
Abstract
Care aides in long-term care (LTC) institutions care for older disabled residents at high risk for COVID-19. However, they experienced many stressors during the COVID-19 pandemic. This study aims to explore the working experiences of care aides in LTC institutions following the relaxation of COVID-19 regulations in Taiwan. This qualitative descriptive study included 20 care aides who had cared for residents with COVID-19. Data were obtained via semi-structured interviews. Caring for residents with COVID-19 and the difficulties, resources and teamwork, and impact of care aides’ work on their lives were discussed. Consequently, four themes were identified. First, difficulties in care, which included physical limitations by protection, workload, and impact of work schedule on the lives of the care aides. Second, psychological impact, such as worry, social isolation, and burnout. Third, interpersonal relationships with supervisors, colleagues, residents, and their families. Fourth, infection control policy from the institution and government. When infection control policies were relaxed, care aides had difficulties in caring for residents; furthermore, their family and social lives were also affected. They were required to learn knowledge of and skills for COVID-19 management. Institutions were required to provide support in materials, care processes, environment, and management.
Introduction
The COVID-19 pandemic has had a profound impact on global health, socioeconomic well-being, and healthcare systems (Kaye et al., 2021). In Taiwan, the period of April 2022 stands out as a pivotal moment due to the relaxation of regulations, marking a significant increase in COVID-19 cases. The number of new cases surged from 3,181 per month in March 2022 to 120,457 in April 2022, signaling a stark uptrend (Lai et al., 2023). Notably, COVID-19 rose from being the 19th leading cause of death in Taiwan in 2021, with 896 fatalities, to the third leading cause in 2022, with 14,667 fatalities (Centers for Disease Control, 2023).
Older adults faced heightened health risks from COVID-19 compared to their younger counterparts (Pant & Subedi, 2020). They were more susceptible to infection, severe illness, hospitalization, and prolonged hospital stays than those under 65 years of age (Applegate & Ouslander, 2020; Chung et al., 2022). Factors such as frailty, comorbidities, and compromised immune function contributed to higher mortality rates among older patients (Applegate & Ouslander, 2020; Wang et al., 2020), while isolation and loneliness exacerbated risks to their mental well-being (Lebrasseur et al., 2021).
The proportion of older adults in Taiwan is projected to reach 20% by 2025 (National Development Council, 2023). With an increase in the aging population, care for older adults with disabilities is crucial. Long-term care (LTC) institutions provide care for older adults with moderate to severe disabilities. Owing to older adults’ high vulnerability to COVID-19, hospitals and LTC institutions in Taiwan had the strictest prevention measures. Furthermore, it was one of the last countries to ease restrictions. LTC institutions adopted the following preventive measures: regular body temperature monitoring and rapid testing for both residents and staff; residents not being allowed to go out and visit their families; use of disinfectives, protective gears, and face masks by the staff; staff having to stay in the same unit; and infected staff being quarantined (Calcaterra et al., 2022; Huang et al., 2021).
LTC targets residents with disabilities who require only physical care for eating, bathing, dressing, and exercising, and so on, rather than intensive medical care. Though not having nursing training, care aides play an important role in providing physical care and daily services. Staff in LTC institutions performed various tasks during the COVID-19 pandemic, such as infection control, routine care, safety maintenance, physical activity, mental support, and assisting communications between residents and their families via technology due to restrictions (Chu et al., 2022). They also had to learn of COVID-19 and its prevention, such as using protective equipment and procedures (Fisher et al., 2021; Yau et al., 2021).
The COVID-19 outbreak precipitated a surge in workload and extended working hours among healthcare workers (Sun et al., 2022), predominantly driven by the demands of COVID-19 prevention measures (Fisher et al., 2021; Yau et al., 2021). This increased workload correlated with elevated stress levels among nurses (Hoedl et al., 2021). Likewise, staff in long-term care (LTC) institutions faced myriad stressors, including the risk of infection, quarantine measures, changes in work schedules, and heightened workload (Avidor & Ayalon, 2022; Boamah et al., 2023). Additionally, stressors such as residents’ physical conditions and unmet needs (Chu et al., 2020), the transmission of COVID-19 to their families (Avidor & Ayalon, 2022), and negative public perceptions of COVID-19 in LTC settings (Reynolds et al., 2022) compounded the challenges.
Emotionally, staff experienced exhaustion and a spectrum of negative emotions, including anxiety (Hung et al., 2022), fear (Reynolds et al., 2022), burnout (Boamah et al., 2023), loneliness, and depressive symptoms (Eltaybani et al., 2024), throughout the pandemic. These negative feelings manifested differently across various stages. Early exposure was marked by fear, anxiety, and a sense of losing control, while the peak of the crisis brought about feelings of anxiety, helplessness, hopelessness, and depression. Moreover, long-term effects included depression, burnout, and post-traumatic stress disorder (Ardebili et al., 2021). Staff also grappled with grief and a sense of personal responsibility when residents succumbed to the virus (Capstick et al., 2022), though positive emotions such as pride and a sense of duty to care also emerged (Hung et al., 2022; Boamah et al., 2023). Meeting the challenges of caregiving during the pandemic necessitated both professional competencies—such as knowledge, skills, and resources—and psychological support for care aides (Eltaybani et al., 2024; Yau et al., 2021).
Previous studies focused on staff in LTC mixed nurses, care aides, and other professionals. However, care aides play a pivotal role in providing direct physical care and engaging older adults with COVID-19, often spending extended periods at their bedside. Hence, this study focused only on care aides. In addition, data were collected when the regulations were relaxed. This timing was pivotal as LTC institutions and staff endeavored to manage the care of numerous confirmed patients while mitigating the impact of COVID-19 on residents, staff, and the institutions themselves. Therefore, this study aims to explore the working experiences of care aides in LTC institution following the relaxation of COVID-19 regulations in Taiwan.
Methods
Research Design
This study employed a qualitative descriptive approach to explore the experiences of care aides during a specific period. The Taiwanese government relaxed their border control policy in March 2022. In addition, nosocomial infections began occurring in LTC institutions in May 2022. Hence, the number of COVID-19 cases increased quickly. Infection control policies included regular body temperature monitoring and rapid testing for both staff and residents, visitor restrictions, tracking records for public spaces, use of personal protective equipment (PPE), setting quarantine area and in-suit isolation, and limited interactions between different areas or floors (Huang et al., 2021).
This study was approved by an institutional review board. The research team provided participant criteria to the managers of LTC institutions, who then introduced willing participants to the study. Participants were informed of their rights—the right to quit during or after the interview without facing punitive action in their work and the right to anonymity, for example. All participants signed an informed consent form before the interviews. Interviews were conducted individually and face-to-face in quiet meeting rooms within the institutions. After the interviews were completed, they received 1,000 Taiwan dollars as a reward. Data were collected from July to August 2022.
Participants
The participants comprised Taiwanese care aides proficient in either Chinese or Taiwanese. In Taiwan, care aides are required to undergo a 90-hour training course and pass an exam for certification. Inclusion criteria encompassed care aides who had worked in nursing homes or LTC institutions between May and July 2022 and had provided care for residents diagnosed with COVID-19. Given the focus of this study on the relaxation of COVID-19 regulations, participants were required to have relevant working experience during that period. Individuals lacking experience in infection control, caring for residents with COVID-19, or those unwilling to participate were excluded. Participants were recruited from a nursing home with approximately 60 beds and a long-term care institution with around 200 beds in Southern Taiwan.
Data Collection
This study focused primarily on the experiences of care aides providing direct physical care for residents with COVID-19 amid the relaxation of COVID-19 regulations. Semi-structured interviews were conducted with the following questions: (1) How did you care for residents with COVID-19 and what care did you provide? What were the differences between caring for residents with and without COVID-19? How did these differences influence your work? (2) What were the difficulties in caring for residents with COVID-19? (3) During the pandemic, what resources did your institution provide (e.g., equipment, educational training, manpower, and bonus money)? Were these sufficient or not? (4) How did the infection control policy and relationships with the managers and your colleagues influence your work? (5) What was the impact of caring for residents with COVID-19 on your personal, social, and family life? How did you adapt to it?
Demographic and work characteristics were also collected, along with COVID-19 diagnosis results and feedback on caring for residents with COVID-19, (whether voluntarily or not) and worry of being infected (not possible, possible, and extreme possible).
Data Analysis
Interviews were audio recorded and transcribed verbatim. The data were subjected to thematic content analysis (Friese et al., 2018). First, the researchers familiarized themselves with the data. The verbatim transcripts were read repeatedly and the initial meanings were identified. Second, the initial coding was set and a framework was constructed. Important contents were identified, categorized, and organized. For example, when a participant said that “approval from the supervisor was a reason for continuing to work,” the statement was coded as “supervisors’ approval,” and all content regarding supervisors were categorized under this code. Third, themes were constructed to capture the significance of the data related to the research questions. The researchers explored the relationships between the categories, and constructed themes based on their meanings. Supervisors’ approval, colleagues’ support, connections/relationships with the residents, and attitude of the residents’ family were grouped as “interpersonal relationships during the pandemic.” Fourth, the themes were reviewed. The researchers reviewed the themes, categories, and coding to ensure that the categories and coding presented the themes appropriately. Categories were streamlined to ensure content conciseness, with those in the same theme exhibiting specific relationships. Moreover, contents of different themes were carefully curated to avoid overlap, allowing each theme to distinctly capture the unique aspects of the phenomena and effectively address research questions. Fifth, the themes were named according to the meanings of their contents. Altasi 6.0 was used for data analysis.
The researchers employed several strategies to ensure quality. First, the researchers established relationships to ensure the participants felt comfortable sharing their experiences and opinions. Second, audio was recorded to ensure the accuracy of data collection and the verbatim transcript was completed within 72 hr. Third, participants’ details and contexts were provided to other researchers to evaluate the transferability of the results. Fourth, the research teams included geriatrics, nursing, long-term care, and clinical psychology professionals who had more than 7 years of experience in long-term care. The researchers reviewed the results from multiple viewpoints to ensure confirmability. Additionally, feedback was solicited from four participants to provide insights from an insider’s perspective. The standards for reporting qualitative research (SRQR) guideline was used to report the study (O’Brien et al., 2014).
Findings
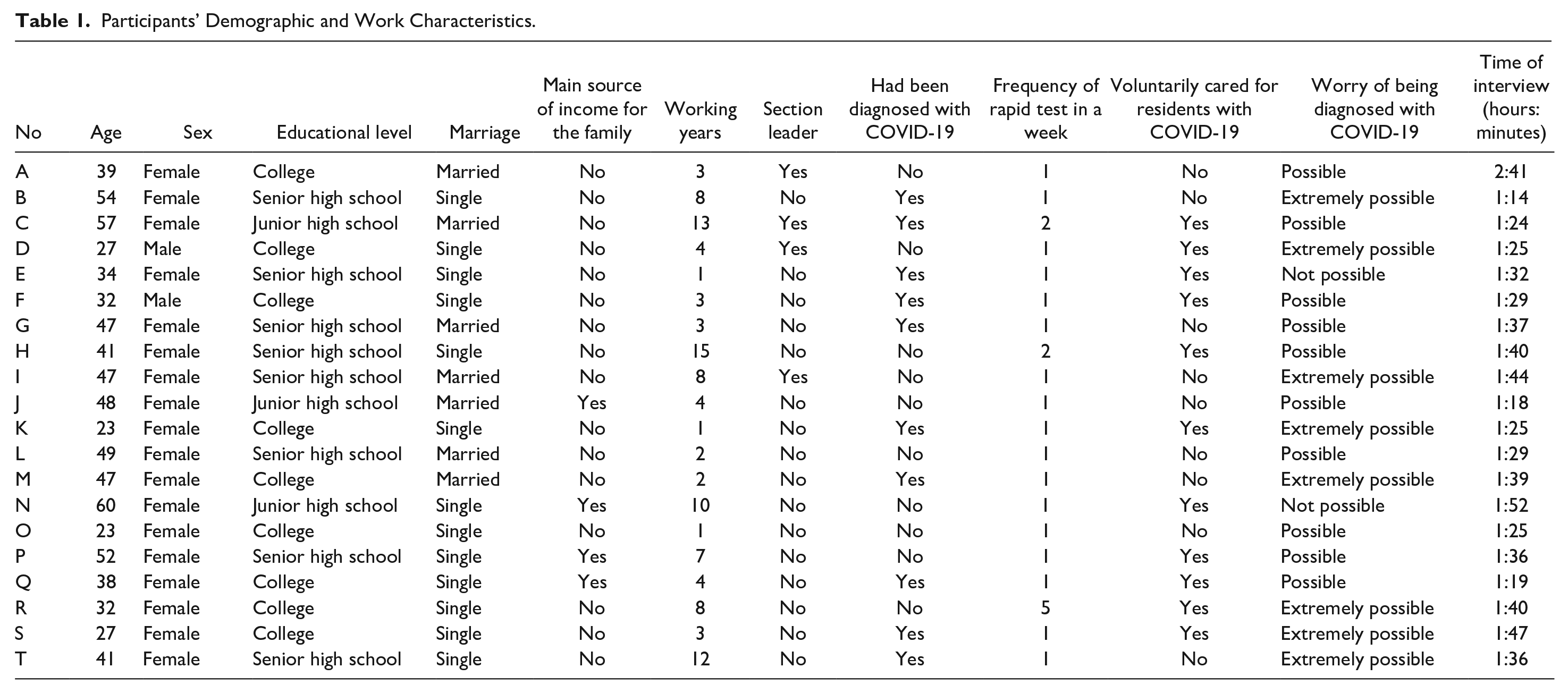
This study included 20 care aides. Of these, 18 were female, nine had college degrees, and four were the main source of income for their families. Ten had been diagnosed with COVID-19, and 11 had voluntarily taken care of residents with COVID-19. According to the epidemic prevention policy, staff in LTC institutions underwent routine rapid testing, with 17 receiving tests once a week (see Table 1).
Participants’ Demographic and Work Characteristics.
In total, four themes were identified, which included difficulties in care during the pandemic, psychological impact, interpersonal relationships, and policy on infection control (see Table 2).
Themes and Subthemes.

Theme 1. Difficulties in Care During the Pandemic
Difficulties in care during the pandemic included workload increase and a shortage of manpower owing to staff infections. Subsequently, institutions asked care aides to attend more shifts of work and reduced flexibility in work schedules. Difficulties in care had a major impact on care aides’ work satisfaction.
Physical Limitation Caused by Personal Protective Equipment
A significant stressor for care aides was the physical constraints imposed by PPE. PPE caused massive disturbances. Care aides had to wear an isolation gown, which was air-proof and covered the entire body and head, as well as a N95 mask and protective face cover. This caused difficulty in breathing and sweating. In addition, institutions set a quarantine area where they could not eat or drink, or go to the toilet. Furthermore, they could not go in and out of the quarantine area frequently. In addition, they worked 8–12 hr and could only stand.
C: It was so difficult to breath with full personal protective equipment, and I had to stand and could not go to toilet. I could go out two or three times a day, and I sweat a lot and all my clothes were wet. I felt exhausted after work. (57-year-old female participant, 13 years of working experience, section leader)
Work Overload
Several tasks increased the workload, such as wearing PPE, environmental cleaning and disinfection, and caring for residents with COVID-19, who had more care demands. In addition, some care aides were quarantined at home as they were infected. Others had to accommodate all the work and continue working without holidays. Therefore, they were overloaded with work.
R: The workload was much more than before, with personal protective equipment and all the complex care procedures. There was always a shortage in manpower. Many staff had COVID-19 and were quarantined at home for more than 10 days. It meant we could not take a day off and had to work these days. (32-year-old female participant, 8 years of working experience)
Impact of Work Schedule on Family Life
Care aides’ work schedule could not be fixed owing to unexpected diagnosis and shortage of manpower. Their work in shifts could change, and hence, they could not plan ahead. Sometimes they had to care for their family with care needs; however, the work schedule caused difficulties in their family lives.
M: I could not schedule the work and off days for a whole month. Many team members got COVID-19, and those who did not had to share the shifts and work. Therefore, I could not arrange my own life; even my mother had a chronic disease and needed care, but I could not take care of her. (47-year-old female participant, 2 years of working experience)
Theme 2. Psychological Impact
COVID-19 had major psychological impacts. In the early stage of the outbreak, care aides feared that COVID-19 was going out of control. Working in a quarantine area and social distancing brought a sense of social isolation. Care aides could not expect the end of the pandemic. In addition, the long-list infection control procedures resulted in burnout.
Worry of Infection Transmission
When the number of residents with COVID-19 surged because of nosocomial infection, care aides feared that the transmission had gone out of control. Subsequently, they were afraid the manpower could not meet the care demands, and the residents with severe physical conditions would die. In addition, they feared that they would bring the virus home and infect their families.
C: I was really scared at the beginning of outbreak; this [resident] had fever, and one infected the other; we were really busy. Many older residents had fever and their immune function was not well, and we were afraid that they would die. Many colleagues were diagnosed [with COVID-19] . . . and I had children (younger than six years old), but they did not have vaccine yet, I was really worried. (57-year-old female participant, 13 years of working experience, section leader).
D: Older residents in long-term care were at high risk for COVID-19, as we were too. I tried my best to protect myself, and I was very cautious. I did not want to increase my members’ workload. (27-year-old male participant, 4 years of working experience, section leader)
Social Isolation and Withholding Social Lives
Care aides who worked in quarantine areas experienced loneliness. They also feared that they transmitted the virus to others. Subsequently, they withheld their social lives and kept social distance. This reduced interactions with their families and friends. Boring lives and loss of social interactions had a negative impact on their mental health.
M: I would feel guilty if others got COVID-19 because of me, so I did not dare to go out. I got depressed imperceptibly, I did not have any social activities and I came home and locked myself in a room. (47-year-old female participant, 2 years of working experience)
I: When I was at the door of the quarantine area, I always felt stressed because of the isolation. I only interacted with the residents and team members (47-year-old female participant, 8 years of working experience, section leader).
Burnout Owing to Long-Lasting Infection Control Procedures
Strict infection control policy was a stressor. Various infection control procedures exhausted the care aides. If the patients increased and infection control policy continued, care aides could experience burnout.
F: Caring for patients with COVID-19 for a long time was quite stressful, and various aspects made me feel tired. If confirmed patients still appeared, the quarantine days would also be extended. How long would the pandemic and the preventive measures and quarantine last? I would think how long do I need to work in such a condition? It was so stressful. (32-year-old female participant, 3 years of working experience)
Theme 3. Interpersonal Relationships
Positive interpersonal relationships provided support for care aides. Supervisors’ approval made them recognize the value of care and colleagues’ support made them feel less lonely. Furthermore, good relationships with the residents improved their willingness to care. However, negative attitude from the residents’ families, such as blame, caused stress.
Supervisors’ Approval as One Source of Achievement
Although care aides faced great psychological stress during the pandemic, supervisors’ approval was a reason they could continue working. If supervisors could fully authorize and support care aides, facilitate communication to discuss and provide feedback, and recognize their efforts, the care aides could also recognize their work’s value and stay devoted.
I: The most important reason I could persist was the trust from the head nurse. She believed in me and supported what I did. If I had a suggestion, I could discuss it with her and modify the suggestion. I just finished my work, but she saw my effort. (47-year-old female participant, female, 8 years of working experience, section leader)
Colleagues’ Collaboration and Support
Care aides provided care as a team and had to collaborate with other care aides, nurses, and therapists. To improve care efficacy, care aides had to modify the care process and optimize team work. Hence, team cohesion also improved. A well working atmosphere provided mental support. With colleagues who worked together, care aides felt less lonely and could persist with their work.
F: During the pandemic, our team members were more willing to figure out problems and provide solutions. I could persist because of the team members. We worked together for so long under this situation, stuck together, and supported each other. If it were only me, I could not have held on. (32-year-old female participant, 3 years of working experience)
Relationships with the Residents as a Motivation for Caring
Some care aides cared for older residents for a long time each day for several years, and developed close relationships with them. Even when the residents got COVID-19, many care aides were still willing to take care of them. They thought the residents could not leave the institution because their families could not provide care, and they did not want the older residents to die of COVID-19. Therefore, they would pay more attention to the residents’ physical condition.
T: I voluntarily took care of older residents with COVID-19. They presented a pitiful sight; they were victims of the pandemic. I took care of them for four or five years and we had good relationships. I would be sad if they passed away because of COVID-19, so I paid close attention to them. (41-year-old female participant, 12 years of working experience)
P: Because of the preventive measures, the residents’ relatives could not enter the institution; and most of the time, the residents could only stay in their rooms or on the same floor. We were the only persons that the residents could interact with, and we took care of not only their physical needs but also their psychosocial needs. (52-year-old female participant, 7 years of working experience)
Criticisms from the Residents’ Families
Care aides faced many criticisms from the families of residents. When older residents who stayed in the institution got COVID-19, the families raised questions about the infection control and quality of care. Hospitals and long-term care institutions faced challenges of nosocomial infection. However, families had stricter standards for long-term care institutions than hospitals. Since families were consumers, they hoped the residents would receive the best care. However, this made care aides feel disappointed as they did their best yet did not receive fair feedback.
A: It was hard for the families to accept that the residents were diagnosed with COVID-19. They thought that it was our fault and that we would not have any problems because they had already paid the bills. Their criticism definitely affected my mood, and I worked so hard. It [the criticism] was unfair. (39-year-old female participant, 3 years of working experience, section leader)
Theme 4. Infection Control Policy
Regarding the infection control policy, it was important that the institutions have good infection control procedures and provide useful infection control education. Care aides believed they deserved a prevention bonus to compensate for their hard work.
Good Infection Control Procedures
Infection control procedures included materials and procedures. Care aides required materials, such as isolation gown, face masks, and PPE. The institutions provided enough material to make them feel safe. In addition, institutions planned infection control procedures on time, which included the environment and standard procedures regarding caring for residents with COVID-19. Subsequently, the care aides followed the procedures.
D: The materials were enough, and the institution could immediately provide what I needed. It was important that I protect myself on time. In addition, the sub-areas were well designed, and the residents and staff had no interaction with other areas, so COVID-19 did not spread quickly. (27-year-old male participant, 4 years of working experience, section leader)
Useful Infection Control Education
Infection control education helped care aides realize the symptoms of COVID-19 and the strategies to protect themselves and care for patients with COVID-19. Education decreased the fear of COVID-19.
C: Infection control education was helpful to understand the disease. Some older residents could not speak, and I watched for the symptoms. However, if I got COVID-19, then I knew how to deal with it. (57-year-old female participant, 13 years of working experience, section leader)
Insufficient Prevention Bonus
The Taiwan government and institutions provided a prevention bonus. However, care aides thought it was not enough. They felt they had too much workload, while shortage of manpower increased the physical and psychological burden. The prevention bonus was not commensurate to the time and energy the aides invested. They thought those who cared for residents with COVID-19 deserved an appropriate bonus.
K: The personal protective equipment and complex care procedures made us tired and exhausted; and when the manpower was not enough, we needed to take care of more residents. The institution or government did provide prevention bonuses, but I thought more were needed. (23-year-old female participant, 1 year of working experience)
Discussion
This qualitative study explored the working experiences of care aides in LTC institutions after the COVID-19 regulations were relaxed. Care aides encountered difficulties in care, including physical constraints caused by protective gear, workload, and impact of work schedules on their lives. They also suffered psychological impacts, such as worry, social isolation, and burnout. Regarding interpersonal relationships, positive aspects included supervisors’ approval, colleagues’ support, and relationships with residents. Negative aspects included criticism from residents’ families. Infection control procedures and education were useful. However, the prevention bonus was insufficient.
Data for this study were collected when COVID-19 regulations were relaxed and the number of patients with COVID-19 surged. Hence, the workload also increased. Similar to in previous studies (Sun et al., 2022; Yau et al., 2021), COVID-19 increased workload mainly due to COVID-19 prevention. PPE was essential for safety; however, it caused physical discomfort and was inconvenient for movement and physical needs. Conversely, care aides were also at risk for infection and had to be quarantined when infected, which resulted in a shortage in manpower. They had to meet the residents’ physical and care needs (Reynolds et al., 2022) and also provide mental support and relief to assuage their negative feelings (Yang et al., 2022). Furthermore, the workload-related stress extended to their family lives. They were worried about transmitting the virus to their families as well as in their social life, hence, they maintained social distance, which decreased their social activities. This affected their work–life balance (Fisher et al., 2021).
Previous studies revealed the impact of COVID-19 on psychological aspects among healthcare professionals (Hung et al., 2022; Lee et al., 2022; Palacios-Ceña et al., 2021). This study also revealed the negative psychological impact of COVID-19. Although care aides had encountered COVID-19 in 2021, they were relaxed and did not realize how large the impact was, such as how many residents would be infected and how long the preventive procedures would last. There was no clear end to the pandemic. Having to work with a high risk of COVID-19, they wanted to protect their families and friends, maintain social distance, and reduce social activities. This caused social isolation and loneliness (Capstick et al., 2022). Multiple factors increased the workload, such as use of PPE, complex procedures of care, longer worktime, and shortage of manpower. Worry and burden were the major psychological problems faced by care aides during COVID-19.
Care aides emphasized the importance of interpersonal relationships during the pandemic. In the work team, they required a supportive and cohesive atmosphere from the team to deal with the challenges and heavy workload. Therefore, approval from the supervisors and managers helped them feel that their directions were right. Teamwork with colleagues helped them deal with various challenges in care and in problem-solving (Capstick et al., 2022). In addition, good relationships with the residents proved to be a motivator. Care aides wanted older residents to recover quickly from COVID-19, especially since their families could not be with them. However, blame or criticism from families who did not understand the real situation in the institutions was a stressor. They also felt that the criticism was unfair as their effort was not visible.
Regarding clinical implications, a multi-level approach is necessary. As COVID-19 was a new infectious disease, care aides and healthcare professionals were unfamiliar with the transmission routes and preventive strategies. Educational training programs focusing on knowledge and skills were found to be beneficial for caring for residents with COVID-19 (Eltaybani et al., 2024). At the individual level, care aides must acquire knowledge and skills related to COVID-19 care and develop personal coping strategies for the psychosocial impact of the virus.
At the organizational level, institutions should ensure an adequate supply of materials for COVID-19 prevention. This would provide care aides with a sense of support, thereby reducing the risk of COVID-19 (Yau et al., 2021). Additionally, environmental redesign, such as separating COVID-19 patients from others and dividing buildings into different areas to minimize staff-resident interactions, could further mitigate the risk of transmission. Effective leadership and work management strategies are crucial for COVID-19 management (Dykgraaf et al., 2021). Institutions should provide care aides with standardized procedures for caring, observing symptoms, recording data, and responding to COVID-19 cases, along with modifications to the environment. Furthermore, governments should issue guidelines for care and preventive measures, along with providing prevention bonuses for frontline staff.
This study has some limitations. First, the participants were recruited from two institutions that shared the same institutional systems and management policy. Hence, the findings may not be applicable to other institutions. Second, care aides in this study understood the symptoms and transmission routes of COVID-19 and were familiar with the care procedures. Hence, their stress and concerns could be different. Future studies should conduct larger surveys on the needs and satisfaction of care aides. Furthermore, strategies for teamwork and management may also be explored.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the Ditmanson Medical Foundation Chia-Yi Christian Hospital (Grant Number: R113-CNGM-01) and the College of Medicine, National Cheng Kung University (Grant Number: CYC113003).
Ethical Approval
Ethics approval was obtained from the Institutional Review Board of Ditmanson Medical Foundation Chiayi Christian Hospital (IRB Number: IRB20220555).