
Abstract
Introduction
The number of patients with diabetes continues to rise and is expected to reach approximately 400 million (Khan et al., 2020). The prevalence of diabetes in Japan is 3%–8% (Uehara et al., 2014). The number of older adult patients with diabetes has been increasing owing to the aging of the population (Danaei et al., 2011). Older adults with diabetes have less frequent interaction with others, have more complications and comorbidities, and use more drugs than those without diabetes (Ida & Murata, 2022a; Sinclair et al., 2015). Those with large glycemic fluctuations or who use insulin have less frequent interaction with others (Ida et al., 2020). Diabetic complications decrease social roles (Ida et al., 2021). In them, barriers to social participation may be huge (Ida & Murata, 2022b).
Social participation is not uniform, but it is regarded as “the person’s involvement in activities that provide interactions with others in a society or a community.” (Levasseur et al., 2010). Levasseur et al. proposed a taxonomy of social activities based on an individual’s levels of involvement with others and the goals of these activities (Levasseur et al., 2010). The taxonomy consists of 6 levels, with levels 3 to 6 (i.e., activities generating interaction with others) denoting social participation activities. Specific social participation activities include being involved in sports groups, hobby groups, learning activities, neighborhood associations, volunteer activities, and work and interaction with friends (Levasseur et al., 2010; Tomioka et al., 2017; Yokobayashi et al., 2017).
Previous studies have developed questionnaires to examine social participation in community-dwelling older adults (Kelders et al., 2012; van Brakel et al., 2006) or social activities in older adults requiring assistance (Hirano et al., 2020). In addition to evaluating the frequency of social participation, it is vital to facilitate social participation in older adults by identifying factors that hinder their social participation. Previous studies (Cabinet Office, 2021; Hand & Howrey, 2019; Naud et al., 2019, 2021; Strobl et al., 2016) have reported that barriers to social involvement include loss of friends, strength or health limitations, and busy schedules. As described above, a comprehensive evaluation of barriers to social participation is important, necessitating a tool to assess such barriers.
To the best of our knowledge, no tool exists to assess barriers to social participation in older adult patients with diabetes. We believed that developing such a tool would facilitate their social participation and enable them to find social participation activities suited to them. This study aimed to develop a questionnaire for evaluating the factors hindering social participation in older adults with diabetes and confirm its reliability and validity.
Methods
Patient Selection
This was a cross-sectional study involving patients with diabetes (types 1 and 2) who were undergoing outpatient treatment. This study included outpatients who received treatment for diabetes at xx, Ise City, Mie Prefecture. The ethics committee of the xx approved the study (Approval number: xx), and it was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent. The eligibility criteria for the study were individuals who were outpatients aged ≥60 years with diabetes and received treatment at our hospital between July 2022 and December 2022. The exclusion criteria were alcohol abuse, severe psychiatric disorders, or inability to cooperate with the study independently. In the planning stage of this study, we estimated that the questionnaire would consist of 10 to 30 questions. Given that 10 respondents were required for each question, we calculated that the required sample size was more than 300. The Kaiser–Meyer–Olkin Measure of Sampling Adequacy was 0.88, indicating that factor analysis was conducted with an adequate sample size (de Vet et al., 2005).
Definition of Social Participation
Based on previous studies (Levasseur et al., 2010; Tomioka et al., 2017; Yokobayashi et al., 2017), social participation was defined as “a person’s involvement in activities that allow interactions with others.” Social activity participants are those who engaged at least once a month in (1) work, (2) volunteer activities, (3) hobby or social clubs, (4) learning activities, (5) sports or exercise activities, (6) quality time with friends or neighbors, (7) neighborhood associations, and (8) activities to share special skills and experiences.
Preparation of the Draft Social Participation Barriers in Patients With Diabetes (SPBD)
The literature was searched on Medline, Web of Science, CINAHL, CiNii, and the Japan Medical Abstracts Society databases to examine the factors hindering social participation on July 1, 2022. An example of a search strategy is provided below. The search terms used are: (“social participation” [MeSH Terms] OR “social participation” [All Fields] OR “social capital” [MeSH Terms] OR “social capital” [All Fields] OR “social networking” [MeSH Terms] OR “social network*” [All Fields] OR “social* engage*” [All Fields] OR “social* activ*” [All Fields] OR “social* disconnect*” [All Fields] OR “social relation*” [All Fields OR “social* integrat*” [All Fields OR “social tie*” [All Fields OR “social contact*” [All Fields] OR “social* connect*” [All Fields] OR “social alienation” [All Fields] OR “leisure activ*” [All Fields] OR “recreational” [All Fields] OR “volunteer activ*” [All Fields] OR “social* involvement*” [All Fields] OR “community participation” [All Fields] OR “community engage*” [All Fields] OR “community involvement*” [All Fields]) AND “elderly” [All Fields] OR “elder” [All Fields] OR “old age” [All Fields] OR “old people” [All Fields] OR “older” [All Fields] OR “aging” [MeSH Terms] OR “aging” [All Fields] OR “ageing” [All Fields]). The literature search extracted original research articles written in English or Japanese. References in the extracted articles were manually searched if needed.
Based on the extracted literature and discussion with physicians, nurses, and caseworkers, 20 draft questions were created. These questions included health, interaction with others, diabetic complications and treatment, and willingness for social participation. The SPBD questionnaire is self-administered, and the responses were given on a 4-point scale: “1. Strongly disagree,” “2. Disagree,” “3. Agree,” and “4. Strongly agree.” We confirmed the clarity of the questionnaire by collecting opinions from 10 patients with diabetes aged ≥60 years who were receiving outpatient treatment at our hospital. They were asked whether the questions were easy to understand (Yamazaki et al., 2021). As a result, in Question 1 “I think I am unable to participate if the information is limited,” some respondents reported that they did not understand what this information was about. Thus, Question 1 has been revised: “I think I cannot participate if the information on social activities is limited.” Regarding Question 8, “I think I am unable to participate if I have diabetic complications,” some reported that specific complications should be described. Thus, Question 8 has been revised as follows: “I think I am unable to participate if I have diabetic complications, such as numbness on the hands or feet, physical appearance, and kidney disease.” The development of the SPBD draft has been completed through the above process.
Relationship Between Questions and Social Participation
To determine whether each question of the SPBD questionnaire was associated with social participation, logistic regression analysis was conducted using social participation as the dependent variable and each question as the explanatory variable. The odds ratio of each question to social participation was calculated. Questions without a statistically significant association in the logistic regression analysis were excluded (Yamazaki et al., 2021).
Confirmation of Reliability and Validity
Cronbach’s alpha coefficient was calculated to evaluate internal consistency. The correlation between each item and the total score (I-T correlation) was calculated, and items with a correlation value <.3 were deleted as they indicated that the corresponding item did not correlate (Boateng et al., 2018). Exploratory factor analyses (principal axis factoring, varimax rotation, and promax rotation) were conducted to test construct validity and confirm the number of factors used in the questionnaire. Questions with factor loadings ≥0.4 were included in the questionnaire (Boateng et al., 2018; Field, 2013), whereas questions with a correlation coefficient ≥.7 were deleted (Boateng et al., 2018). Using the above process, the questions to be used in the questionnaire were determined, and the total score of the questionnaire was represented as an SPBD score. As criterion-related validity, Pearson’s correlation coefficient was calculated to determine the correlation among SPBD scores, frequency of social activities, homeboundness, physical frail scores, and social frail scores.
Variable Measurement
The following variables were evaluated: age, sex, body mass index (weight [kg]/height [m2]), smoking habits, drinking habits, classification of diabetes (type 1 or 2), duration of diabetes, hemoglobin A1c (HbA1c), hypertension, dyslipidemia, diabetic retinopathy, diabetic nephropathy, depression, diabetic nephropathy, cardiovascular disease, living alone, homeboundness, physical frailty, social frailty, and use of antidiabetic agents. Diabetes was classified into type 1, type 2, and others according to the diagnostic criteria (Araki et al., 2020). Hypertension was defined as systolic blood pressure ≥130 mmHg, diastolic blood pressure ≥80 mmHg, or intake of oral antihypertensive medication, whichever was met. For lipids, dyslipidemia was defined as either triglycerides ≥150 mg/dL, high-density lipoprotein-cholesterol <40 mg/dL, low-density lipoprotein-cholesterol (LDL-c) ≥120 mg/dL (LDL-c ≥ 100 mg/dL for patients with coronary artery disease), or intake of oral lipid-lowering drugs. Diabetic neuropathy was characterized by the presence of reduced Achilles tendon reflex, decreased vibration sensation on the lateral malleolus, or abnormal nerve conduction test result, whichever was met. The presence of cardiovascular disease was determined when the patient had either a current or a medical history of ischemic heart disease, such as angina pectoris or myocardial infarction, or cerebrovascular diseases, such as cerebral infarction. Homeboundness was evaluated using a self-administered questionnaire based on a previous study (Ida et al., 2020). Physical frailty was evaluated using a simple frail index developed by Yamada and Arai (Yamada & Arai, 2015). Social frailty was evaluated using a 5-item questionnaire developed by Makizako et al. (2015). The patients were instructed to answer Yes or No regarding smoking habit (Do you smoke?), alcohol habit (Do you drink?), and living alone (Do you live alone?). Furthermore, the use of diabetes drugs was confirmed by checking the patient interview form (if data was unavailable, medical records were used).
Statistical Analysis
Patient background factors and questionnaire score distribution were presented. The unpaired t-test was employed for continuous variables, and the chi-squared test for binary variables for group comparisons. The two-sided significance level was set at <.05. Statistical analyses were conducted using STATA version 16.0 (Stata Corporation LP, College Station, TX).
Results
Patient Background
A total of 353 patients (210 men and 143 women) who met the eligibility criteria were included in the analysis. The proportion of social participation was 75.6%, specifically (1) 36.5% for work; (2) 5.6% for volunteer activities; (3) 11.9% for hobby or social clubs; (4) 4.5% for learning activities; (5) 14.4%, sports, and exercise activities; (6) 41.3% for quality time with friends or neighbors; (7) 10.7% for neighborhood associations; and (8) 3.9% for activities to share special skills and experiences (Table 1).
Characteristics of the Analysis Population.
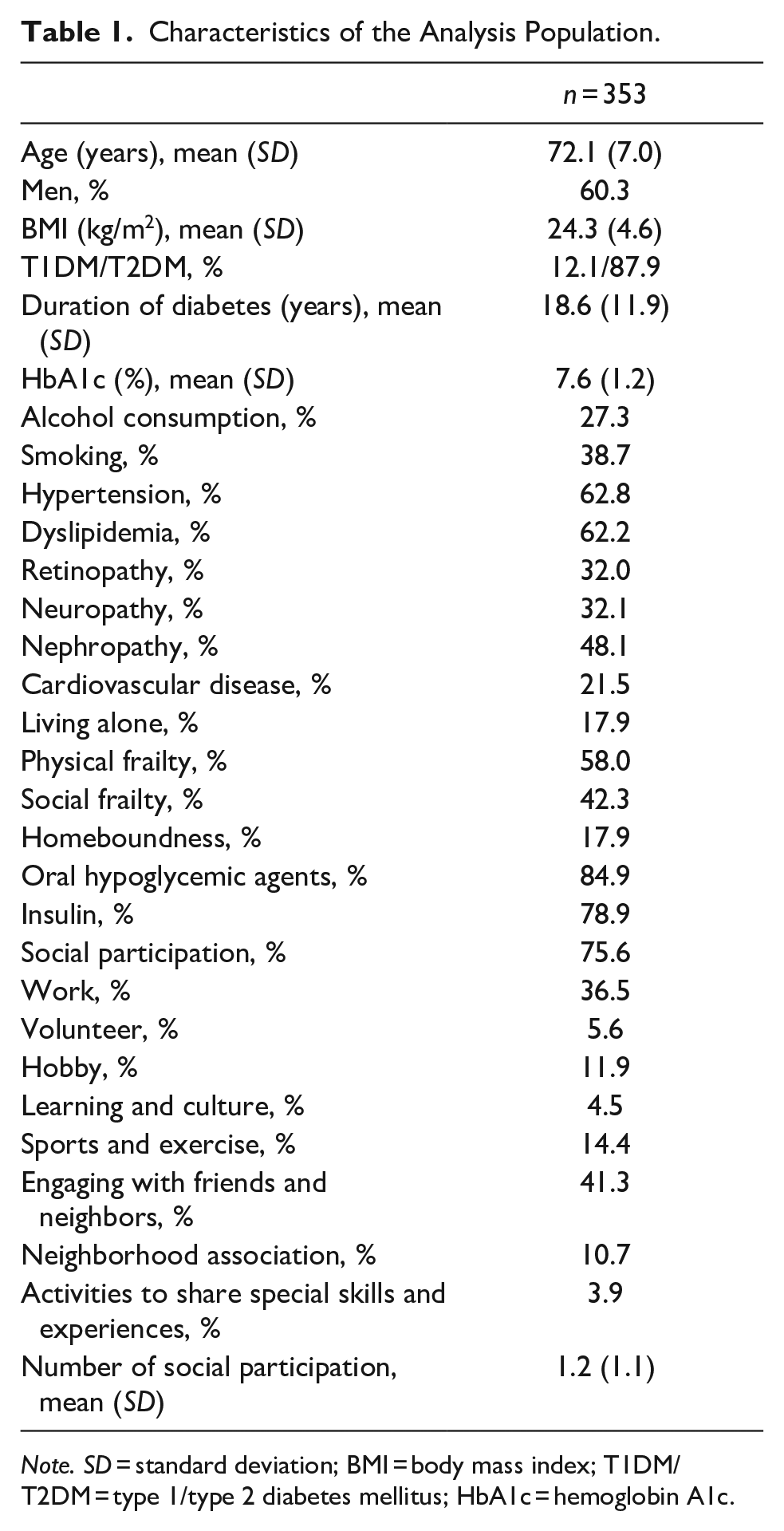
Note. SD = standard deviation; BMI = body mass index; T1DM/T2DM = type 1/type 2 diabetes mellitus; HbA1c = hemoglobin A1c.
The relationship between questions and social participation is demonstrated in Table 2. A significant association was not observed in questions 2, 3, 4, 6, 7, 15, and 16 in the logistic regression analysis, and these questions were deleted. The I-T correlation coefficient of the remaining 13 questions was ≥.3, and Cronbach’s alpha coefficient was .87. Principal axis factoring with nonrotation demonstrated that the eigenvalue decreased to 5.4, 1.2, and 0.8. The Kaiser–Meyer–Olkin Measure of Sampling Adequacy was 0.08, indicating that factor analysis was conducted with an adequate sample size.
Item Scores and Their Relationship to Social Participation.

Note. Items in bold are significantly associated with social participation barriers. SD = standard deviation.
Interpretable factors were not identified after varimax and promax rotations, and it was considered a single-factor structure. In terms of factor loadings, question 1 was low at 0.170; thus, it was deleted. Correlation coefficients between the remaining questions (questions 5, 8, 9, 10, 11, 12, 13, 14, 17, 18, 19, 20) were ≥.7 in questions 9, 10, 11, 12, 13, and 14. Considering factor loading and clinical significance, questions 10 and 11 were deleted. The total score of the remaining 10 questions was expressed as an SPBD score (23.2 ± 6.2). The SPBD score was significantly associated with the number of social activities (r = −.251, p < .001), frequency of going out (r = .164, p < .001), physical frailty (r = .330, p < .001), and social frailty (r = .329, p < .001). The adjusted odds ratio of the SPBD scores for social participation was 0.93 (95% confidence interval [0.88, 0.98]; p = .011) (Table 3).
Logistic regression with social participation as the outcome.

Note. CI = confidence interval; HbA1c = hemoglobin A1c; SPBD = Social Participation Barriers in Patients with Diabetes; *P < 0.05.
Discussion
In this study, we developed the SPBD questionnaire, a self-administered questionnaire used to evaluate factors hindering social participation in older adults with diabetes. The reliability and validity of the questionnaire were confirmed. To the best of our knowledge, the SPBD questionnaire is the first tool for assessing factors hindering social participation in older adults with diabetes.
Herein, we discuss the 10 questions in the SPBD questionnaire. The highest factor loading questions were associated with diabetes treatment (questions 12, 13, and 14), followed by those associated with diabetic complications and hyperglycemia (questions 8 and 9) and other questions (questions 5, 17, 18, 19, and 20). The results indicated that diabetes treatment was a huge barrier to social participation. Previous studies that included older adults with diabetes have demonstrated that a low frequency of going out is associated with insulin use (Ida et al., 2020), scarce interactions with others are associated with significant glycemic fluctuations (Ida et al., 2020), and social roles are associated with diabetic nephropathy (Ida et al., 2021). These results support the findings of the current study to some extent, although the definition of social participation differs between the previous studies and this study. Previous surveys indicated that busy schedules, limited interactions with neighbors, and interactions with groups without young generations are factors hindering their participation in community activities (Cabinet Office, 2021; Hand & Howrey, 2019; Naud et al., 2019; Strobl et al., 2016).
In this paragraph, we discussed the association of SPBD scores with the number of social activities, frequency of going out, physical frailty, and social frailty. The correlation coefficient between the SPBD score and the number of social activities, physical frailty, and social frailty was .25 to .3, but that between the SPBD score and frequency of going out seemed too small (.16). This result suggested that, as compared with a low frequency of going out, less social interactions and decreased physical function were factors strongly related to less social participation in older adults with diabetes. As the theory proposed by Levasseur (Levasseur et al., 2010), social activities are not just an outdoor activity, but an activity related to interaction with others and to physical and mental function, suggesting that SPBD scores may be associated with social interactions and physical function. In the present study, a multivariate analysis after adjusting several variables, including physical and social frailty, showed a negative association between SPBD scores and social participation. The SPBD questionnaire can comprehensively evaluate factors hindering social participation, such as treatment of diabetes, diabetic complications, and interaction with others. The present study showed that scores of the questionnaire were associated with a low frequency of social participation independent from other variables, including frailty, demonstrating the validity of the questionnaire.
Next, we discuss the frequency of social participation. The frequently reported social participation was engaging in quality time with friends or neighbors, work, and sports and exercise activities. Compared with previous studies that included (Kanamori et al., 2014; Tomioka et al., 2017; Yokobayashi et al., 2017), the proportion of engaging in quality time with friends or neighbors and work was similar between the present study and previous ones. However, the proportion of sports and exercise activities, hobbies, volunteer activities, and neighborhood associations was lower in this study than in previous studies. Two factors could explain this difference. First, people in poor physical condition are less likely to participate in hobby groups and volunteer activities (Cabinet Office, 2021; Naud et al., 2021; Strobl et al., 2016). This study included patients with diabetes, of whom many had complications and comorbidities. Second, women are more likely to participate in hobby groups and volunteer activities than men (Cabinet Office, 2021; Tomioka et al., 2017), and the proportion of men was higher in the present study. These two factors may result in less frequent participation in these two social activities.
Here, we discuss factors associated with SPBD scores, that is, engaging in quality time with friends or neighbors, volunteer activities, and hobbies. Hyperglycemia decreases interaction with friends (Yokobayashi et al., 2017). A possible explanation for this is that eating with friends leads to the intake of more calories (Yokobayashi et al., 2017). Regarding hobby and volunteer activities, as aforementioned, the presence of comorbidities, use of many drugs (polypharmacy), and hyperglycemia may be the leading causes of less frequent social participation (Klinedinst et al., 2022; Luster et al., 2022; Sinclair et al., 2015; Yokobayashi et al., 2017). The SPBD scores were not associated with sports and exercise activities or work. This could be explained by the fact that many patients in this study already had exercise habits, such as walking and resistance exercises, as part of their diabetes treatment. Thus, they were not hesitant to participate in sports and exercise activities. The SPBD scores were not associated with work; however, work was frequently reported as social participation. Although it is mere speculation, they may work for a living. Further evaluation will be required to investigate the relationship between SPBD scores and each social participation activity.
Cronbach’s alpha values ≥.7 usually indicate an acceptable level of reliability (Boateng et al., 2018). In this study, Cronbach’s alpha of SPBD was .873, indicating that this questionnaire was reliable. Furthermore, SPBD scores were significantly associated with physical and social frailties. Physical and social frailties are associated with less frequent participation in community activities in community-dwelling older adults (Bessa et al., 2018; Xie & Ma, 2021), indirectly suggesting that SPBD examines factors hindering social participation.
Next, we discuss the clinical significance of this study. Social participation is less frequent in patients with diabetes than in those without (Ida & Murata, 2022b). Examining factors that hinder social participation using SPBD may facilitate social participation in patients with diabetes. Among the SPBD questions, those with high factor loadings were those related to diabetes treatment. Multivariate analysis revealed that the actual use of oral hypoglycemic agents and insulin was not associated with social participation. The results indicated that older adults with diabetes might participate in social activities regardless of their treatment regimens (although they regarded diabetes treatment as a barrier to social participation). It is seemingly difficult to provide interventions for negative feelings possessed by patients with diabetes, corresponding to questions 17 and 20 (I am not a good talker [Q-17], I am not good at interacting with others [Q-20]); however, a previous study suggested that invitation from others to join social activities or the presence of friends may attenuate such negative feelings (Okamoto, 2008). Interventions for any of the SPBD questions may simultaneously remove several factors that hinder social participation in older adults with diabetes. The specific use of the SPBD questionnaire includes reduction of the intake of antidiabetic agents or the frequency of their use and glycemic fluctuations, along with the proposal of activities tailored to their personal values (e.g., proposing activities that allow them to interact with young people, or activities without requiring constant communication). Further studies will be needed to evaluate how the SPBD questionnaire can be used in practice.
This study had several limitations. First, the participants were outpatients at a clinic specializing in diabetes; therefore, the results of this study are applicable to patients with stable glucose levels or those with diabetes who are managed under the careful supervision of a family physician. Second, the sample size was relatively small. Third, no analysis was conducted on data on cognitive function or educational history, which may affect the results. Finally, this was a cross-sectional study, and thus, we could not predict the prognosis of patients with a high SPBD score (i.e., those with many factors hindering their social participation) and examine how their SPBD scores changed through interventions.
Conclusion
In the present study, we developed an SPBD questionnaire that assessed barriers to social participation in older adult patients with diabetes. The validity and reliability of the questionnaire were confirmed. We believe that the SPBD questionnaire can be used to assess barriers to social participation in older adults with diabetes.
Footnotes
Acknowledgements
The authors would like to thank the Department of Metabolic Diseases staff members at the Ise Red Cross Hospital for their cooperation in this study.
Author Contributions
SI designed the study and drafted the manuscript; KM worked on giving advice and reviewing the manuscript from a medical point of view, and KI and SM helped draft the manuscript. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The ethics committee of the Ise Red Cross Hospital approved the study (Approval number: ER2022-36), and it was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, SI, upon reasonable request.