
Abstract
Severe staff shortages, sustained stress, low compassion satisfaction, high compassion fatigue, and serious levels of burnout among healthcare workers were frequently reported during COVID-19. In this cross-sectional study with 760 care aides working in 28 LTC homes in Alberta, Canada, we used a two-level multilevel regression model to examine how working environments were associated with compassion fatigue, burnout, and compassion satisfaction measured with the Professional Quality of Life (ProQOL-9) scale. Our findings showed that higher compassion satisfaction and lower burnout were observed when care aides perceived a more supportive working culture. Care aides reported higher compassion fatigue when there was a lack of structural or staffing resources. We also found that perceptions of not having enough staff or enough time to complete tasks were significantly associated with higher levels of burnout. These findings suggest which elements of the working environment may be promising targets for improvement efforts.
• Provides a richer understanding of compassion fatigue among care aides in long-term care (LTC) settings. • Addresses a research gap on LTC working environments, focusing on which elements of the working environment influence care aides’ compassion fatigue, burnout, and compassion satisfaction. • Offers contextualized insight into how individual, unit, facility, and organizational factors can be predictable for burnout, compassion fatigue, and compassion satisfaction in LTC settings.
• This research finding highlights the importance of fostering workforce resilience through a supportive work culture, sufficient staffing, and structural resources. • Supportive work culture emerges as a modifiable environmental factor that is both economically viable and readily implementable in LTC settings. This environmental modification can mitigate the threats of workplace burnout and improve compassion satisfaction among the care aides. • The findings could inform policy changes at both organizational and governmental levels to improve working conditions in LTC homes through regular assessments of workplace culture and resources.What this paper adds
Application of study findings
Background
The psychological well-being of healthcare professionals has increasingly become a significant concern over the past 15 years (Bamforth et al., 2023). This well-being is profoundly influenced by compassion-related work life, a term encompassing physical, mental, and emotional challenges healthcare workers encounter in their daily interactions with patients. This concept includes both positive aspects, such as compassion satisfaction, and negative aspects, like compassion fatigue and burnout (Stamm, 1995, 2010). Compassion satisfaction is the pleasure that derives from effectively helping others or motivating them to offer help (Meadors et al., 2010). It inspires healthcare workers to improve patient care and believe they can make a positive impact (Slatten et al., 2011). Compassion fatigue, on the other hand, results from the stress of working in challenging situations or witnessing others’ pain or distress (Figley, 2013; Sorenson et al., 2016; Yu et al., 2016). For instance, oncology nurses often experience compassion fatigue after repeated exposure to patients’ suffering from the side effects of aggressive chemotherapy or those in the end stages of cancer (Potter et al., 2010). It is also called the “cost of caring” in the sense of negative consequences of caring for patients (Figley, 2002; Figley & Roop, 2006).
Burnout, an important element of compassion-related work life, significantly impacts healthcare professionals’ ability to provide empathetic and effective care. It is characterized by prolonged feelings of emotional exhaustion, hopelessness, and difficulties in performing jobs effectively (Braunschneider, 2013; Bride et al., 2007; Cañadas-De la Fuente et al., 2018; Slatten et al., 2011; Stamm, 1995). Burnout and compassion fatigue are interrelated; however, the development of burnout is gradual, while compassion fatigue can occur more rapidly (El-Bar et al., 2013; Hunsaker et al., 2015; Todaro-Franceschi, 2019). During COVID-19, many studies frequently reported severe staff shortages, sustained stress, low compassion satisfaction, high compassion fatigue, and serious levels of burnout among healthcare workers (Galanis et al., 2021; Garnett et al., 2023; Lluch et al., 2022; Richert & Zucchero, 2023; Sexton et al., 2022). A recent study in the United States (US) revealed that nearly half of the US healthcare workers experienced burnout and were searching for new jobs (Rotenstein et al., 2023).
In Canada, unregulated care aides or personal support workers constitute approximately 90% of the long-term care (LTC) workforce (Chamberlain et al., 2019). These workers are responsible for managing physical symptoms and providing emotional support to residents with complex needs (Fujisawa & Colombo, 2009; White et al., 2021). The COVID-19 pandemic exacerbated already difficult working conditions, introducing severe staffing shortages, severe resident isolation, and increased resident mortality (Titley et al., 2023; Wagner, 2020). Care aides experienced physical and emotional exhaustion due to heavy workloads (Reinhardt et al., 2022), staffing crises (Blanco-Donoso et al., 2021; Franzosa et al., 2022), inadequate infrastructure (Estabrooks et al., 2020), and insufficient safety measures (Estabrooks et al., 2020). Healthcare workers caring for COVID-19 patients reported higher levels of burnout, compassion fatigue (Cheung et al., 2022; Ruiz-Fernández et al., 2020), and secondary trauma (Egol et al., 2011; Vagni et al., 2020). Studies have shown that LTC nurses experience higher compassion fatigue when unable to provide sufficient support to residents (Kolthoff & Hickman, 2017; Shahar et al., 2019). However, research indicates that a supportive working environment can mitigate these negative outcomes, reducing compassion fatigue and burnout (Wu et al., 2016) and turnover intention (Marshman et al., 2022). Conversely, staffing shortages can increase workload, leading to higher burnout and lower job satisfaction (Kelly & Todd, 2017; Lee et al., 2020).
Identifying the elements of safe and supportive LTC working environments is essential if we are to make progress on reducing the negative consequences of compassion-related work life. The aim of this study is to investigate which elements of the LTC working environment are related to care aides compassion fatigue, burnout, and compassion satisfaction. To date, most empirical studies have investigated prevalence and levels of compassion fatigue (Hunsaker et al., 2015; Kartsonaki et al., 2023; Van Mol et al., 2015; Xie, Chen, et al., 2021; Xie, Wang, et al., 2021) and contributing factors (Oktay & Ozturk, 2022; Sprang et al., 2007; Xie, Wang, et al., 2021) among physicians and nurses in acute healthcare settings, for example, emergency, oncology, and intensive care units. Although substantial research addresses burnout in LTC settings (Chamberlain et al., 2017; Cooper et al., 2016; Duan et al., 2023; Gruneir et al., 2024), we located little evidence exploring compassion fatigue and its relationship with the working environment, revealing a critical gap in the literature. A better understanding of the relationship between compassion-related work lives and working environments will inform the development of targeted interventions aimed at enhancing working conditions, which, in turn, may improve the care experiences of care aides in LTC settings.
Theoretical Framework
This study incorporates the compassion fatigue concept, and the job demand-resource model. The concept of compassion fatigue guides us to understand how healthcare workers’ mental health is affected by prolonged exposure to patients in distress. According to this concept, the inability to assist patients during critical stages of illness over an extended period of time increases the risk of compassion fatigue and burnout among caregivers (Figley, 2013). This concept argues that empathetic engagement, while essential for patient care, paradoxically heightens a caregiver’s vulnerability to compassion fatigue (Figley, 2013).
The job demand job resource model (JD-R) was introduced to understand burnout in the workplace and explain how the organizational environment influences employee’s well-being. According to this model, every job involves demand and resources. High job demands lead to physical and psychological exhaustion when they exceed an employee’s capacity to cope. Increasing job resources can reduce workload and prevent burnout by allowing employees to cope with demands and stay engaged with organizational goals (Bakker & Demerouti, 2018; Demerouti et al., 2001). For example, a study showed that the growing demand for care in hospitals and long working hours was associated with higher burnout levels (Xian et al., 2020). Additionally, low work resources, such as insufficient social support and lack of rewards, were also linked to increased burnout.
In this study, the job demands and resource model guided us to hypothesize how working environment factors, such as lack of staffing, increase job demands and exacerbate burnout while reducing compassion satisfaction (Figure 1). Conceptual framework for care aides’ burnout, compassion fatigue, and compassion satisfaction.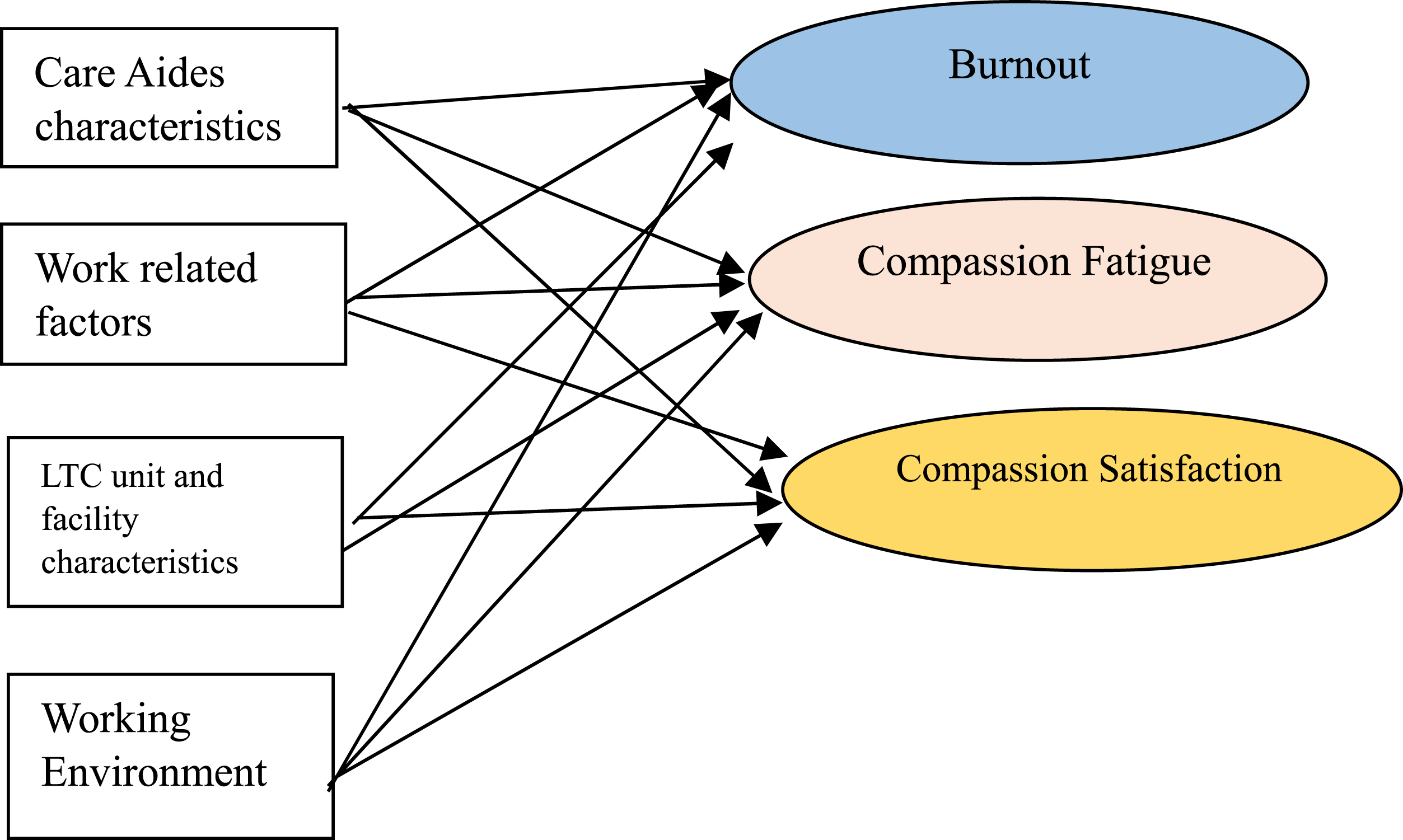
Methods
Design and Data Sources
We conducted a cross-sectional analysis using data collected from the Translating Research in Elder Care (TREC) program during the COVID-19 pandemic (August 2021 to February 2022). TREC is a longitudinal research program that investigates the impact of the organizational environment on best practices and on the health of both staff and residents in residential LTC settings. This cross-sectional study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline to ensure adequate reporting of study results (Von Elm et al., 2007).
Study Sample
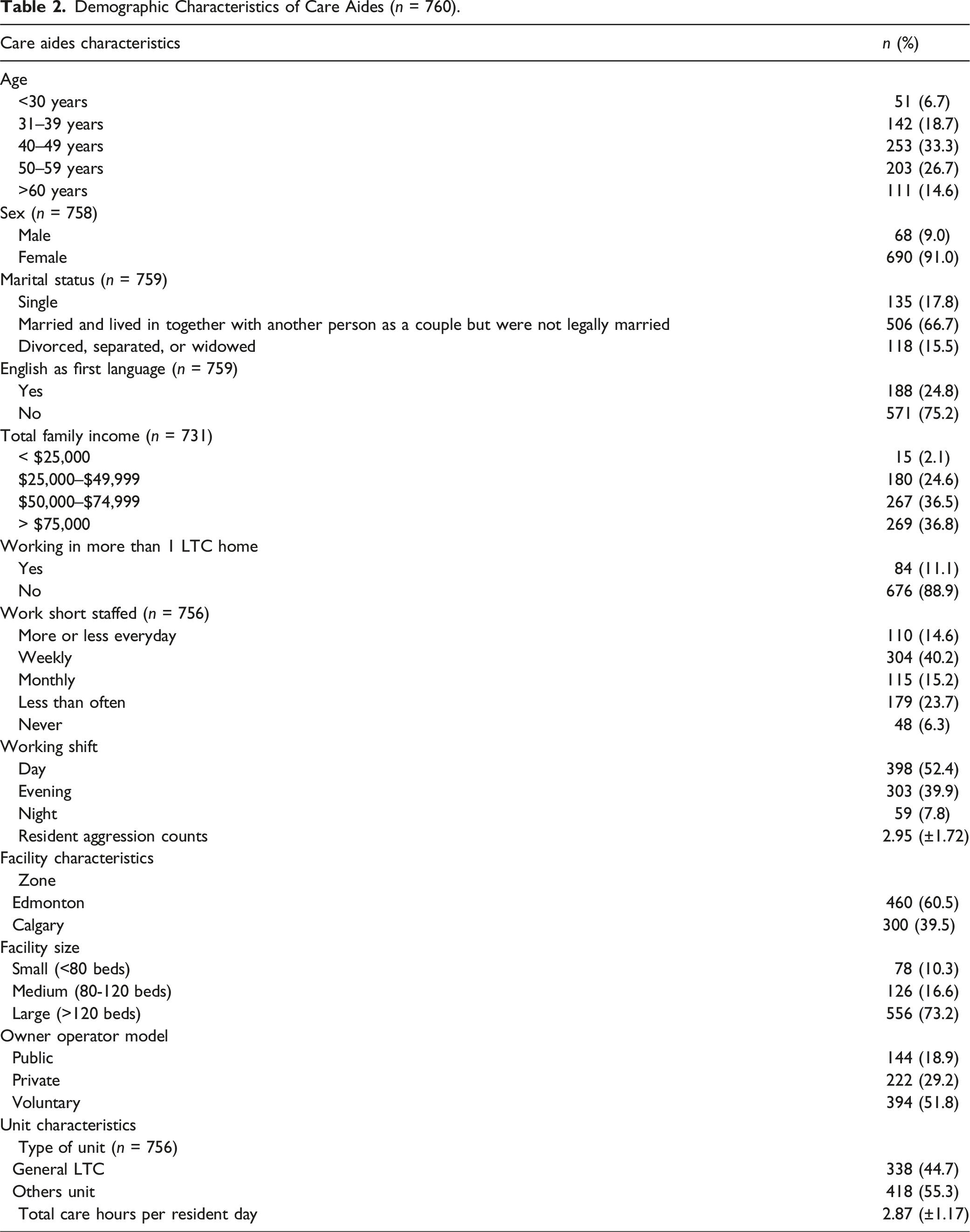
Our sample consisted of 760 care aides working in 98 care units within 28 LTC homes in Alberta, Canada. LTC homes were chosen using a stratified random sampling method, with strata being region, facility size, and the owner operator model. Care aides working in the selected LTC homes were invited in person to participate in the TREC care aide survey if they had a minimum of 3 months of experience working in the same care unit and completed at least six shifts every month. Trained interviewers completed virtual structured interviews with participants via Zoom. In our study, a total of 760 care aides (eligible sample n = 2241) voluntarily participated, yielding a response rate of 33.92%. This response rate in TREC was lower than usual, likely due to the survey being conducted during one of Alberta’s worst COVID years in 2021.
Variables and Measures
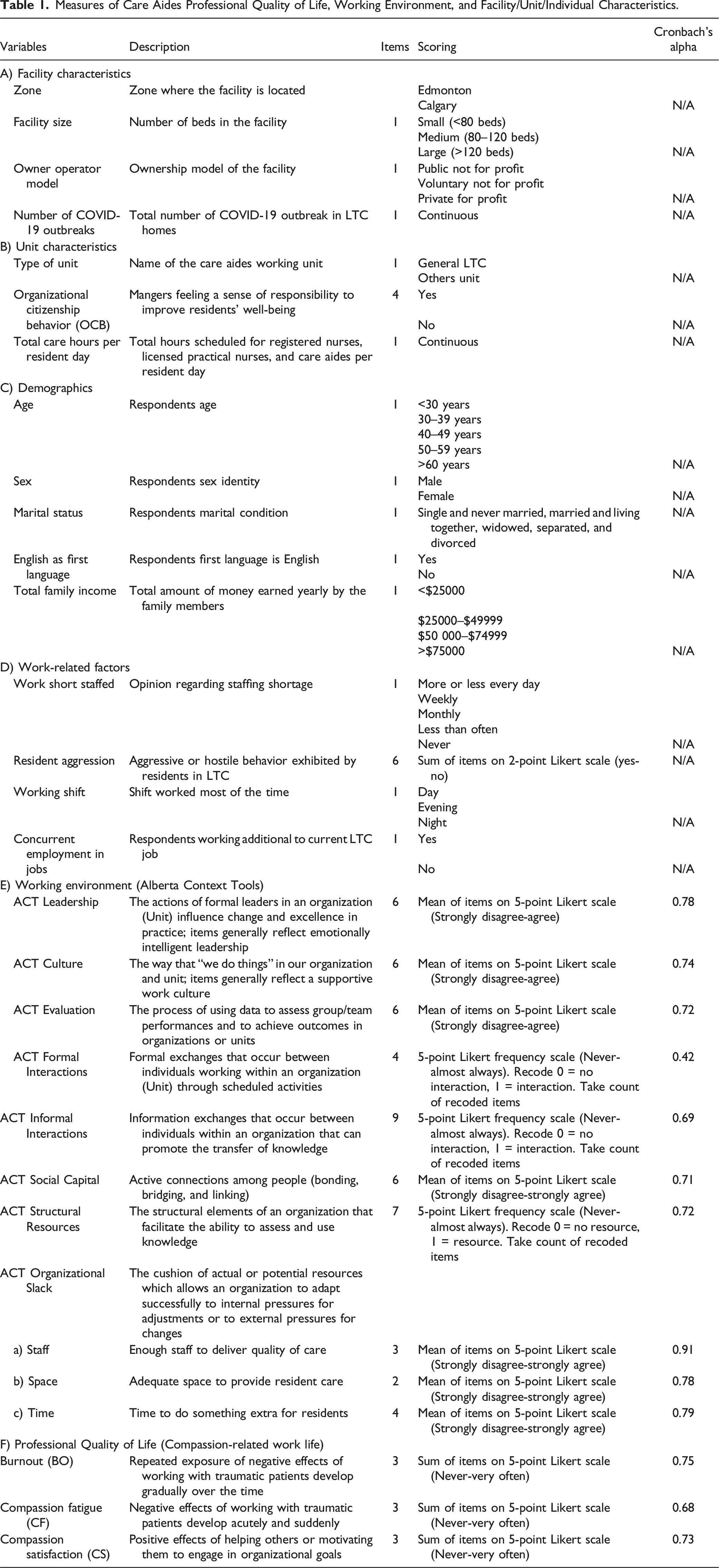
Measures of Care Aides Professional Quality of Life, Working Environment, and Facility/Unit/Individual Characteristics.
Professional Quality of Life (ProQOL-9)
Care aide burnout, compassion fatigue, and compassion satisfaction were measured with the Professional Quality of Life-9 (ProQOL-9) (Galiana et al., 2020). ProQOL-9 is a 9-item validated instrument developed from the original and longer ProQOL IV and ProQOL V. Each of the three subscales is made up of three items on a 5-point Likert scale (1 = never to 5 = very often). Respondents were asked to identify how frequently they have had the experience described by each item in the past 30 days. Scores for each subscale are measured by summing up three items. The ProQOL-9 has been previously assessed for reliability and validity among palliative care professionals. Cronbach’s alpha scores were 0.83 for burnout, 0.82 for compassion fatigue, and 0.84 for compassion satisfaction (Galiana et al., 2020).
Work Environment (Organizational Context)
We used the Alberta Context Tool (ACT) to measure organizational context at the clinical microsystem (care unit) level (Estabrooks et al., 2009). The ACT has 10 concepts, including leadership, culture, evaluation (data feedback processes), formal and informal interactions, social capital, structural and electronic resources, and organizational slack (staffing, space, and time). Each item is measured on a 5-point Likert scale. Each scale score for leadership, culture, evaluation, social capital, and organizational slack in staffing, space, and time is obtained by taking the average of its items. Scores for formal interactions (range 0–4), informal interactions (range 0–9), and structural resources (range 0–7) are calculated by taking the count of recoded items. Previous studies have reported that the ACT is a valid and reliable instrument used for care aides in LTC with a Cronbach’s alpha being 0.70 for 8 of 10 concepts (Estabrooks, Morgan, et al., 2011; Estabrooks, Squires, et al., 2011).
Statistical Analysis
We used descriptive analyses to examine the characteristics of care aides, units, and facilities. We used a two-level random intercept linear regression analysis (to adjust for the clustering of care aides within units) to examine the relationships between the work environment and care aides’ burnout, compassion fatigue, and compassion satisfaction. Our adjusted models controlled for care aide, unit, and facility characteristics (see Table 1). We initially developed a three-level model as our care aides nested in units and units nested in facilities (Hox et al., 2017). We excluded the facility level from our final model because it showed a low intra-class correlation at the facility level (ICC <0.001), thus leaving a two-level model. All 10 context variables were included in the models, as the variation inflation factors (VIF ≤ 1.8) indicated no issues of multi-collinearity (Harris, 2021). In our model, we used listwise deletion to deal with missing cases as there were less than 5% of missing data (Madley-Dowd et al., 2019; Schafer, 1999). We conducted linear regression analyses separately for each ProQOL subscale (burnout, compassion fatigue, and compassion satisfaction). The conditional pseudo-R2 value was used to assess model fitness, and the analyses were carried out with SPSS-28 version (IBM Corp N, 2017).
Ethics
We obtained ethics approvals from the University of Alberta Health Research Ethics Board (Pro00037937).
Results
Demographic Characteristics of Care Aides (n = 760).
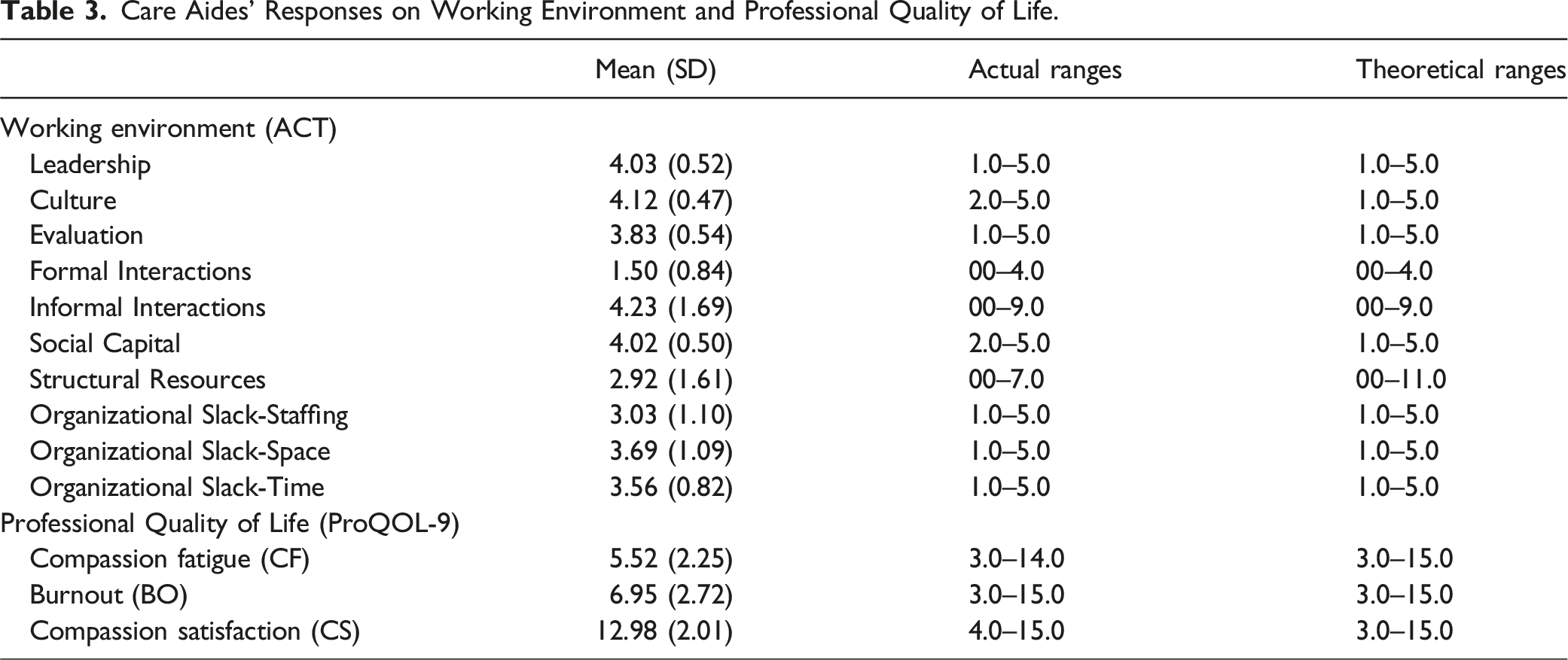
Care Aides’ Responses on Working Environment and Professional Quality of Life.
Compassion-Related Work Life Among Care Aides in LTC Homes.
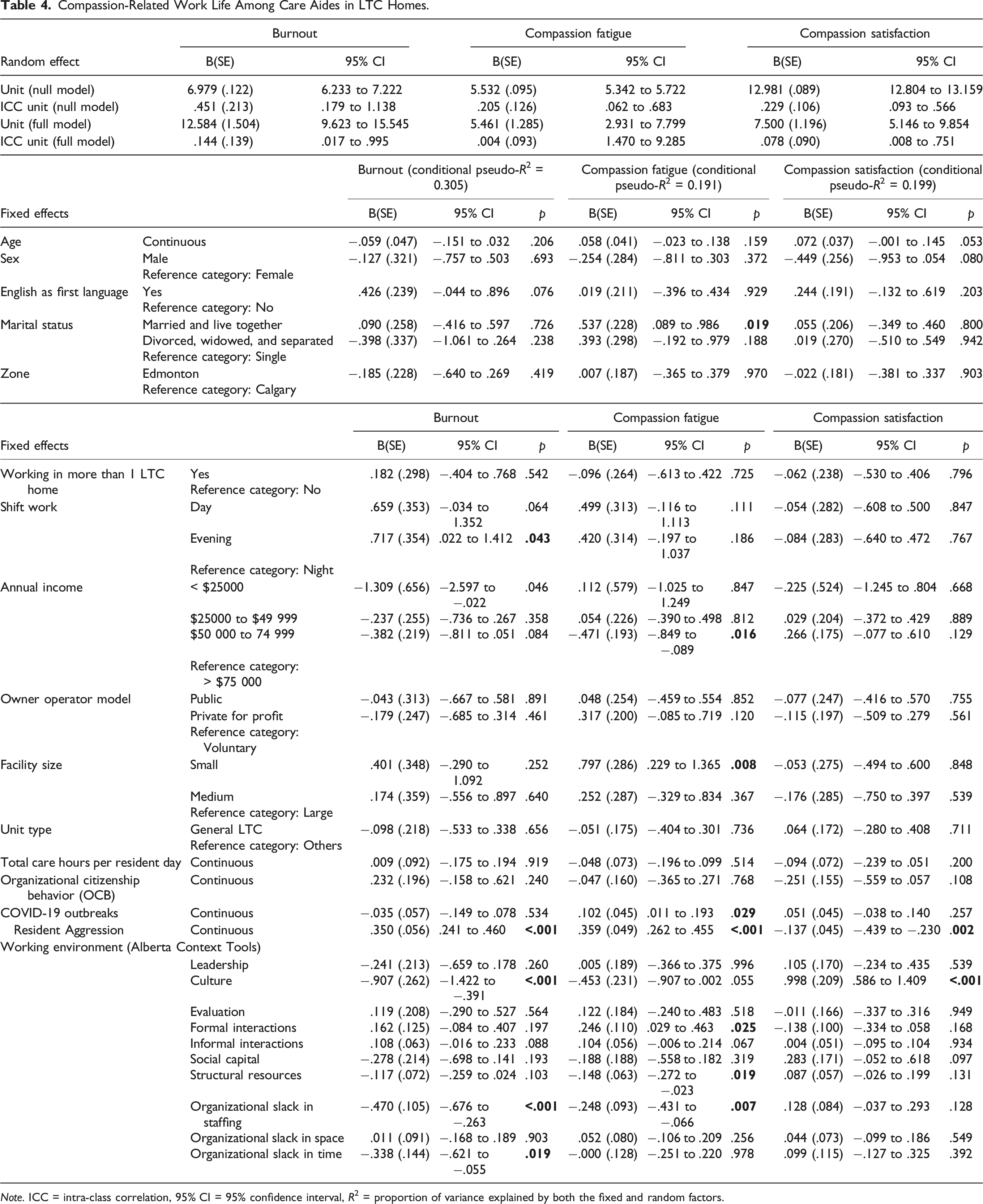
Note. ICC = intra-class correlation, 95% CI = 95% confidence interval, R2 = proportion of variance explained by both the fixed and random factors.
Discussion
Our study fills a critical gap in the literature by providing insights into which elements of the working environment influence compassion fatigue among workers in LTC settings. We found that a supportive work culture was strongly associated with higher compassion satisfaction and lower burnout among care aides. In contrast, compassion fatigue was linked to inadequate structural and staffing resources. Furthermore, care aides who perceived staffing shortages or insufficient time to complete tasks reported significantly higher levels of burnout, highlighting the impact of resource constraints on their psychological well-being.
A working environment can be called supportive or positive when it promotes a culture of teamwork, recognition, autonomy, and professional development (Estabrooks et al., 2009). In our study, care aides reported burnout and compassion fatigue may be due to a lack of supportive organizational cultures in their workplace. When employees feel unsupported, particularly in emotionally demanding roles like caregiving, it can contribute to feelings of isolation and disempowerment, which are key factors in burnout (Maslach & Leiter, 2016). A systematic review of organizational culture among nurses showed that a positive or supportive organizational culture is significantly associated with reducing work-related stress (Kiptulon et al., 2024). Similarly, critical care nurses reported that workplace recognition significantly enhanced compassion satisfaction and decreased burnout (Kelly & Lefton, 2017). While our study did not reveal particular organizational culture elements associated with burnout and compassion fatigue, future research should concentrate on the components of supportive cultures that address these challenges. Furthermore, interventions such as team-building, recognition programs, and professional development opportunities should be designed and tested for their usefulness in improving care aides’ well-being and job satisfaction.
Adequate staffing is an important component of a positive work environment and has long been identified as a major contributor to employee burnout. A substantial body of research suggests that insufficient staffing levels place an extra burden on current employees, leading to emotional exhaustion and subsequent burnout (Chemali et al., 2022; Konstantinou et al., 2018; Kowalski et al., 2010; Søvold et al., 2021; Toh et al., 2012; Tsolekile et al., 2015). The job demands–resources model of burnout argues that when job demands are high and resources (staff) are low, stress and burnout increase (Demerouti et al., 2001). Staffing in Canadian long-term care homes is particularly difficult, with a heavy reliance on part-time caregivers. A study recommends increasing permanent staff to address staffing shortages in long-term care facilities (Franzosa et al., 2022).
We argue that care aides may feel compassion fatigue due to their inability to help residents because of increased workload and insufficient staff. This was supported by another finding from our study, where care aides’ perception of a lack of time to implement best practices was associated with higher levels of burnout. Having perception of sufficient time for extra tasks and collaborative discussions about best practices were linked to lower levels of burnout (Cooper et al., 2016) and increased job satisfaction (Chamberlain et al., 2016). Heavy workloads limit care aides’ opportunities for meaningful interactions with residents (Mallidou et al., 2013). Because of their substantial workloads, care aides tend to complete their duties without engaging in meaningful interactions with residents (Wiersma, 2012).
Our study indicates that a scarcity of structural resources, including clinical guidelines, textbooks, and notice boards may contribute to increased levels of compassion fatigue. While compassion-related research is limited in LTC working environments, some studies found correlations between structural resources and burnout in other settings. For example, lack of structural resources in LTC homes was correlated with burnout among care aides (Chamberlain et al., 2017). During the COVID-19 pandemic, clinical guidelines served as psychological safeguards for nurses (Maiorano et al., 2020), whereas emergency healthcare workers reported elevated levels of burnout when faced with insufficient resources (Blanchard et al., 2022).
We reported that care aides who participated in formal interactions, such as team meetings and family conferences, experienced higher levels of compassion fatigue. While no direct evidence explicitly linking formal interactions to this outcome has been identified in previous research, studies highlighted that excessive empathetic engagement with patients and their families contributed to significant emotional exhaustion (Anderson et al., 2019) and compassion fatigue among healthcare workers (Nishihara et al., 2022). Engaging in conversations with family members about a patient’s declining health, persistent pain, or approaching end-of-life can be emotionally challenging for healthcare workers, often evoking feelings of helplessness, profound grief, and emotional exhaustion. Further research is needed to explore the direct impact of these formal interactions on caregiver well-being.
Limitations
Our study had some important limitations. First, generalizations can only be made for care aides working in LTC homes, similar to those reported here. Second, we may have had a significant response bias because of low response rate. Third, as the study is cross-sectional, we were unable to make any causal claims regarding the relationships between the LTC working environment and compassion fatigue, burnout, and compassion satisfaction. Fourth, survey data may be subject to recall biases or social desirability biases. The study is further limited to the context of the COVID-19 pandemic, which may have unique effects on the working environment and psychological outcomes of care aides.
Conclusion
Less supportive work culture was correlated with higher burnout and lower compassion satisfaction, while insufficient structural or staffing resources were linked to increased compassion fatigue. Perceptions of insufficient staffing and time constraints were also associated with higher levels of burnout. These findings highlight the critical importance of a positive and supportive work environment in preventing compassion fatigue and burnout in this frontline caregiving workforce through future intervention. A more stable and resilient workforce is likely to provide higher quality care to residents and enhance workforce retention.
Footnotes
Acknowledgments
The authors express gratitude to Heather Titley, PhD, for her continuous support in coordinating the study, as well as to the TREC team for their contributions to the research. Additionally, Joseph Akinlawon, the data manager, supplied relevant information concerning the TREC data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Alberta Ministry of Health (AHW011810 Estabrooks) and the Canadian Institutes of Health Research (CIHR) (RES0053356).