
Abstract
Adults are encouraged to discuss their end-of-life health care preferences so that their wishes will be known and hopefully honored. The purpose of this study was to determine with whom older adults had communicated their future health care wishes and the extent to which respondents themselves were serving as a surrogate decision maker. Results from the cross-sectional online survey with 294 persons aged 50 and older reveal that among the married, over 80% had a discussion with their spouse and among those with an adult child, close to two thirds (64%) had. Over a third had discussed preferences with an attorney and 23% with a physician. Close to half were currently serving as a surrogate decision maker or had been asked to and had signed papers to formalize their role. 18% did not think that they were a surrogate but were not sure. More education is needed to emphasize the importance of advance care planning with a medical professional, especially for patients with advanced chronic illness. More education and research about the role of surrogate medical decision makers is called for.
Introduction
Despite the national push to do so, most American adults have not completed an advance directive (Kossman, 2014). Advance directives include Durable Power of Attorney for Health Care, in which an agent is named as a surrogate decision maker; a Living Will, in which people can document their wishes in the event they are terminally ill; and a medical directive, indicating which interventions to pursue or avoid. The literature shows limited success of advance directives influencing the course of care (Cohen-Mansfield & Lipson, 2008; McMahan, Knight, Fried, & Sudore, 2013; Shapiro, 2015). Advance care planning, on the contrary, a process that entails a discussion of goals of care within the context of health status, prognosis, and patient preferences (Emanuel, von Gunten, & Ferris, 2000), has been shown to increase the concordance between patient preferences and the type of care they receive (Houben, Spruit, Groenen, Wouters, & Janssen, 2014). The purpose of this manuscript is to report findings from a pilot study which asked lay people about their communications related to advance directives and advance care planning.
Method
Sample
In spring 2016, an e-mail invitation to participate in a short online survey about advance directives and advance care planning was sent to 1,235 adults age 50+ who had signed up as STAR (Seniors Together in Aging Research—a registry of persons aged 50 or older who have agreed to be contacted and invited to participate in aging-related research at the University of Iowa) volunteers. The e-mail invitation and anonymous online survey were granted exempt status by the University of Iowa’s Institutional Review Board. Respondents received one invitation; there was no follow-up. Completed responses were received from 294 persons (24% response rate). Later, it was determined that if two people shared the same computer (e.g., married couple), the computer system would allow only one person to answer the survey, which may have lowered the response rate.
Respondent Characteristics
Seventy percent were women. About a third (31%) reported being between the ages of 50 and 64; 42% between the ages of 65 and 74; 24% between the ages of 75 and 84; and 3% of respondents were aged 85 or older. Almost all (98%) reported their race as non-Latino White. Three fourths of the respondents indicated that they had completed 4 years of college or more. Two thirds (68%) were from Johnson County where the University of Iowa is located. Most respondents (71%) had either a living will and/or a Durable Power of Attorney for Health Care.
Survey Instrument
The online survey instrument contained 26 closed-ended questions (with the possibility to explain the selected response) and the final question was open-ended and invited comments related to any question or to the topic in general. This article has been developed based on the responses to three questions (as well as any written comments submitted that were related to these questions):
“In the past five years, have you had a serious discussion with anyone to clearly communicate YOUR health care wishes in the event that you have a serious accident (or illness) and physicians believe you will never recover the ability to recognize yourself again?”
The answer set contained nine different types of people (spouse/partner, adult child, sibling, friend, physician/doctor, nonphysician health care worker, attorney/lawyer, religious/spiritual leader, and other). For example, the first question was worded as follows: “I have discussed my preferences with my SPOUSE/PARTNER.” For each, respondents were instructed to mark “yes” or “no” or “not applicable.”
The second question was as follows: “Has someone else appointed YOU as their medical decision maker, in case they can’t communicate their health care wishes in the future?” There were five possible answers:
Yes, I am already making decisions on behalf of someone else who can’t communicate medical wishes.
Yes, I have been asked to be the official decision maker on behalf of someone else and we have signed papers.
Yes, I have been asked to be the official decision maker, but we have not signed any papers.
No, at least I don’t think so.
No, I am sure I have not been appointed as a medical decision maker
And the third question for this manuscript is as follows:
“Assume you have a serious chronic illness that is expected to worsen and likely result in death over the next 3-5 years. Assume your physician offered to have a 30 minute conversation with you about your health condition and the medical decisions you might face over the next years, and was interested in helping you weigh the pros and cons of different medical options. Would you be interested in having that conversation with your physician?” With two possible answers (yes or no). Respondents were given space to explain their answer.
Data Analysis
Quantitative data were analyzed using descriptive statistics available through the online survey tool (Qualtrics). Responses to the open-ended question were collected through Qualtrics. All comments were read and categorized by the main question topics.
Results
As indicated in Table 1, the majority of the married respondents (83%) reported having had a serious discussion about future health care wishes with their spouse, and a majority with children (64%) had discussed preferences with an adult child. Discussions with close friends and siblings were less common. A higher percentage of respondents had discussed the issue with an attorney (38%) than with a physician (23%). Comments from respondents indicated confusion about with which physician they would or should have an advance care planning discussion, “I have multiple physicians providing my health care, so I am unsure of the physician with whom I would discuss these issues.” Another responded indicated, “I have not felt that any of the several doctors I see has talked with me about my TOTAL situation—too many specialists interested in only their specialty. My internist is TOO BUSY. I feel fragmented” (emphasis in the original).
Percent of Respondents Who Have Had a Serious Discussion About Future Health Care Wishes, and With Whom.

Note. In the past 5 years, have you had a serious discussion with anyone to clearly communicate your health care wishes in the event that you have a serious accident or illness and physicians believe you will never recover the ability to recognize yourself again? (2016 STAR survey, N = 294). STAR = Seniors Together in Aging Research.
Some respondents volunteered additional information related to their advance directive and wishes by typing in the open-ended comment section. Some volunteered it had been many years since they completed the advance directive document. For example, “I believe I addressed this about 25 years ago but have no idea where the documentation would be.” Another respondent wrote, “I know what I want but my legal paperwork is very old and needs to be changed since I have been divorced for 15 years.” One responded shared this comment, I went to the emergency room last year. At one point, a physician asked if I would want to be resuscitated if my heart stopped. I said no. The daughter who is one of those named as POA (power of attorney) was surprised, as was one of my sons who was with me, too. It is harder than I knew to make your loved ones fully understand what you want.
When asked about the desire to meet with a physician for 30 minutes to discuss a serious illness, 97% of respondents indicated, “yes.” One of the three people who answered “no” wrote that those decisions had already been made, no need to further discuss.
Findings reported in Table 2 show that more than half of the respondents (58%) indicated involvement as a surrogate decision maker on behalf of another person, including 4% who indicated that they are currently making decisions on behalf of someone else. About one quarter (24%) of the sample reported that they were sure that they had not been appointed as a surrogate decision maker and 18% did not think they had been, but were not sure.
Number and Percent of Respondents Who Are Surrogate Decision Makers.
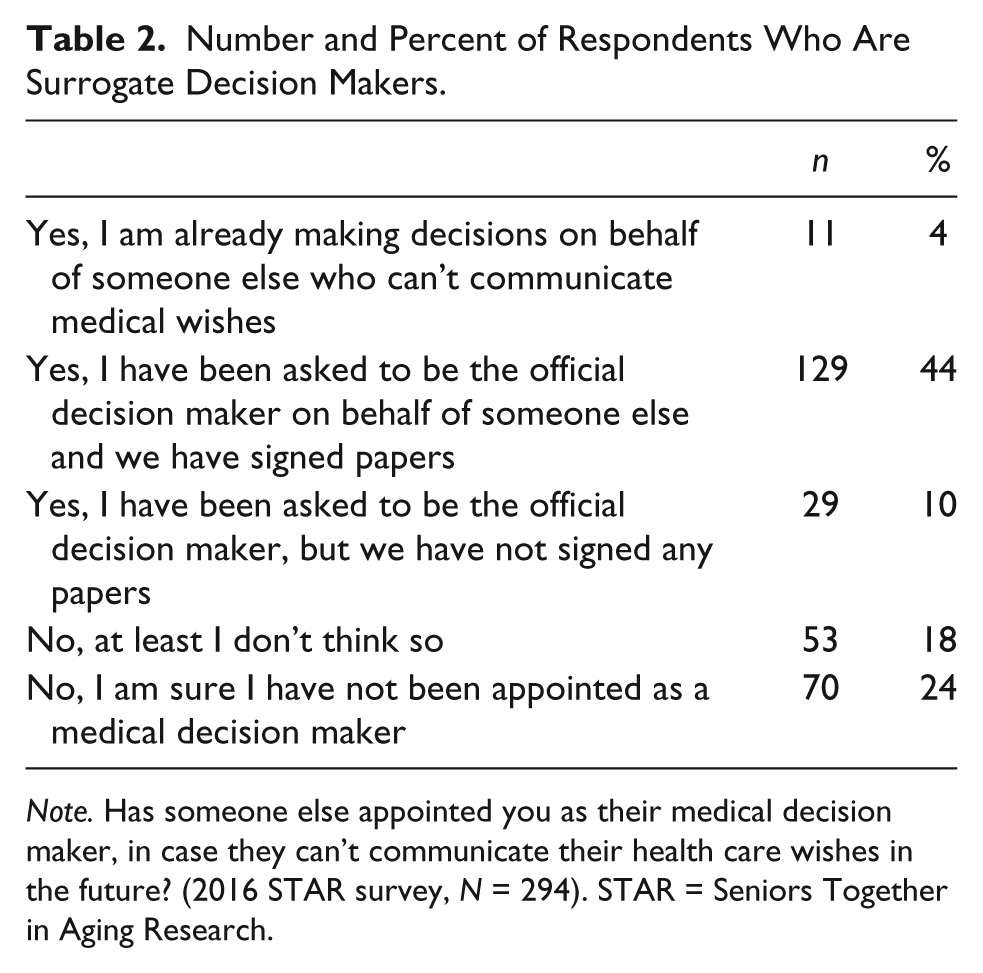
Note. Has someone else appointed you as their medical decision maker, in case they can’t communicate their health care wishes in the future? (2016 STAR survey, N = 294). STAR = Seniors Together in Aging Research.
Although this sample is not representative of the state of Iowa, it does reflect the views of well-educated older adults in Johnson County.
Discussion
There are three main findings derived from this study. First, more people had spoken with their attorney than with their physician about their future medical care preferences; second, the vast majority (97%) of respondents would want to engage in a 30 min conversation about treatment options related to a serious illness; and third, one in five respondents (18%) was not sure whether someone else had appointed them as a surrogate decision maker. Each is discussed below.
Higher Percentage Discussed Preferences With an Attorney
Why would a higher percentage of well-educated older adults discuss their future health care wishes with an attorney than with a physician? Terminology may provide a partial explanation, especially in the case of the “living will.” People may associate the term “wills” with lawyers. Advance directives that are notarized or witnessed are legal documents, and although states do not require a lawyer to be involved in the completion of advance directive documents, some people may prefer it. People may be more comfortable talking with an attorney because the meeting is generally private and not as rushed as a medical encounter in a hospital or clinical setting might be. Also, while it is not uncommon for an older adult to be seeing more than one physician, it is uncommon for an older adult to have more than one attorney. Unlike attorneys, a health care professional can engage in discussions about advance care planning, based on the patient’s specific medical status, prognosis, and medical options given the patient’s goals of care. Health care providers can also help patients understand the characteristics of a successful surrogate medical decision maker.
Physicians and other licensed independent providers inviting Medicare beneficiaries to discuss future health care preferences are expected to become more common because as of January 2016, Medicare reimbursed for “advance care planning services.” The Center for Medicare & Medicaid Services (CMS) provides billing code 99497 for Advance care planning including the explanation and discussion of advance directives such as standard forms (with completion of such forms, when performed), by the physician or other qualified health care professional; first 30 minutes, face-to-face with the patient, family member(s), and/or surrogate.) (https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/AdvanceCarePlanning.pdf)
Patients who report that they have already completed an advance directive can be encouraged to bring the document to their next clinic appointment. This invitation may encourage patients to locate their advance directive. Patients may know they have one, but do not know where it is. Being unable to locate the document diminishes its usefulness.
Given a Serious Diagnosis, Almost All Patients Would Like a 30 Minute Conversation With a Physician
Our findings indicate, that when faced with a life-threatening illness, most patients want to engage in discussions about options with physicians. An important part of an advance care planning discussion is the concept of “goals of care” (Kaldjian, Curtis, Shinkunas, & Cannon, 2009). Providers with patients who are confronting a serious illness should not only discuss current goals of care but could also take the opportunity to plant the seed that sometimes goals of care change as the patient’s health or functional status changes or as they gain experience with different types of interventions.
Physicians can ask whether patients have shared their goals of care, values, and preferences with the person appointed as the surrogate decision maker. Including the appropriate family member or surrogate in the advance care planning discussion can help increase the chances that the surrogate understands the patient’s preferences and will be better able to help communicate them as necessary (Emanuel et al., 2000). Depending on the circumstances, the provider and patient may want to have a private discussion first, and then bring the surrogate decision maker in at a subsequent appointment, or meet jointly for the initial meeting. CMS allows physicians to use the CPT billing codes more than once for a given beneficiary with the expectation that the reason for the multiple billings is documented. A well-informed surrogate decision maker, familiar with the patient’s goals of care and a sense of under what conditions the goals of care might change, can be a powerful asset to both the patient and the health care team.
Serving as Someone Else’s Surrogate
Advance care planning discussions with patients present an opportunity to ask the patient whether he or she is likely to be called upon to be a surrogate decision maker on behalf of someone else. Most people have probably never been asked this question, and findings from this sample of well-educated respondents suggest that many older adults simply do not know. (We were unable to identify other studies that asked this question, so it is not possible to compare our results with others). If people do not know whether they have been appointed as a surrogate, they are unlikely to have discussed values and preferences. If your patient suddenly finds him or herself in the role of a surrogate decision maker, it can be stressful, especially if they are not prepared. Also, being asked this question helps patients understand how important it is for them to communicate with their own surrogates. If, for whatever reason, physicians and other licensed independent providers are not available to discuss advance care planning with a patient, they should be aware of other advance care planning discussion options in the health care system or in community and make a referral.
A limitation of this study is the use of a convenience sample, comprised mostly of women and mostly of people who report themselves as non-Hispanic White. The sample also contains a higher proportion of college-educated older adults than in the general population. We have no information about people who did not respond. Despite these limitations, the findings suggest the need for more public education related to advance care planning and the benefits of engaging in these conversations with health professionals.
Many national efforts have encouraged adults to consider signing an advance directive, especially a health care power of attorney which names a surrogate decision maker. Future efforts should encourage people to engage in an advance care planning process with a physician or other knowledgeable health care provider. Although naming a surrogate is important, advance care planning has been shown to be more effective in securing the level and type of medical care the patient desires. Attorneys should encourage their clients to not only appoint a surrogate medical decision maker but, especially for their clients with advance chronic illness or a serious diagnosis, to engage in advance care planning discussions with a health care professional, who can engage in a goals of care discussion specific to the circumstances facing the patient. These findings also suggest that there is room for improvement in the education of surrogates and potential surrogates.
Footnotes
Authors’ Note
This information or content and conclusions are those of the authors and should not be construed as the official position or policy of nor should any endorsements be inferred by Health Resources & Services Administration (HRSA), U.S. Department of Health & Human Services (HHS), or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Health Resources & Services Administration (HRSA) of the U.S. Department of Health & Human Services (HHS) under grant number U1QHP28731 and the Geriatrics Workforce Enhancement Program.