
Abstract
Mindful self-care is a valuable activity that contributes to old people’s independence and self-control and its development is in line with the duties of social workers. This study aimed to validate the mindful self-care scale (MSCS) for Iranian old people and was performed on old people living in the community of Shiraz, Iran. This cross-sectional study was conducted on old people living in the community who met the inclusion criteria in Shiraz, Iran. After linguistic validation of the Persian version of MSCS with 36 items, face, and content validity were determined. Then the first part of construct validity was conducted using a kurtosis test, and exploratory factor analysis with the first sample (n = 250). After selecting the appropriate items, confirmatory factor analysis was assessed with the second sample (n = 250). Scale reliability was also evaluated. The optimal cut-off points were obtained by calculating the area under the curve (AUC). SPSS version 23 was used for further data analysis, while confirmatory factor analysis was conducted using AMOS version 24. Exploratory factor analysis loaded only 24 items with four factors. The modified second-order confirmatory factor analysis model displayed a good fit (RMSEA = 0.04; CFI = 0.90; GFI = 0.90). Cronbach’s alpha coefficient of MSCS with 24 items was .94. The cut-off points were 38, 11, 23, and 17 for factors of resilience, goal achievement, supportive relationship, and self-care respectively, and 90 for the whole instrument. The study found that the MSCS short form with 24 items is valid and reliable in the Iranian elderly population, making it an effective tool for mental self-care screening and a practical tool for social workers. However, the study recommends repeating the study in other cities of Iran to generalize the findings.
Introduction
The old population worldwide is growing rapidly due to various factors such as improving health conditions, improving medical care, reducing mortality, and this population has increased from 200 million in 1950 to 600 million in 2012, and this figure will reach 2 billion by 2050 (Bourne & Eldermire-Shearer, 2018). The aging population in Iran is also rapidly increasing, with the percentage of the population aged 65 and above projected to increase from 8.65% in 2016 to 10.5% in 2025 and 21.7% in 2050 (Manoochehry & Rasouli, 2017). The findings of a study indicate that 58% of older adults over the age of 65 need help to perform their daily activities and they have a lower quality of life (QOL) (Fassino et al., 2002). In the context of Iran, the quality of life in older adults is relatively poor, with only 7% of the elderly population reporting high QOL, 42% reporting low QOL, and 50% reporting moderate QOL (Poursadeqiyan et al., 2021). Older adults in Iran face challenges in adapting to changing family roles, and relationships, and decreasing financial resources (Noroozian, 2012).
To address these limitations and promote successful aging, self-care is highlighted as a valuable activity that can help older adults achieve individual independence, cope with aging issues, and ultimately enhance their quality of life (Allen et al., 2012). However, the reduction of self-belief to accept responsibility and self-confidence, which is reinforced by the negative stereotypes of social environments regarding aging, challenges and hinders the promotion of self-care practices. Therefore, it seems that measuring self-care ability with a mindful perspective and developing interventions based on this approach can help social workers in promoting self-care behaviors.
Mindful self-care is well-defined as a recurring process that includes mindful awareness and evaluation of intrinsic needs and external demands as well as purposeful commitment to specific measures to meet the needs and demands to attain wellness and personal effectiveness (Cook-Cottone, 2015). Mindful self-care is more than the traditional concept of self-care and has origins in Mindfulness-Based Stress Reduction (MBSR) and Dialectic Behavioral Therapy (DBT) (Christopher & Maris, 2010; McCusker et al., 2016). In fact, mindfulness self-care is a set of behaviors performed to have a desirable harmony with the self and others and support positive visualization (Cook-Cottone, 2015; Piran, 2015; Piran & Teall, 2012). Depending on the literature, there are many potential components to mindful self-care: mindful awareness, conscious relaxation, nutrition, hydration, exercise, self-relaxation, relief, self-compassion, social support, and spirituality (Cook-Cottone, 2015; McCusker et al., 2016; Norcross & Guy, 2007; Riegel et al., 2012).
Evidence shows that self-care behaviors are not appropriate in older adults (Zandinava et al., 2017). Cognitive and functional problems, multiple comorbidities, reduced social interactions, and low levels of self-efficacy in older adults lead to reduced self-care capacity (Dong & Simon, 2010; Naik et al., 2008; Sung & Kim, 2008). In addition, depletion of social support networks and loss of positive experiences affect mindfulness self-care and may create feelings of detachment, burnout, conflict, or self-harm, impaired body image, and substance abuse in older adults (Cook-Cottone, 2015; Hays et al., 1998; Woertman & van Den Brink, 2012). To solve the problems caused by the aging process and plan for successful aging, social workers have to know the mindful self-care circumstances of older adults (Eaton et al., 2024). For a deeper understanding of self-care, a tool is needed to measure it based on mindfulness. This tool can help social workers as experts in mindfulness and cognitive training who are at the forefront of psychosocial support and care for older adults (Wong et al., 2018).
Most of the research on mindful self-care has been conducted with the Mindful Self-Care Scale (MSCS) (Cook-Cottone & Guyker, 2018) which specifically identifies and classifies mindful self-care within clinical and non-clinical samples (Feng et al., 2019; Sünbül et al., 2018; Webb et al., 2019). This questionnaire is developed by Cook-Cottone and Guyker (2018), and conceptually six self-care domains of MSCS fit with Maslow’s (1968) theory: physical care and mindful relaxation (physiological needs), supportive structure (safety needs), supportive relationships (belonging needs), mindful awareness (cognitive needs), and self-compassion and purpose (esteem and self-actualization needs) (Cook-Cottone & Guyker, 2018; Hotchkiss & Cook-Cottone, 2019; Maslow, 1968). According to our searches, the MSCS, other than the original language, was translated and validated only in Turkish university students (Aydin-Sunbul et al., 2018).
Therefore, it seems that the existence of a validated version of this tool in the Persian language can be useful in the development of research in the Persian-speaking population of the world (including Iran, Afghanistan, Tajikistan, etc.), international comparative research, and for use by social workers. However, translating and validating the MSCS for the Iranian population involves several challenges, including linguistic and cultural differences. The Persian language and Iranian cultural context may affect the accuracy and relevance of the scale’s items, requiring careful consideration and adaptation. The validation process must also account for the unique characteristics of the Iranian elderly population, such as their cultural beliefs and values, to ensure the scale’s validity and reliability in this context.
In addition, it is noteworthy that the validation of the Persian version of the Mindful Self-Care Scale (MSCS) among the Iranian old population is essential due to the growing recognition of mindful self-care practices in promoting well-being among older adults. The lack of validated measures in Persian for assessing mindful self-care poses a significant gap in the field, hindering accurate assessment and tailored interventions for Iranian older adults. This study aims to fill this gap by providing a culturally adapted and validated tool, addressing linguistic and cultural nuances specific to the Persian language and Iranian cultural context. Therefore, this study aimed to determine the validity, reliability, and cut-off points of the Persian version of the 36-item Mindful Self-Care Scale (MSCS) (Cook-Cottone & Guyker, 2018) among the Iranian old population.
Materials and Methods
Measures
The Mindful Self-Care Scale (MSCS) was designed in 2018 to measure conscious self-care behavior. This self-report scale included six subscales and 36 questions, eight of which were related to the physical care subscale. The subscales of mindful relaxation, self-compassion, supportive relationships, supportive structure, and mindful awareness, included 6, 6, 5, 4, and 4 items respectively. This scale had three general questions as well. Response scores are based on the frequency of behavior in the past week (7 days): 1 never (0 day), 2 rarely (1 day), 3 sometimes (2–3 days), 4 often (4–5 days), 5 regularly (6–7 days) and one of the physical care questions (engaging in sedentary activities) should be reversed (Cook-Cottone & Guyker, 2018).
Translation and Cultural Adaptation
To ensure the accuracy and cultural relevance of the Mindful Self-Care Scale (MSCS) for the Iranian context, a rigorous forward-backward translation process was conducted. Two independent translators performed the English-to-Farsi translation, while two other translators conducted the Farsi-to-English back translation. Discrepancies between the forward and backward translations were meticulously resolved through discussion and revision, with valuable input from a panel of experts. Cultural adaptations were carefully implemented to enhance the scale’s relevance to the Iranian context, including modifications to certain words and images to ensure they were culturally appropriate and easily understandable for Iranian older adults. This thorough translation and cultural adaptation process aimed to create a version of the MSCS that accurately reflects the nuances of the Iranian culture and language, facilitating its effective use in assessing mindful self-care practices among Iranian older adults.
For face validity and to determine the completion time, the questionnaire was filled out by 10 old people to assess in terms of the concept and structure of the Persian language. After that, based on the opinions of the research team, the questionnaire was modified suitably and the final version was found.
Participants
This was a cross-sectional study conducted on two samples (phase 1, n = 250; phase 2, n = 250) of old people living in the community in Shiraz city during April and May 2020. In this study, two healthcare centers out of a total of 16 centers and 1 day center out of three options in Shiraz City were randomly selected. Older adults meeting inclusion criteria at the healthcare centers and day centers were identified through their records and chosen using a random number list. They were then asked to attend these centers on specific days to voluntarily take part in completing a questionnaire after being briefed on the study’s objectives and providing informed consent. Additionally, among the six parks where the elderly gather, one park was randomly selected. Elderly people who enter this park on weekends between 8 and 10 am were included in the study if they declared their desire and eligibility. Older people were included in the study if they met any of the following criteria: 60 years of age or older, having at least elementary education and not having persistent and serious psychological and physical problems. The exclusion criteria were unanswered questions in more than 30% of the questionnaire, and unwillingness to participate in the study.
Content Validity
To calculate the qualitative content validity, 10 experts in the field of health psychology who were familiar with the psychometric process were asked to provide their views on the accuracy of the item content in written form. They also checked the item position, grammar, and the use of appropriate words in phrases. Furthermore, in quantitative content validity collected from a panel of 10 experts, we examined the item importance and accuracy, using a three-point rating scale and the content validity ratio (CVR); also, we evaluated the design of the items, including relevance, clarity, and simplicity, by content validity index (CVI). The CVR and CVI scores for the MSCS were 0.85 and 0.91, respectively.
Content validity was done to ensure that the tool measures the desired attribute and that the questions cover the entire content of the tool (DeVon et al., 2007). To determine the content validity ratio, 10 experts (health promotion, gerontology, psychology, and nursing) were asked to evaluate the necessity of each item using a three-point rating scale (Almanasreh et al., 2019). To check the content validity index, experts expressed their opinions about the relevance, clarity, and simplicity of each item. After receiving the opinions of 10 experts, the content validity ratio and content validity index were calculated. According to Lawshe’s table, the minimum content validity ratio based on the evaluation of 10 experts was more than 0.62 (Lawshe, 1975). Based on the calculations, all the questions got an acceptable score and were retained and CVR and CVI scores were 0.85 and 0.91, respectively.
Construct Validity
After collecting data from the first 250 participants, for construct validity, the kurtosis test was measured and normality was identified. The kurtosis test is a test for normality that is used to run descriptive statistics and should be within +1 to −1 range (Garson, 2012). Then, the factor structure of the MSCS was specified by exploratory factor analysis (EFA) using three methods including principal component analysis, generalized least squares, and maximum likelihood in both Varimax and Equamax rotations (SPSS version 23). After selecting the appropriate items, confirmatory factor analysis (CFA) was performed on 250 participants of the second sample using structural equation modeling with AMOS 24, and first and second-order confirmatory factor analysis models were drawn and fit indices were calculated.
ROC Analysis
The ROC curve was applied to assess the best cut-off point using SPSS version 23. The ROC calculation is applied in psychometric studies to complement EFA & CFA (Hoo et al., 2017).
Reliability
Cronbach’s alpha coefficient was used to calculate the reliability coefficient and internal consistency.
Results
Characteristics of the Participants
The demographic data of the participants in the first sample indicated that most of the participants (n = 225; 90%) were in the age range of 60 to 70 years with a mean of 68.4 ± 3.7 years. The majority of participants were females (n = 175; 62.3%). Eighty-six percent (n = 215) of them were married, 3.2% (n = 8) single, and 10.8% (n = 27) widow. The majority of the participants, (n = 242) lived with their families. Forty-two percent (n = 105) of them did not have any diseases and the rest of them had diabetes (n = 68; 27.2%), hypertension (n = 45; 18%), depression (n = 6; 2.4%), and other diseases (n = 26; 10.4%). Most participants had lower education than diplomas (n = 145; 58%), and the rest had diplomas (n = 54; 21.6%), bachelor of degrees (n = 45; 18%), and master’s degrees (n = 6; 2.4%). Characteristics of most participants in the second sample included 60 to 70 years old (n = 203; 81.2%); female (n = 151; 60.4%); married (n = 209; 83.6%); living with family (n = 234; 93.6%); with diabetes (n = 66; 26.4%) and HTN (n = 50; 20%); lower education than diploma (n = 132; 52.8%).
Construct Validity
In the first sample, the Kurtosis values of questions 11 and 14 were 8.18 and 13.43, respectively, so these questions were deleted. A normality test was performed and considering Boxplot, 5 outlier participants were excluded from the analysis (with numbers: 49, 51, 68, 86, 88).
Results of Exploratory Factor Analysis
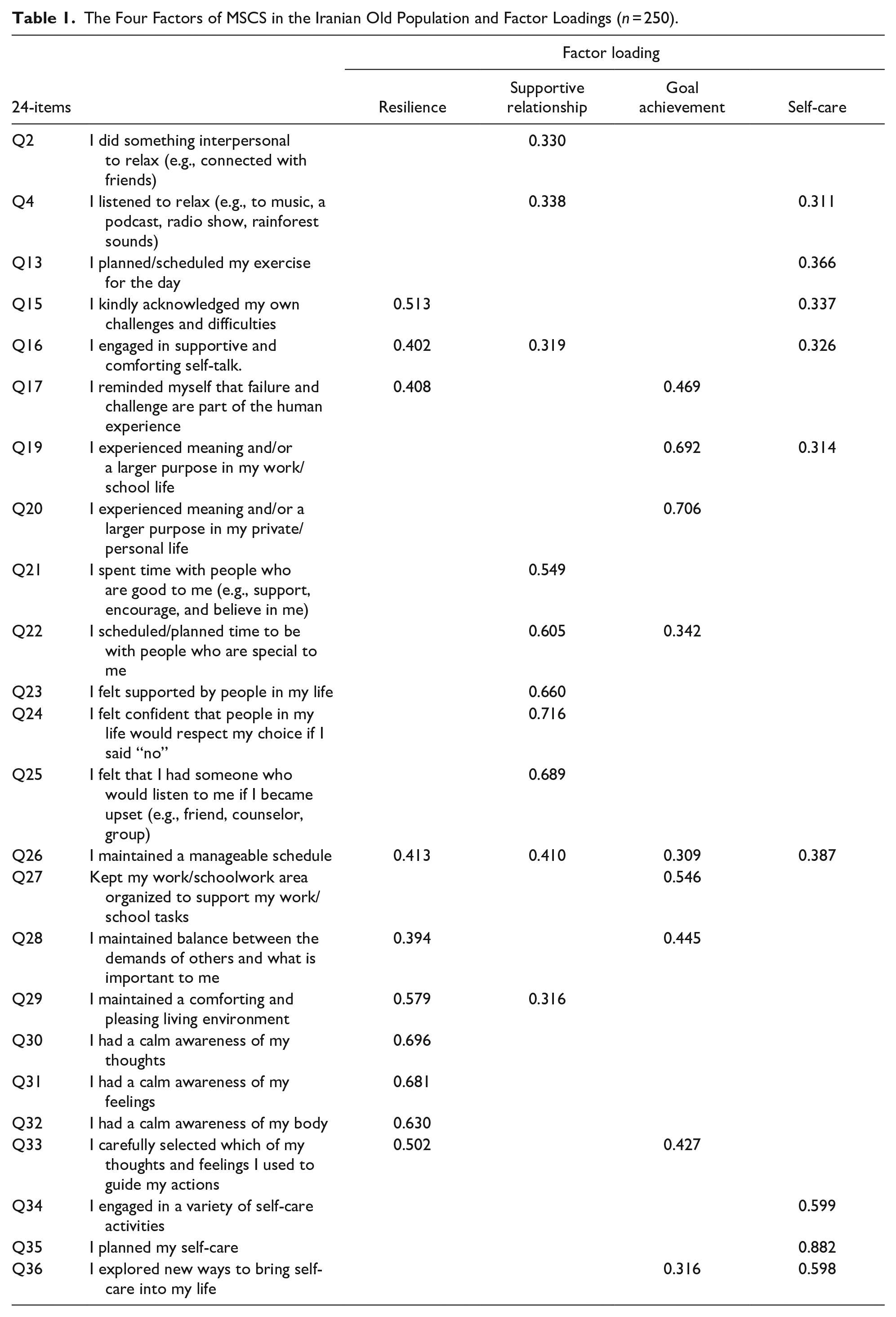
The results of Bartlett’s test of sphericity (χ2 = 4135.796; p < .001) and Kaiser-Meyer-Olkin test (KMO = 0.897) indicated that data were appropriate for factor analysis. Therefore, exploratory factor analysis (EFA) was conducted on the 34-item questionnaire with 245 participants utilizing three methods of principal component analysis, Generalized Least Squares, maximum likelihood, and each in two rotations (varimax and Equamax). Six models were obtained that Maximum likelihood with Equamax rotation was a theoretically and statistically better model. Here, 10 items (1-3-5-6-7-8-9-10-12-18) of the MSCS questionnaire were deleted due to absolute value <0.3. After that four factors were extracted (24 items) and named resilience (10 items), supportive relationship (six items), goal achievement (three items), and self-care (five items) (see Table 1).
The Four Factors of MSCS in the Iranian Old Population and Factor Loadings (n = 250).
Results of Confirmatory Factor Analysis
After selecting the appropriate items, the result of EFA was verified by conducting confirmatory factor analysis (CFA) and using structural equation modeling. The first- and second-order confirmatory factor analysis models were modified by AMOS correction commands. Table 2 shows suitable fit indices of modified the first-and second-order model compared with default models. Figure 1 displays the structural modeling of modified first- and second-order CFA models.
Fit Indices of the Confirmatory Factor Analysis (CFA) of MSCS Among Older Adults.


Modified first-order and second-order model.
Reliability Analysis
The reliability of 36-item MSCS and our final 24-item scale was estimated 0.92 and 0.94, respectively, via Cronbach’s alpha in the older adults. The Cronbach’s alpha coefficients of four subscales: resilience, supportive relationship, goal achievement, and self-care were .91, .84, .79, and .79, respectively.
Results of ROC Analysis and Determination of Cut-Off Points
After exploratory and confirmatory factor analysis, the cut-off points of Receiver Operating Characteristics (ROC) analysis were used. According to Table 3, using the ROC Curve distribution for 24-MSCS, we used mean scores (Montazeri et al., 2003) as a cut-off threshold of mindful self-care questionnaire. The cut-off points were 38, 11, 23, and 17 for the resilience, goal achievement, supportive relationship, and self-care subscales, respectively, and 90 for the whole instrument. D-Value coefficient is known to determine the appropriate cut-off point and less than 0.2 indicates the favorable cut-off score.
AUC, Sensitivity, Specificity, and D Value for Possible Cut-Off Points of 24-Item MSCS and Subscales.

Source. (John & Benet-Martínez, 2014; Kallner, 2018)
Note. AUC = area under curve; CI = confidence interval; DIFF = abs (sensitivity – specificity); D Value or K-Index = Sqrt ((1 − Sensitivity)² + (1 − Specificity)²).
Two-sided Chi-squared test, p ≤ .05.
Discussion
The present study aimed to translate the Mindful Self-Care Scale (MSCS) into Persian and assess its validity and reliability to be used in different studies on the old population to serve as a suitable tool for Farsi-speaking researchers and social workers. We applied exact methods according to psychometric and conceptual criteria. The final MSCS was shorter than the original one with improved fit indices in the older adults. The number of short version sub-scales for the older adults was also fewer than the original one and included four subscales: resilience, goal achievement, supportive relationship, and self-care. Based on the results 12 items were removed in different analyzes. Now, we introduced a shorter version of MSCS for the old population that includes four subscales with 24 items.
According to the findings, out of six items related to relaxation, four were removed during different analyses (options 1, 3, 5, and 6). It seems that the reason for these omissions is that the examples of relaxation in the traditional and religious society of Iran are different from modern Western society. Examples such as writing, painting, playing instruments, and singing are part of the modernity of Western societies, and examples of relaxation for older adults in Iran include attending religious ceremonies, attending mosques, reciting the Qur’an, and attending the cemetery, examples of which are not available in any of the items. The illiteracy of the old participants (58%), lack of access to books, and the absence of reading habits can also be the reasons for not reading books among the participants. The sound of music, radio programs, or rain is also a tangible example of relaxation that is understood in different cultures, so they have not been eliminated. Of course, an omission of the above options is not an absolute deletion, but it is suggested that this questionnaire should be modified, and examples of calming the Iranian society should be included in the items. The authors of this study suggest four alternative items for relaxation in line with Iranian culture, including “I did something intellectual (using my mind) to help me relax (e.g., read the noble Quran),” “I did something creative to relax (e.g., calligraphy, gardening, cooking, repairing home appliances),” “I sought out images to relax (e.g., old movies, old photo album, sea, and sky),” “I sought out smells to relax (rain, grass, flower, soil, smells of thatch).” In the continuation of this subject, it should be said that since social workers support people transitioning to aging and its challenges through a combination of practical and emotional support, anxiety management, and relaxation training (Wamara & Naumiuk, 2023), the presence of relaxation items in the questionnaire can help to measure the condition of the old people.
There were four items about doing exercise among the deleted items (10, 11, 12, 14): “I exercised at least 30 to 60 minutes”; “I took part in sports, dance or other scheduled physical activities (e.g., sports teams, dance classes)”; “I did sedentary activities instead of exercising (e.g., watched TV, worked on the computer)”; and “I practiced yoga or another mind/body practice (e.g., Tae Kwon Do, Tai Chi).” The possible explanation is that some Iranian old people faced different barriers to exercise including individual barriers such as lack of exercise habits, physical problems, laziness, and environmental barriers such as lack of an elder-friendly environment for exercise and not having enough money to enroll in sports classes. Some studies have also confirmed that most Iranian older adults do not engage in regular physical activity and it is estimated that 68% of Iranians over the age of 60 do not take part in any physical activity during the week (Motefaker et al., 2007; Nadri et al., 2016; Salehi et al., 2010). Another reason could be that in traditional Iranian society, older adults, especially women, are looked at as wise, calm, and inactive people. Of course, it is noteworthy that yoga and tai chi are not common sports in Iran. In our opinion, the only common physical activity among Iranian seniors is walking with friends in local parks, which unfortunately is not common among older women. This finding shows the insignificance of exercise among Iranian older adults, and that geriatric social workers can bring social vitality to Iranian older adults by providing training and providing the conditions for exercising.
Based on the results, three items about older adults’ nutrition (7, 8, 9) were also removed. A logical explanation could be that snacks have a wide range in Iranian culture, so it is better to provide examples of various types of snacks such as nuts, raisins, and figs and also seems necessary to give examples of protein, fruits, and vegetables to the older adults to make the items more tangible and understandable. Our suggested alternative items are as follows: “I drank at least 6 to 8 cups of water or other beverages such as milk, fruit juice, herbal tea, and herbal distillates,” “I ate a variety of nutritious foods (e.g., meat, poultry, fish, eggs, spinach, cabbage, and other vegetables, fruits, pistachios, raisins, and figs),” and “I planned my breakfast, lunch, evening meal and dinner.”
In general, items were removed for several reasons, including cultural differences in relaxation methods, low literacy rates among the elderly in Iran, and difficulties in understanding some items related to nutrition. Similarly, a study aimed at the psychometric properties of the Persian version of the music model considers it inevitable to remove certain items to improve the reliability and validity of the scale for use in the Iranian context and the Persian language (Farahani & Saeedi, 2022). Therefore, it seems that removing the items was necessary to ensure the accuracy and appropriateness of the scale for use in the Persian language and culture. Although the removal of items from the scale can affect the construct validity and overall reliability, the main concepts were preserved to some extent in this questionnaire, that is, the general items related to relaxation and exercise remained in this questionnaire and only the samples were removed. Nevertheless, it seems that this study should have been done to identify the existing gaps, and in the next investigations, items corresponding to Iranian culture can be added to the questionnaire by obtaining permission from the original developer of the questionnaire.
According to the findings, one of the components of this questionnaire is supportive relationships, which is in line with social work duties, such as examining the ability of older adults to attract social support, as well as examining their social environment and then providing assistance and supporting for the development of supportive relationships (Gehlert & Browne, 2011). In addition, another component of the questionnaire is resilience. Several physical, emotional, and social issues, including poverty, social isolation, and deterioration of health and daily functioning are challenges of old age, and research shows that factors such as social support, spirituality, and hope contribute to the resilience of old people (Polson et al., 2018). Social workers can increase the resilience and hope of the elderly by assessing the resilience of the elderly and applying strategies to promote successful aging (Gallardo-Peralta et al., 2022).
We did a thorough search to find the cut-off points of the original questionnaire and its subscales, but we did not find anything, so we used mean scores as a cut-off threshold of the mindful self-care questionnaire in the Iranian old population. It is indicated that the mean MSCS-24 score for the old population of respondents provides a rough guide to the best cut-off threshold. Therefore, as to the people who scored above the mean, the results indicated that 55.6% of the respondents had good mindful self-care. This indicates that if researchers wish to use a screening instrument for mindful self-care in the old population, MSCS-24 is remarkably robust and useful.
Recommendations for Future Research
Future research on mindfulness self-care in the elderly should focus on expanding its application to different populations and cities, investigating its relationship with health outcomes, and examining the impact of mindfulness-based interventions on the physical and emotional well-being of the elderly. This is particularly important in the context of the aging population in Iran, where self-care ability is a crucial factor in improving the quality of life for older adults. Additionally, it is suggested that the items removed from the Mindful Self-Care Questionnaire (MSCS) should be modified based on the Iranian elderly culture and a study should be conducted to re-estimate the validity and reliability of the questionnaire.
Clinical Implications for Health Managers and Policymakers
Validation of the Mindful Self-Care Questionnaire in the Iranian elderly context has significant clinical implications for health managers and policymakers. This questionnaire, with acceptable psychometric properties and a good factor structure, is a valuable tool for measuring mindful self-care in older adults in Iran. It enables healthcare professionals and social workers to identify areas where support is needed for older adults to practice mindful self-care, leading to improved health outcomes and quality of life. By measuring mindful self-care, tailored interventions can be developed to address the unique needs of older adults in Iran, helping policymakers identify gaps in healthcare services that may hinder mindful self-care practices.
Conclusion
The short version of MSCS for older adults with 24 items illustrated acceptable psychometric properties and a good factor structure to measure mindful self-care in old people in the Iranian context. One of the limitations of this study was that, out of respect for the original developer of the questionnaire, we could not make the necessary cultural changes to its items and had no choice but to delete items. Additionally, the study was conducted only in Shiraz, Iran, which may limit the generalizability of the findings to other regions or elderly populations within Iran. To ensure the scale’s applicability across different contexts, it would be beneficial to repeat the study in other cities of Iran.
Footnotes
Acknowledgements
We are grateful to dear seniors who participated in the study that without their support the study could not have been conducted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was scientifically approved and financially supported by the Vice-chancellor of research at Shiraz University of Medical Sciences, Shiraz, Iran.
Ethical Approval
This study was approved by Shiraz Medical Sciences University’s ethics committee No: IR.SUMS.REC.1398.1365.