced, and easily accessible. Relatively short writing sessions designed with caregivers’ busy schedules in mind may bolster both participation in and adherence to an EW program.
Notably, collaboration with an industry-based product designer was essential for the success of this intervention development project; the team utilized a “team science” approach, including open communication, clearly defined roles and responsibilities, and trust among collaborators. 47 The app prototype was developed by our product designer in tandem with the writing intervention content by the research team, helping ensure that the app's features, screens, and the user experience aligned with the needs of caregivers. Through this integrated approach, we were also able to make the intervention app-based, creating a dedicated environment that could deliver affirmations, psychoeducation, reminders, and progress tracking, while helping caregivers feel supported throughout their writing experience. Continued development (e.g., of the onboarding process) and subsequent beta testing of the app is needed to ensure readiness of a randomized controlled trial. Further, future research is needed to ensure the name of the intervention product is attractive as well as considerate of a broad range of caregiver's perspectives.
In addition to the results reported here, a number of discoveries related to labels and language organically surfaced during the focus groups. For example, we referred to the intervention as “Writing to Heal”, an EW program for ADRD spousal caregivers. However, the language we used, particularly the labels “healing” and “program,” was received differently among caregivers. For example, one caregiver found the use of the word “heal” upsetting because there is no cure for ADRD, and therefore, “healing” (i.e., a reversal of their degenerative condition) is not possible for their spouse. Additionally, the term “writing program” was not received well by all caregivers; some found the word “program” daunting given they already had so many other commitments associated with their caregiving role. Instead, “writing series” may be a less intimidating alternative. While recruiting caregivers of spouses living with ADRD, some caregivers shared that they did not identify with the term ADRD; they expressed having markedly different experiences as a spousal caregiver of a person living with other form(s) of dementia than spousal caregivers of people living with Alzheimer's Disease. Researchers recruiting dementia caregivers may consider whether the term “ADRD” is as inclusive as we intend it to be and may consider instead, using the term “dementia” more broadly. Nevertheless, these insights from caregivers are paramount to developing intervention products specifically tailored to caregiver needs and experiences, and for conducting more inclusive intervention trials.
Future research is needed to determine whether there may be gender differences in caregiver acceptability and feasibility of the intervention product. The CDC reports that approximately two thirds of dementia caregivers are women. 48 This gender bias in the general caregiving population is also reflected in our study sample, though multiple men were included in this study. The last focus group reported in this study consisted of two male caregivers, who shared unique perspectives that they may not have discussed had female caregivers been present. Previous research suggests that there are gender differences in caregiving roles; for example, men in a caregiving role tend to focus on instrumental tasks while female caregivers tend to take on more social and emotional tasks. 49 Accordingly, future research is necessary to ensure that caregiving intervention products, including the app developed in the current study, are inclusive of caregiver's needs across the gender spectrum.
Mackenzie and colleagues found that while writing was beneficial to mental and physical health improvements, there were no significant differences in outcomes between an expressive-writing and history-writing approach. 19 This suggests writing, in any form, may be beneficial, and should be explored further. Some participants in this study reported already writing objectively about “facts” or events related to their spouse's behavior, diagnosis, or symptoms over time. Most caregivers agreed writing was a helpful way to record events, whether it be to document their spouse's disease progression or capture a significant moment in time they may want to reflect on later. Thus, writing seemed to serve multiple helpful purposes for caregivers, and many were open to the idea of using writing as a form of tangible support in addition to an emotional expression tool. Future trials of EW among caregivers may include experimental conditions in which caregivers write expressively or objectively about their caregiving experiences to compare effects.
This study was not without limitations. Being naive to participant's previous writing experiences at the time of recruitment may have inadvertently opened the study to potential sources of bias. For example, it could be that participants who were already interested in or experienced with writing self-selected into a study about expressive writing, biasing our acceptability results. In addition, this study collected data from caregivers nationwide; to do so, we had to conduct focus groups, virtually. While there is a multitude of benefits to online focus groups, 50 there may also be limitations in the depth of the discussions generated.
Although some other apps have been developed to help ADRD caregivers, few are accessible to caregivers and even less present evidence for improved clinical outcomes among caregivers. 51 Further, while these resources are valuable, they primarily focus on monitoring symptoms, recording current events with the person living with ADRD, facilitating communication across care teams, or providing informational resources.51–55 In contrast, the present intervention aims to help caregivers emotionally process the stressors associated with caregiving, with the hope that reprocessing stressful events may thereby reduce the negative impact of stress on their body, mind, and spirit.
Conclusion
ADRD caregiving is extremely stressful and often prolonged. 2 There is a demonstrated need for evidenced-based interventions that may reduce the negative effects of stress associated with caregiving, particularly among spousal caregivers to those living with ADRD. In this study, we used qualitative methods and usability testing to identify opportunities for targeted treatment and potential barriers to a mobile app-based writing series. This intervention was intended to help spousal caregivers process their emotions associated with the stress and grief involved in caregiving for a partner living with ADRD, while continuously monitoring caregivers’ perceived acceptability and feasibility of each proposed feature. A mobile-based writing intervention catering to the specific needs of these caregivers may be a helpful coping resource for caregivers, but future research is needed to test the app's efficacy in reducing negative mental and physical health outcomes among spousal caregivers.
Supplemental Material
sj-pdf-1-alz-10.1177_13872877251378478 - Supplemental material for Initial development of the writing to heal app: A structured writing series for caregivers of spouses living with Alzheimer's disease and related dementias
Supplemental material, sj-pdf-1-alz-10.1177_13872877251378478 for Initial development of the writing to heal app: A structured writing series for caregivers of spouses living with Alzheimer's disease and related dementias by Samantha Weiss, Katherine Harris, Olivia L Carney, Valentina I Maza, Sierra Wickline, Alexandria Henderson, Trudy Widjaja, Brighton Garrett, Daniel L Hill, Leona Liskovec, Patricia Chen and Angie S LeRoy in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We would like to thank our research team and collaborators for their commitment to and support of the planning and data collection for this project—especially Chris Fagundes, Ann Wang, Kristi English, Alex Wherrey, Grant Shrable, Shreyas Srinivasan, Emily Kolb, Dylan Puepke, Katherine Beach, Ashton Richards, Madelyn Edlund, Victoria Norton, Caroline Wilkerson, Carlos Carbajal & Sofia Villarreal-Ibarra as well as Nola Majoros. We would like to thank Michael Liskovec for helping us anticipate and avoid potential obstacles in developing the Writing to Heal app. Importantly, we would also like to thank the caregivers who participated in our study and so generously and selflessly shared their insight and experiences with us, for the greater good of those whose families are impacted by Alzheimer's or a related dementia. Use of AI: AI Images – The home screen image (on the app) was generated using Visual Electric, an AI image generator (prompt: concept of calm with sun on horizon with oranges and blues and greens, filter: ethereal watercolor). AI Journaling – While developing the writing prompts, the authors referenced Rosebud.app, an AI-powered journal for mental health and personal growth. The authors engaged in roleplay with the journal, writing from the perspective of a caregiver of a spouse with ADRD. The journal's responses and choice of words were then used as a resource to spark further discussions among the researchers and shape the language used in the writing prompts.
ORCID iDs
Ethical considerations
This study was approved by the Rice University Institutional Review Board IRB-FY2023-219.
Consent to participate
Each of the caregivers included in this study completed the informed consent process and provided written consent to participate.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by an NIH K01 Career Development Award from the National Institute on Aging (K01AG073824-02, PI: Angie LeRoy). In addition, the preparation of this publication was made possible through the support of Grant 62691 from the John Templeton Foundation. The opinions expressed in this publication are those of the author(s) and do not necessarily reflect the views of the John Templeton Foundation. In addition, funding for the preparation of this article was supported by a University of North Florida (UNF) MedNexus Innovation Fund Award. Funding for the open access fees associated with the publication of this article was provided by a UNF Faculty Publishing Grant, as well as a UNF College of Arts & Sciences Faculty Publishing Grant.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
De-identified qualitative focus group transcripts are available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.