
Abstract
As the incidence of dementia rises, increased utilization of surrogate decision-makers, including legal guardians, is anticipated. This manuscript presents an analysis of resident physicians’ experiences and perceptions regarding requirements, roles, and responsibilities of caring for older adults in need of, or already under, legal guardianship. This is a cross-sectional study, conducted at a tertiary academic medical center. A survey was sent, via Qualtrics, to all emergency medicine, family medicine, internal medicine, general surgery, and medicine-pediatric resident physicians. Eighty-eight out of three hundred thirty-three (26.4%) eligible residents physicians completed the survey. Most (98.9%) reported caring for patients under guardianship, yet many resident physicians reported significant uncertainty regarding the roles and responsibilities of guardianship, including its potential benefits and limitations. They also displayed misconceptions and overconfidence about guardians’ abilities to facilitate disposition, ensure financial security, and assign code status, among other matters. Our study highlights the importance of structured and directed education on the topic of guardianship for medical trainees.
Introduction
Cognitive deficits are correlated with impaired capacity (K. E. Zietlow et al., 2020). Within the United States, one-third of individuals 65 years and older had dementia or mild cognitive impairment (Manly et al., 2022). As the number of older Americans grow, so too will the proportion of those with dementia, and the percentage increases with age (2023 Alzheimer’s disease facts and figures, 2023). Patients who are deemed to lack decisional capacity due to cognitive impairment, and who do not have legally recognized powers of attorney or advance directives, may be appointed a legal guardian. Guardianship is an area of rising concern among those who care for older adults, as guardianship, due to its scope, infringes on traditional notions of autonomy and individual liberty. Additionally, several instances of guardian-perpetrated exploitation and abuse have emerged (Palmieri, 2021).
Despite these growing concerns, the medical community has yet to recognize guardianship and surrogate decision-making as educational priorities. Within the United States, we identified a psychiatry residency program that developed a workshop focused on care transitions, which included topics related to guardianship (Frank et al., 2020); and a geriatric fellowship program that piloted experiential training as an expert witness and included testifying in a mock guardianship trial (Foley et al., 2017). While these two workshops are promising, there is a concerning paucity of any published curricula specifically dedicated to the topics of guardianship and surrogate decision-making pertaining to older adults. Moreover, the Accreditation Council for Graduate Medical Education does not include these topics as required milestones for internal medicine (IM), family medicine (FM), general surgery (GS), medicine-pediatrics (MP), or emergency medicine (EM) residency programs, even though most of these trainees will care for wards under guardianship and may be asked to provide evidence in guardianship petitions or hearings.
In this manuscript, we share the results from our survey of resident physicians across multiple specialties. We asked resident physicians to report their experiences with patients requiring guardianship and their perceptions of the responsibilities, benefits, and limitations associated with guardianship. We aim to promote further understanding of current resident physician knowledge and perceptions to better inform future educational initiatives.
Methods
This is a cross-sectional assessment, conducted at a large tertiary academic medical center. An online program (“Qualtrics,” Provo, UT) was used to send a survey to all EM, FM, GS, IM, and MP resident physicians. The survey posed 12 direct questions about resident physicians’ experience with patients. Questions include agreeing or disagreeing with statements such as “I believe instruction on how to perform a decisional capacity assessment should be part of my residency training” as well as “In my understanding, patients who have intact decisional capacity must demonstrate which of the following,” and then selecting all that apply. Participation was voluntary and uncompensated. Data analysis was performed using Microsoft Excel (“Microsoft Excel” 2016). This study was reviewed and granted an educational exemption by our institution’s Institutional Review Board.
Results
Of 333 eligible resident physicians, 96 (28.8%) responded. Eight surveys were excluded due to incomplete response; thus, 88 surveys were included for analysis. Table 1 summarizes participants’ training programs and levels.
Distribution of Participating Resident Physicians by Training Year and Specialty.

Note. PGY = post-graduate year.
Did not specify their training program.
An overwhelming majority of resident physicians (98.9%) reported caring for patients under guardianship; only a single respondent reported no experience. Sixteen (18.2%) managed one to two patients, 30 (34.1%) managed three to five patients, and 41 (46.6%) managed more than five patients. Most resident physicians (96.6%) characterized themselves as “agreeing” or “strongly agreeing” that content on capacity evaluations and guardianship should be part of their training. Sixty-three (71.6%) resident physicians reported agreeing or strongly agreeing that they can recognize when an older adult needs guardianship, ten (11.4%) were unsure, and 15 (17.0%) disagreed or strongly disagreed.
In Table 2, we summarize resident physicians’ perceptions of the responsibilities and benefits of guardianship. In general, resident physicians showed a large degree of variance regarding their perceptions of the roles of guardians.
Residents Physicians’ Perceptions of the Benefits of Guardianship.
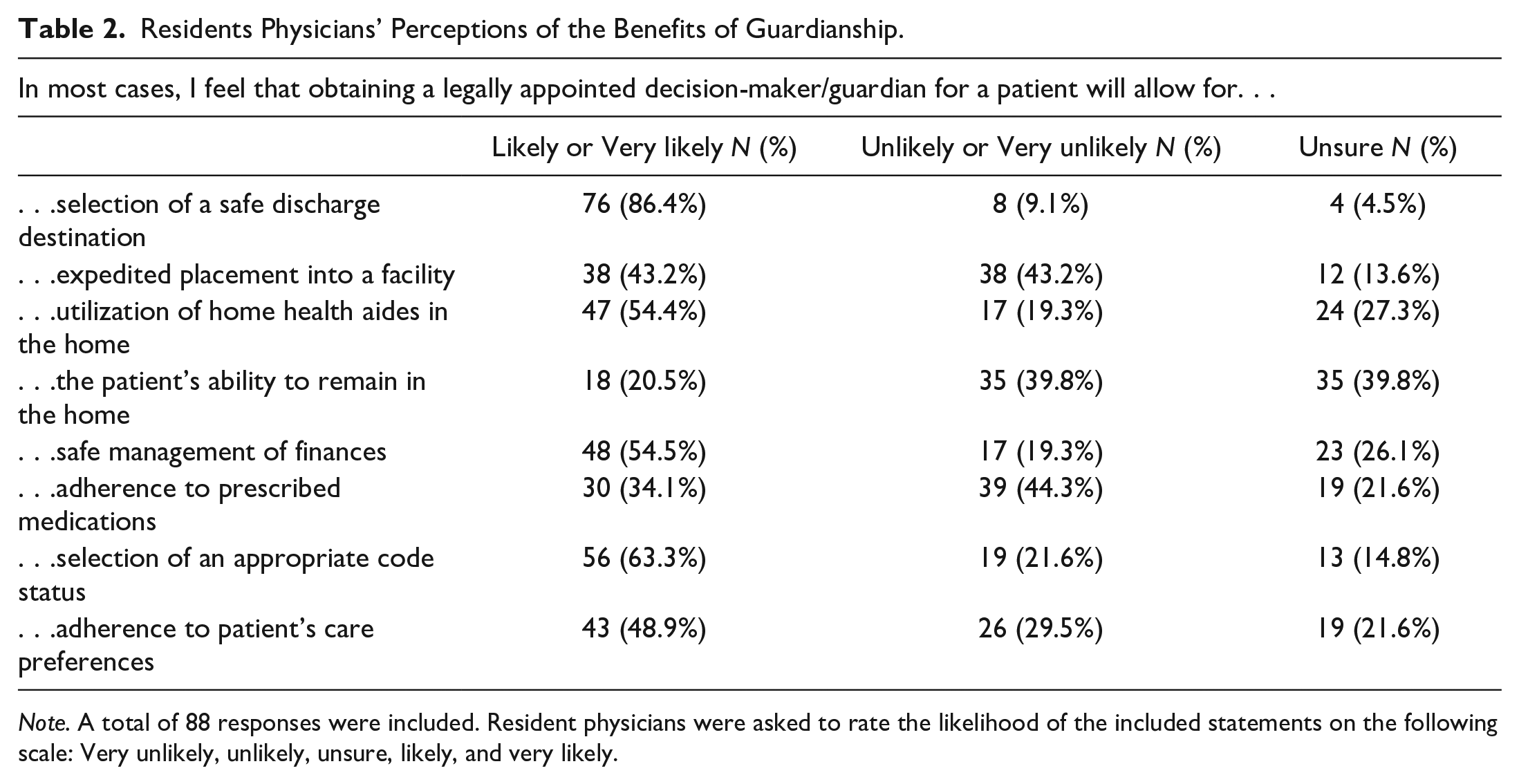
Note. A total of 88 responses were included. Resident physicians were asked to rate the likelihood of the included statements on the following scale: Very unlikely, unlikely, unsure, likely, and very likely.
Discussion
This manuscript presents the results of a survey of knowledge and perceptions about guardianship among resident physicians across a variety of specialty and training years. Resident physicians reported uncertainties across some domains and confidence across others. Guardianship represents a nuanced and complex topic, complicated by variability across federal, state, and county regions (K. Zietlow et al., 2022). Consequently, resident physicians’ reported confidence in certain domains of guardianship may not align with medico-legal realities.
Over half of resident physicians believe that guardianship promotes certain positive outcomes: selection of an appropriate code status, selection of a safe discharge destination, appointment of home health aides, and safe management of patient finances. However, in many states, guardians are not permitted to change a patient’s code status to “do not resuscitate” or consent to withdrawal of life-sustaining treatment in the absence of previously documented advanced directives or a court order (K. Zietlow et al., 2022). While guardians may select a discharge destination or facilitate home care services, patients must meet financial eligibility criteria or must privately pay for these services. Lastly, due to a lack of standardized education and training requirements for prospective guardians, even with guardianship in place, patients may not receive appropriate management of their medical or financial affairs (Aviv, 2017).
Conversely, resident physicians are least likely to believe guardianship leads to expedited placement into a facility, increased medication adherence, increased adherence to patient’s care preferences, or avoidance of institutionalization. Resident physicians are correct in that guardianship does not ensure expedited placement into a facility. The process of appointing a guardian often takes several weeks or more, due to multiple statutory requirements. Issues of medication adherence are ethically fraught, as forcible administration of medications may not be practical, safe, or even legal. Exceptions, such as long-acting injectable psychotropic medications, are highly state-specific and often require a court order (Substance Abuse and Mental Health Services Administration [SAMHSA], 2019). There is an unfortunate paucity of literature assessing how guardianship may affect care outcomes or the alignment of care with patient preferences, which may contribute to resident physicians’ uncertainty.
In 2022, the “International Code of Medical Ethics of the World Medical Association” emphasized the need for physicians “to respect the dignity, autonomy, and rights of the patient” (Parsa-Parsi, 2022). To honor this ethical imperative and allow appropriate guidance and advocacy for our aging population, we argue physicians must receive proper education and gain a clinically-relevant understanding of surrogate decision-making. It is important to emphasize that patients with cognitive deficits retain the right to make their own decisions, unless they are deemed to lack global capacity through a court directive. In such instances, a guardian may be appointed, effectively removing those rights from the patient. Therefore, making an accurate assessment of a patient’s capacity is vital, and deeming a patient to lack such capacity should not be made frivolously.
Notably, education on guardianship is more robust within the field of psychiatry and pediatrics, but content in these fields is highly specific to the patient population they serve. Therefore, there is a crucial need to develop specific curricula on guardianship that is applicable to older adults facing cognitive and functional changes, which can be further complicated by geriatric syndromes, such as dementia. Principles from such curricula can also apply to other common clinical scenarios that physicians may encounter, such as neurodegenerative diseases (e.g., Parkinson’s disease) or traumatic brain injury. Because there is a paucity of research on how guardianship affects patient outcomes, a potential area of future research could examine outcomes of patients managed by resident physicians who received specific training on guardianship and surrogate decision-making compared to those who did not.
Limitations of our study include a 28.8% response rate, and that it was conducted at a single institution. The small sample size limits our ability to do further statistical analysis (e.g., to determine whether perceptions correlate with specialty and/or level of training). Our exploratory questions did not specify the scope of guardianship, nor did we differentiate between a known entity versus a trained professional serving as guardian, which may affect respondents’ perceptions.
This study highlights resident physicians’ self-acknowledged uncertainty and inconsistency over important guardianship components and provides a basis from which to develop curricula addressing the important areas of surrogate decision-making, as well as the ethical and medico-legal aspects of guardianship. Our institution is currently piloting a curriculum on guardianship for IM and FM resident physicians, and based on initial unpublished data, the curriculum has been well-received. We suggest resident physician training programs provide more intentional education and training on the process of guardianship: understanding the aspects of care which guardianship can facilitate, the ethical standards by which guardians are expected to adhere, the limitations and drawbacks of guardianship, and lastly, whether potential alternatives to guardianship have been explored (Peterson et al., 2021). Although we acknowledge that there are several competing demands for resident physicians’ time, we strongly believe such curricula will allow us to better serve our aging population and provide valuable care to a clinically vulnerable population.
Footnotes
Acknowledgements
The authors would like to thank James Fitzgerald, PhD, for his contributions to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.