
Abstract
Research on functional outcomes in long-term care (LTC) home residents after COVID-19 infection is limited. In the current study, we examined outcomes in 1,310 LTC residents with a positive COVID-19 test in the period from March 2020 to April 2022 (“COVID” group). We also reviewed outcomes in residents in the same LTC homes without a history of COVID-19 during the same period (“No-COVID” group, n = 2,301). In a retrospective longitudinal design, we explored activities of daily living (ADLs), cognitive function, and clinical care needs over time. Change was assessed from the last assessment before contracting COVID-19 to three assessments subsequent to COVID-19, over on average seven months after infection. We found deterioration over time in ADLs and cognitive performance in both groups. The change in ADLs and clinical care needs was slightly greater in the COVID than the No-COVID group from baseline to the first follow-up assessment; in subsequent assessments, the change was similar in both groups. Overall, we observed similar functional outcomes among surviving residents in the two groups, with initially greater deterioration in ADLs and clinical care needs in residents with a history of COVID-19 followed by a trajectory resembling the one in the No-COVID residents.
Adverse effects of the COVID-19 pandemic in long-term care (LTC) residents have been documented worldwide (Amore et al., 2021; Betini et al., 2021; Mas Romero et al., 2020). Due to multiple interrelated factors, such as advanced age, comorbidities, communal living, and complex care needs, LTC home residents were particularly vulnerable in the pandemic circumstances. Of utmost importance in LTC during the pandemic was prevention of outbreaks and mortality among residents, also reflected in a predominant research focus on these topics. More recently, research about consequences of COVID-19 and trajectories of recovery in longer periods after COVID-19 infection has been emerging, including Cortés Zamora et al. (2022), Greco et al. (2021), Pérez-Rodríguez et al. (2021), and van der Krogt et al. (2022).
In the first wave of the pandemic, Pérez-Rodríguez et al. (2021) reported a high rate of functional, cognitive, and nutritional decline in 435 LTC residents, with no differences found between residents with and without COVID-19 in a 1-month follow-up. In a 3-month follow-up of 215 residents at the start of the pandemic, Cortés Zamora et al. (2022) found a significant psychological impact on COVID-19 survivors and a functional decline in residents regardless of COVID-19 status. Greco et al. (2021) reported, also in the first wave of the pandemic, increased frailty and decreased physical performance in 76 residents with COVID-19 and decline in cognitive performance that was similar in infected and non-infected residents. In 86 residents with COVID-19 at the pandemic’s start, van der Krogt et al. (2022) reported that in most residents initial deterioration in functioning was followed by recovery at three months after infection; however, activities of daily living (ADL) functioning remained lower compared to the baseline, and symptoms such as fatigue and sleeping problems were present.
Overall, the majority of these studies included residents that contracted COVID-19 in the early phases of the pandemic (in 2020), the studies were characterized by short follow-up times (up to three months), and the follow-up assessment was conducted at a single time point. When multiple follow-up points were included (van der Krogt et al., 2022), only residents with COVID-19 were followed, and the health changes over time after COVID-19 could not be delineated from the changes expected in the general LTC population. In the current study, we expand on the previous research and address some of its limitations, to provide more evidence and inform clinical and care practices for residents in LTC.
The Current Study
We investigated clinical care needs and recovery of ADLs and cognitive function in LTC home residents with a history of COVID-19, assessed at multiple time points, including baseline (prior to a positive COVID-19 test) and three time points following the test. We assessed change in these variables from the baseline assessment to each of the follow-up assessments. Residents in the same LTC homes without a positive COVID-19 test in the same period were also included in the study; therefore, we reviewed relevant outcomes and change over time in the residents with and without a history of COVID-19. Adding to the existing literature, this study involves a larger sample of residents with COVID-19, a longer period during the pandemic, and a longer post-COVID-19 follow-up time.
Method
Participants
We examined post-COVID-19 outcomes in publicly funded residents in 19 LTC homes affiliated with the Fraser Health Authority (FHA), one of the five regional health authorities in British Columbia (BC). All homes reported COVID-19 infections among residents during the study period. Residents residing in these LTC homes at any time from March 01, 2020 to April 30, 2022 (the study inclusion period) were eligible to participate in the study. Residents who had a positive COVID-19 test 1 during the study inclusion period comprised the “COVID” group and residents in the same LTC homes that did not test positive for COVID-19 during this period comprised the “No-COVID” group. Only residents who had a Resident Assessment Instrument-Minimum Data Set 2.0 (RAI-MDS 2.0) assessment conducted within 6 months before the follow-up start date were included in the study (N = 3,611, 84% of all residents)—with the final study sample consisting of 1,310 residents in the COVID group and 2,301 in No-COVID group. Transitions/transfers within the system, changes in funding status, and contracting COVID-19 before the first assessment were common reasons for not having a baseline assessment.
Data Sources
All the data were collected retrospectively from the FHA data sources. Information about COVID-19 testing and the test results was obtained from the BC Population and Public Health in FHA, and other information was collected from administrative databases and RAI-MDS 2.0 records. The RAI-MDS 2.0 assessment is typically conducted with LTC residents quarterly (or more frequently if needed) as a part of regular care. The provincially mandated assessment is conducted by trained LTC personnel. Ethical approval for the study was received from the FHA Research Ethics Board.
Measures
Resident’s ability to perform ADLs was measured by the ADL Scale—Long Form (InterRAI, 2023; Morris et al., 1999). The scale taps into seven activities pertaining to personal hygiene, dressing, eating, and bed mobility. The activities are assessed on a 5-point scale, with the endpoints defined as 0 = independence and 4 = total dependence. The scores are summed into a total score (“ADL score”) ranging from 0 to 28, and higher scores indicating higher level of dependence for ADL assistance. Resident’s cognitive function was measured by the Cognitive Performance Scale (InterRAI, 2023; Morris et al., 1994), which includes activities such as making self understood, daily decision-making, and independent feeding. The final “CPS score” is a 7-point scale, from 0 = intact to 6 = very severe impairment, with higher scores indicating a lower level of cognitive function. As indictors of resident clinical care needs, we used Resource Utilization Groups (RUG) III methodology (Canadian Institute for Health Information, 2016; Fries et al., 1994) and information about medications and treatments received. The RUG III maximum category score classifies residents in seven ordered categories (from reduced physical function to special rehabilitation). In this study, we used a dichotomous “RUG score,” with the score 1 representing four categories (special rehabilitation, extensive services, special care, and clinically complex) and indicating higher clinical care needs, and the score 0 representing the other three categories (reduced physical function, behavior problems, and impaired cognition). “Medications” was defined as the number of different medications taken by a resident during seven days before assessment. “Treatments” was a dichotomous variable with the score 1 indicating that resident was receiving at least one of the specialized treatments within seven days before assessment (including oxygen therapy, IV medication, renal dialysis, chemotherapy, ventilator) and score 0 indicating not receiving any of these treatments in the seven days preceding assessment.
Study Design and Procedure
For each resident in the COVID group, we obtained information from the last RAI-MDS 2.0 assessment before the positive COVID-19 test date, which served as a baseline assessment (labeled PRE). The same information was then collected from the first three assessments subsequent to the date of their positive COVID-19 test (labeled POST1, POST2, and POST3), the latest until January 31, 2023. This process is depicted in Figure 1. Information was collected from only three assessments subsequent to contracting COVID-19, because only up to three post-COVID assessments were available for residents who contracted COVID-19 in 2022. Out of the residents who had a valid PRE assessment, POST1 was available for 1,034 (79%) of residents, POST2 for 919 (70%) of residents, and POST3 for 795 (61%) of COVID group residents. The main reason for the decreasing number of assessments/participants over time was mortality (e.g., residents who had a valid PRE deceased before POST1, or residents with PRE and POST1 deceased before POST2, etc.). Other reasons for missing POST assessments, in a small number of cases, was moving from the LTC home or incomplete/invalid assessments. On average, PRE assessment in the COVID group was conducted within two months before the positive COVID-19 test date (M = 1.7, SD = 1.1). The mean time from the test date to POST1 was 1.4 months (SD = 0.8), to POST2 4.4 months (SD = 1.1), and to POST3 7.2 months (SD = 1.2).
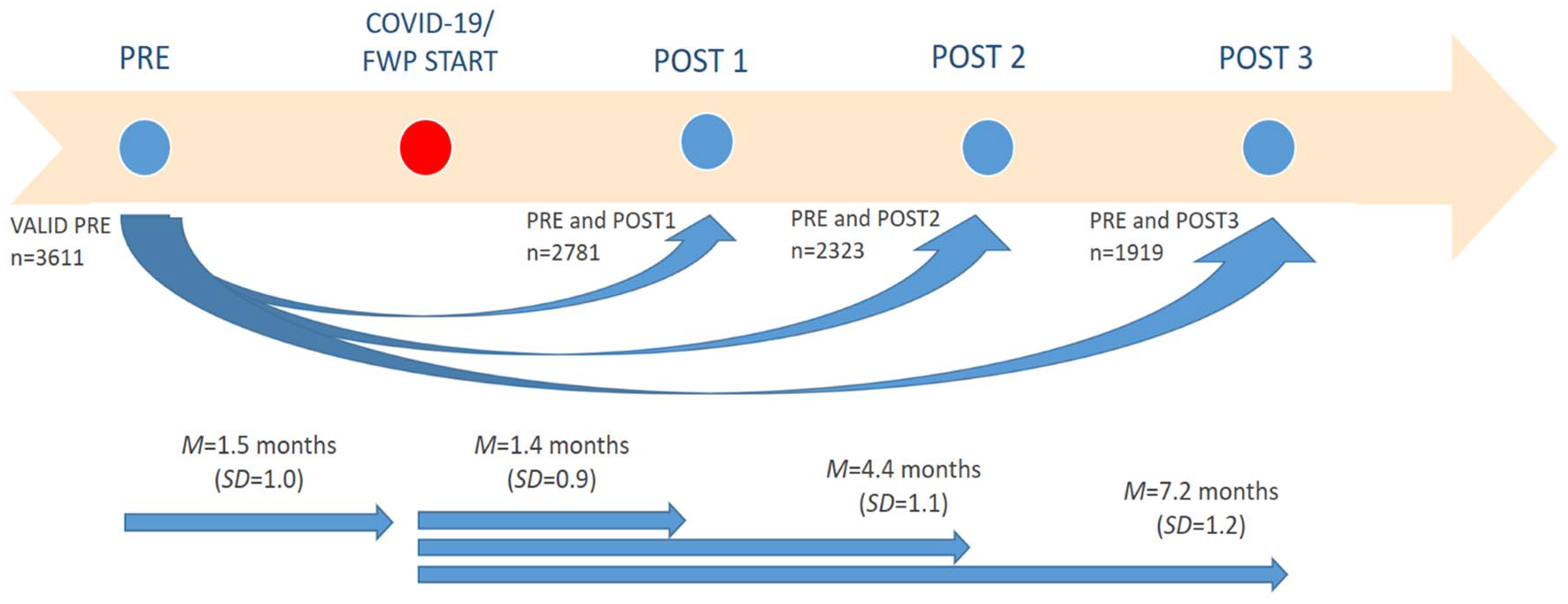
Data collection procedure. “PRE” stands for the last assessment before contracting COVID-19 or before the follow-up [FWP] start in No-COVID group. “POST1,” “POST2,” and “POST3” are three assessments subsequent to contracting COVID-19 or FWP start. Decreasing number of residents from PRE to POST1, POST2, and POST3 was result of mortality between the assessments.
Similarly, in the No-COVID group, PRE and three POST assessments were collected relative to a randomly selected follow-up start date (a date randomly selected for each resident within the study inclusion period). 2 In the No-COVID group, the length of time from follow-up start to the assessments was similar as in COVID group: to PRE assessment M = 1.4 months (SD = 1.0); to POST1 1.4 months (0.9); to POST2 4.4 months (1.1); to POST3 7.2 months (1.2)—with POST1, POST2, and POST3 obtained for 1,747, 1,404, and 1,124 residents, respectively. A subgroup of No-COVID residents contracted COVID-19 after April 30, 2022 (during the follow-up period). For these residents (n = 371), we ended their follow-up at the date of their positive COVID-19 test—no information was considered after this date, while information from the period before contracting COVID-19 was retained.
Data Analysis
We described the outcome variables at all assessment points. Our focus was on studying change in each variable from the PRE assessment (baseline scores) to each of the POST assessments in the COVID and No-COVID group. To assess the differences in change between the two groups, we used mixed design ANOVA (with a between- and within-subjects factor) and assessed the interaction effects between the factors. For dichotomous variables, nonparametric testing (chi-square test and McNemar test) was utilized to assess differences between the groups and over time. In multivariate analyses, we investigated follow-up outcomes in the two groups while adjusting for relevant covariates (i.e., age, sex, and the baseline scores)—we used multivariate linear regression or logistic regression, depending on the nature of the dependent variable. Multivariate residuals were examined to address the assumptions of the statistical models and ensure validity of the results.
Results
Resident Characteristics
Out of all 3,611 residents, 59% were female (40% male and 1% other), the mean age at the time of admission to the LTC home was 82.5 years (SD = 10.8) and at the PRE assessment 84.8 years (SD = 10.5). In PRE assessment, the average ADL Score was in medium ADL functioning range (M = 16.1, SD = 8.4) and the CPS Score in moderate cognitive impairment range (M = 2.9, SD = 1.6). According to the RUG III maximum category classification, the reduced physical functions category was the most frequent (57.5% residents), followed by impaired cognition (19.3% residents). Less than a quarter of residents (19.4%) were classified in the four highest clinical care needs categories (i.e., special rehabilitation, extensive services, special care, clinically complex). The majority of the residents (90%) were not receiving any of the given specialized treatments, while the average number of medications during seven days before assessment was 8.2 (SD = 4.1). For greater detail about resident characteristics, in the two groups and over time, see Table 1S (Supplemental Materials).
At the positive COVID-19 test date, COVID group residents were on average 85.0 years old (SD = 9.9) and 58% female, similar to age and sex distributions in the No-COVID group at the follow-up start, age 84.9 years (SD = 10.8), 60% female. About mortality, 240 residents (18.3%) died in the first month after positive COVID-19 test (all-cause mortality). Information about COVID group mortality was available for the 9-month period after infection—during this time 417 (31.8%) of residents died.
Functional and Clinical Care Outcomes
Distributions of the outcome measures scores and the change in the mean scores from baseline assessment to each of the follow-up assessments in the COVID and No-COVID group are visualized in Figures 2 to 5. Greater detail about the scores in all assessments and the results of the statistical tests (if not provided in the text in this section) is included in Supplemental Materials.

Distribution of the Activities of Daily Living (ADL) scores (a–c) and change in the mean ADL score from PRE to POST assessments in the two groups (d–g). The change in the COVID group is depicted by green and in No-COVID group by blue line. In PRE-POST1 graphs, n is the number of residents with PRE and POST1; in PRE-POST2 n = residents with PRE and POST2 (smaller n, due to mortality after POST1); and in PRE-POST3 n = residents with PRE and POST3 (smallest n, due to mortality after POST 1 or POST 2). The PRE-POST3 was further broken down into PRE-POST1-POST2-POST3 (residents who had all assessments).

Distribution of the Cognitive Performance Scale (CPS) scores (a–c) and change in the mean CPS score from PRE to POST assessments in the two groups (d–g). The change in the COVID group is depicted by green and in No-COVID group by blue line.

Change in the Resource Utilization Groups (RUG) score (a–c) and Treatments score (d–f) from PRE to POST1, POST2, and POST3 in COVID and No-COVID group.

Distribution of the Medications score (a–c) and change in the mean score from PRE to POST assessments in the two groups (d–g). The change in the COVID group is depicted by green and in No-COVID group by blue line.
ADLs
There was an increase in the mean ADL score (indicating declining functional status) from PRE to POST1, from PRE to POST2, as well as from PRE to POST3 (all p-values <.001, medium effect size—η2 from 0.05 to 0.12). The increase in the ADL score from PRE to POST1 was greater in the COVID group than in No-COVID group, F (1, 2779) = 9.91, p = .002, while the change from PRE to POST2, and from PRE to POST3 was similar in the two groups (Figure 2d–f). After adjusting for age, sex, and the ADL score in the PRE assessment, the results confirmed a statistically significant positive relation between COVID and the ADL score in POST1 assessment, b = 0.45, p = .005, β = .03, and no relation between COVID and the ADL score in POST2 or POST3 assessment.
Cognitive Function
In the overall analyses, there was an increase in the mean CPS score (indicating a decrease in cognitive function) from PRE to POST1, from PRE to POST2, as well as from PRE to POST3 (all p-values <.001, small effect size—η2 from 0.01 to 0.02). The change in the CPS score from PRE to POST assessments in the COVID and No-COVID group was similar (Figure 3d–f), with no statistically significant differences found. After adjusting for the baseline CPS score, age, and sex, there was no statistically significant relation between COVID and the CPS score in any of the POST assessments.
Clinical Care Needs
In the COVID group, there was a statistically significant increase from PRE to POST1 assessment in the number of residents with the high RUG score (from 14.1% to 20.3%, p < .001), indicating higher clinical care needs in POST1, while the change in the No-COVID group was not statistically significant (from 17.9% to 18.6%). Similarly, the number of residents receiving one of the specialized treatments increased in the COVID group from PRE to POST1 (from 9% to 14.4%, p < .001) while remaining similar in the No-COVID group (from 9.5% to 9.7%). The change from PRE to POST2 and POST3 was similar in the two groups in relation to both RUG score and Treatments (Figure 4). After adjusting for age, sex, and PRE RUG score, the results confirmed a statistically significant relation between COVID and the RUG score in the POST1 assessment, b = 0.37, p = .002, exp(b) = 1.44, and no relation between COVID and RUG score in POST2 or POST3. Similarly, there was a statistically significant positive relation between COVID and Treatments at POST1, b = 0.76, p < .001, exp(b) = 2.14, and no relation between COVID and Treatments at POST2 or POST3, after adjusting for covariates and Treatments at baseline.
The mean number of medications remained similar over time in the two groups (Figure 5d–g). After adjusting for the covariates and the number of medications at baseline, there was no relation between COVID and Medications in any of the POST assessments. A small increase in the mean number of medications in overall analysis was found in the longest period, from PRE to POST3 (p = .03, η2 = 0.003).
All Assessments
In the group of residents who had all four assessments (PRE, POST1, POST2, POST3), the change in the mean outcome scores over time in the two groups is visualized in Figures 2g, 3g, and 5g. The trends observed were consistent with the results reported at the separate assessment points (i.e., with residents surviving to each assessment point).
Discussion
We investigated change over time in functional outcomes in LTC home residents with history of COVID-19, at multiple follow-up points and over a longer follow-up period, expanding on the previous research on this topic. When studying consequences of COVID-19 in the population of LTC home residents, the unique characteristics of this population must be carefully considered. There is a high prevalence of morbidity, high frailty, and high mortality in LTC residents, and health deterioration over shorter periods of time is common. To provide a relevant real-life context for exploring outcomes in residents with a history of COVID-19, we included other residents residing within the same LTC homes, in the same period, but with no evidence of COVID-19. We found a slightly greater deterioration in ADLs in the COVID group than in the No-COVID group in the period following the positive COVID test, as well as a greater increase in clinical care needs. However, this trend did not persist, and no difference was found between the two groups in the subsequent assessments.
A deterioration over time in ADL performance was recorded in both COVID and No-COVID group of residents, consistent with previous research findings in Cortés Zamora et al. (2022) and Pérez-Rodríguez et al. (2021). Similarly, a slight deterioration in cognitive functioning was found in both groups, consistent with the findings in Greco et al. (2021). A deterioration over time in ADLs and cognitive functioning may be expected in the population of LTC residents, with various factors important for this trend, such as advanced age, multimorbidity, and greater susceptibility to infections and their adverse effects. Additionally, in the pandemic circumstances, many pandemic-related factors were likely to contribute to this trend, such as reduced mobility, social isolation, and interruption of the residents’ daily routines due to infection prevention and control measures (Levere et al., 2021).
We found a slightly greater deterioration in ADLs in the COVID group than in the No-COVID group in the first outcome assessment (i.e., from baseline to the first follow-up assessment), in line with other evidence about the negative effects of COVID-19 in the period following infection (Carnahan et al., 2021). The difference between the two groups was found in the first assessment only, and the change from baseline assessment to the following assessments was similar in the two groups. Similarly, there was a greater increase in the clinical care needs in the COVID group than in the No-COVID group from baseline assessment to the first outcome assessment only, suggesting that the increase in needs in the initial period after COVID-19 did not persist and that higher needs were likely related to the acute COVID-19 infection. Recovery toward baseline, after initial deterioration in functioning in the residents with COVID-19, was reported in van der Krogt et al. (2022). No difference in change in cognitive functioning from baseline to subsequent assessments was found between the two groups in our study, consistent with Greco et al. (2021).
One of the most severe effects of COVID-19 was the high post-COVID-19 mortality in LTC residents (Akhtar-Danesh et al., 2022)—high mortality in the COVID group in the first month following a positive COVID-19 test was revealed in this study. Mortality among the frailest residents in the short period after contracting COVID-19 may be related to the findings of greater deterioration in ADLs and increase in clinical care needs in the COVID group in the first follow-up assessment with no differences found in the following assessments (i.e., after the highest wave of mortality subsided and the frailest residents died). However, the same trend of an initial deterioration in the COVID group and no later differences between the groups was found in the subgroup of residents who lived the longest and had all four assessments, pointing to the process of recovery after the disease.
Limitations of the current study include group membership determination (COVID and No-COVID) based only on a positive COVID-19 test. Due to inconsistent testing procedures in the early phase of the pandemic and the limited accuracy of the tests (Dinnes et al., 2020), some residents in the No-COVID group could have been infected with the virus as well. Additionally, we did not have reliable information about the severity and course of the COVID-19 disease in residents in the COVID group or about pre-COVID-19 comorbidities, which would enable us to differentiate further and expand our analysis and results. Information was not available about re-infections and about COVID-19 vaccination uptake—these important variables need to be examined in future research, as well as other relevant moderators, including pandemic phase, virus modality, and changes in care during the pandemic. Finally, it is important to note that the research question addressed in the current study tapped into overall differences in selected functional outcomes in residents with and without history of COVID-19, in available time intervals (quarterly assessments). More granular investigation was conducted about the very important topic of pandemic mortality in LTC, as well as about individual outcome trajectories among COVID-19 survivors (e.g., the Long COVID conditions; Fyffe et al., 2023; Sorensen et al., 2022). These two topics required different research designs and analytical approaches, and the results are reported and discussed in separate reports.
Conclusion
The current study provides more details to the picture of the COVID-19 pandemic in LTC homes. The results convey both the severity of COVID-19 effects in LTC home residents and hope for recovery, informing relevant clinical and care practices in LTC. Mortality was substantially increased in the period following the infection among residents with a history of COVID-19. A slightly greater deterioration in ADLs and a greater increase in clinical care needs in the COVID group than in the No-COVID group in the period following the positive COVID test did not persist, and no difference was found between the groups in the subsequent assessments. Such findings bring hope for full recovery in survivors of COVID-19. Improving outcomes in the acute phase and survivorship in the first month after infection is a continuing concern in LTC residents with COVID-19.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214241245551 – Supplemental material for Exploring Post-COVID-19 Functional Outcomes in Residents in Long-Term Care Homes in British Columbia, Canada
Supplemental material, sj-docx-1-ggm-10.1177_23337214241245551 for Exploring Post-COVID-19 Functional Outcomes in Residents in Long-Term Care Homes in British Columbia, Canada by Gordana Rajlic, Janice M. Sorensen and Akber Mithani in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
We would like to thank the Fraser Health Authority (FHA) for facilitating this study. The views and conclusions expressed in this paper do not necessarily reflect those of the FHA. We would like to express our appreciation to Dr. Ronald Kelly for his valuable help with MDS RAI 2.0 data and Simran Dhadda for her editing assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is in part funded by COVID-19 Pandemic Response and Impact Grant (Co-RIG) Program of the Foundation for Advancing Family Medicine and the Canadian Medical Association Foundation, Grant/Award Number: FAFM-2021-0094-EN_Mithani.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.