
Abstract
Background:
Falls are the leading cause of fatal injury, and most common cause of non-fatal trauma, among older adults. We sought to elicit older patient’s perspectives on fall risks for the general population as well as contributions to any personal falls to identify opportunities to improve fall education.
Methods:
Ten patients with a history of falls from inpatient trauma and outpatient geriatric services were interviewed. Transcripts were analyzed independently by five individuals using triangulation and constant comparison (NVivo11, QSR International) to compare fall risks to fall causes.
Results:
All patients reported that either they (9/10 participants) or someone they knew (8/10) had fallen. Despite this, only two personally worried about falling. Patient perceptions of fall risks fell into seven major themes: physiologic decline (8/10); underestimating limitations (7/10); environmental hazards (7/10), lack of awareness/rushing (4/10), misuse/lack of walking aids (3/10); positional transitions (2/10), and improper footwear (1/10). In contrast, the most commonly reported causes of personal falls were lack of awareness/rushing (7/10), environmental hazards (3/10), misuse/lack of walking aids (2/10), improper footwear (2/10), physiologic decline (2/10), underestimating limitations (1/10) and positional transitions (1/10). In general tended to attribute their own falls to their surroundings and were less likely to attribute physical or psychological limitations.
Conclusion:
Despite participants identifying falls as a serious problem, they were unlikely to worry about falling themselves. Participants were able to identify common fall risks. However, when speaking about personal experience, they were more likely to blame environmental hazards or rushing, and minimized the role of physiologic decline and personal limitations.
Introduction
Falls from standing represent a serious but preventable threat to the health of older Americans. Each year, approximately one in three adults over the age of 65 experiences a fall (Bergen et al., 2016). Of these, one in ten will sustain serious injury (Chang et al., 2004; Tinetti, 2003). Fall risk increases with age due to a number of factors, including decreased mobility, cognitive impairment, medications, dizziness, decreased visual acuity, environmental hazards, and postural hypotension (Graafmans et al., 1996; Pfortmueller et al., 2014; Rubenstein, 2006; Tinetti et al., 1995; Tromp et al., 1998). Importantly, in addition to physical injury, fall victims also experience significant psychological trauma that can result in self-limitation of activities and subsequent loss of independence (Tinetti et al., 1988; Vellas et al., 1987). With the US population aging rapidly, preventing falls, the adverse quality of life effects of fall-related injuries, and fall-related healthcare costs represents a critical goal for healthcare providers and public health practitioners.
The increasing prevalence of falls and fall-related injury has made fall prevention an important area of research. Because every patient (and every fall) is different and has multiple possible components, the approach to fall prevention is similarly multimodal. Fall interventions have focused on approaches such as exercise and strengthening programs (Guo et al., 2014; Sherrington et al., 2011), medication review and optimization (Gillespie et al., 2012), home hazard assessment (Gillespie et al., 2012; Lord et al., 2006), and combinations of all of these (and other) elements (Gillespie et al., 2012; Goodwin et al., 2014; Pfortmueller et al., 2014). However, some studies have shown that patients often refuse to participate in such programs even if the intervention has been proven to be effective (Day et al., 2011). This is possibly because older adults, particularly those who have not fallen, tend to minimize their risk of falling and may find fall interventions irrelevant to their personal circumstances (McMahon et al., 2011; Peach et al., 2017). Understanding how older adults perceive fall risk may help tailor fall interventions and could improve adherence to recommended interventions.
In this qualitative study, we focused on patient perspectives of what caused their personal falls and assessed knowledge of known fall risks for the general aging population. Our goal was to identify gaps in perceived fall risks and actual fall causes to provide further primary data from the intended targets of fall prevention interventions on ways to improve adoption and efficacy of existing fall prevention programs.
Methods
We conducted a qualitative study of older adult patients who had fallen or were at risk of fall based on age and frailty at the UMass Memorial Medical Center (UMMC). UMMC, a 781-bed tertiary care center spread across three campuses in Worcester, Massachusetts is the clinical partner of the University of Massachusetts Medical School. It is the largest health care system in central Massachusetts, housing the region’s only level 1 trauma center. This trauma center evaluates approximately 2,500 trauma patients annually, nearly 40% of whom present as trauma patients due to falls from standing. Institutional Review Board approval was obtained prior to beginning the study. Patients aged 65 or older who had been treated for a fall at the UMMC trauma center or who were long-term patients of the UMMC outpatient geriatric clinic were eligible for the study if they were proficient in spoken English and had cognitive ability to participate in a face to face interview. Eligible patients were referred by the trauma service due to history of treatment for a fall or were referred by the geriatrics outpatient team due to history of fall or perceived fall risk by the provider. Referred patients were approached by the study team either in person at the conclusion of a clinic visit or by letter to participate in the study. Participation was voluntary and required the ability to present for a 1-hour face to face semi-structured interview.
Interviews were conducted in quiet offices located in either the trauma surgery clinic or the geriatrics outpatient clinic. All patients were required to sign a formal written consent for participation on the day of the interview. The consent acknowledged the voluntary nature of participation, the ability to terminate the interview at any time, and consent to have the interview recorded. Interviews were conducted by one or two research assistants lasting approximately one hour and recorded using a digital tape recorder. Each participant also completed a questionnaire with basic demographic and health information and completed a Mini-Mental Status Exam (MMSE) on the day of the interview (Folstein et al., 1975). The MMSE was used as a clinical descriptor and was not employed as a screening tool so patient results did not affect their inclusion in the study. Participants were offered to rest or to take a break, if needed, and water, other cold beverages, and appropriate snacks were provided should the participants require such during the interview.
Recorded interviews were professionally transcribed in a HIPPA compliant manner. Pseudonyms were applied to maintain anonymity and transcripts were uploaded into NVivo V11 (QSR International, Melbourne Aus) for qualitative analysis. The study plan was to enroll up to 20 participants, 10 from each clinical site or until theme saturation, whichever occurred first. To determine theme saturation, the two study team members (JW, CC) who conducted interviews also undertook a process of continuous coding as new data were being acquired and concluded theme saturation by the tenth interview. Therefore, further enrollment was halted. Interviews were conducted from July 2012 to June 2013.
Coding was then conducted by an independent team of five analysts (TC, BN, AC, KS, PM) who had not previously participated in conducting interviews or measuring theme saturation. After appropriate training in qualitative analysis and coding, two teams were formed, and transcripts were analyzed in numerical order by one team (starting with transcript one) and in reverse order by the other team (starting with transcript 10). Coding of each transcript was conducted independently with a weekly meeting to review content coded into existing and new themes based on the entry of two new transcripts into the analysis. This resulted in two independent reviews that overlapped ensuring that by the end of coding, each transcript was subject to analysis including all of the themes identified from other transcripts. Identification and grouping of themes was performed under the principles of grounded theory also known as the inductive approach where initial analysis is undertaken with attention to specific small concepts which are then grouped together into broader themes (Bradley et al., 2007). The analytic team then examined the created themes, resolved discrepancies and developed a coding taxonomy. Similarly coded text was then compared in order to expand on existing concepts and identify any new themes using the constant comparative method (Glaser & Strauss, 1967). Coding overlap was quantified in order to gauge the validity of the themes identified by analysts. Adjudication was performed by the PI (HS) when disagreements over theme classification occurred. In this iteration of our study, theme saturation was achieved by the sixth transcript. Therefore, we concluded, as the original interviewers had, that no further enrollment in the study was required.
Results
There were six women and four men enrolled in the study. The majority (7/10) were between the ages of 71 and 80 years. All participants were Caucasian, and average MMSE of 28 (out of 30), indicating normal cognitive function, with a low score of 20. Three patients reported using walking aids consistently, either a walker, cane, or both. None used a wheelchair. All patients were taking prescription medications with a range of 3 to 5 separate substances. Six reported being on anticoagulants. One participant was taking chronic narcotics for chronic pain. The most common reported medical co-morbidities were high blood pressure (9/10), high cholesterol (8/10), and arthritis (6/10).
Patient Understanding of Personal Health and Fall Risk
When asked about their current state of health, and specifically their
Representative Quotes From 10 Community Dwelling Adults Over 65 Regarding Perception of Personal Health and Fall Risk.
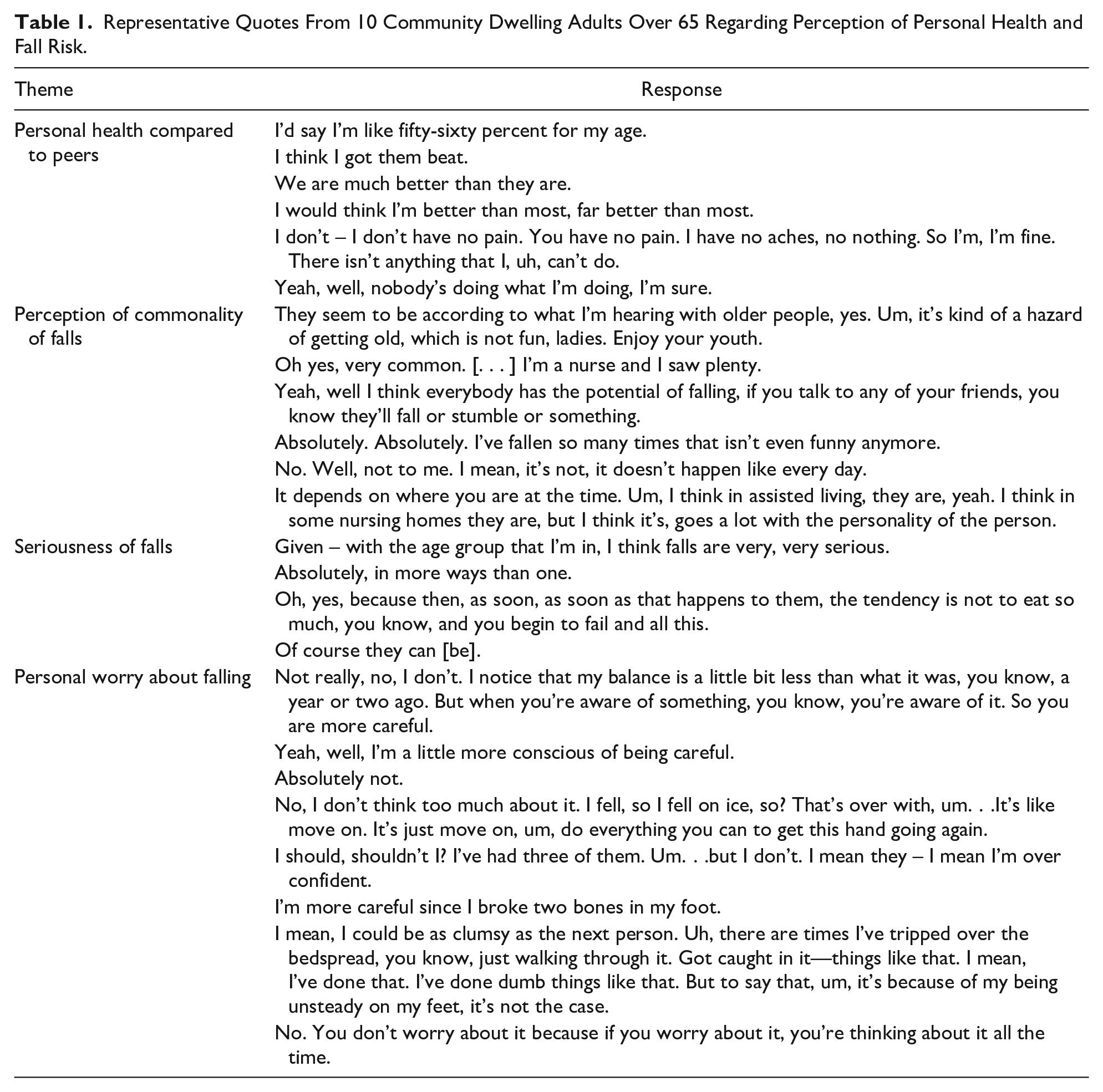
Eight participants reported that someone close to them had fallen. All participants except one reported a personal fall and fall-related injury. When speaking about
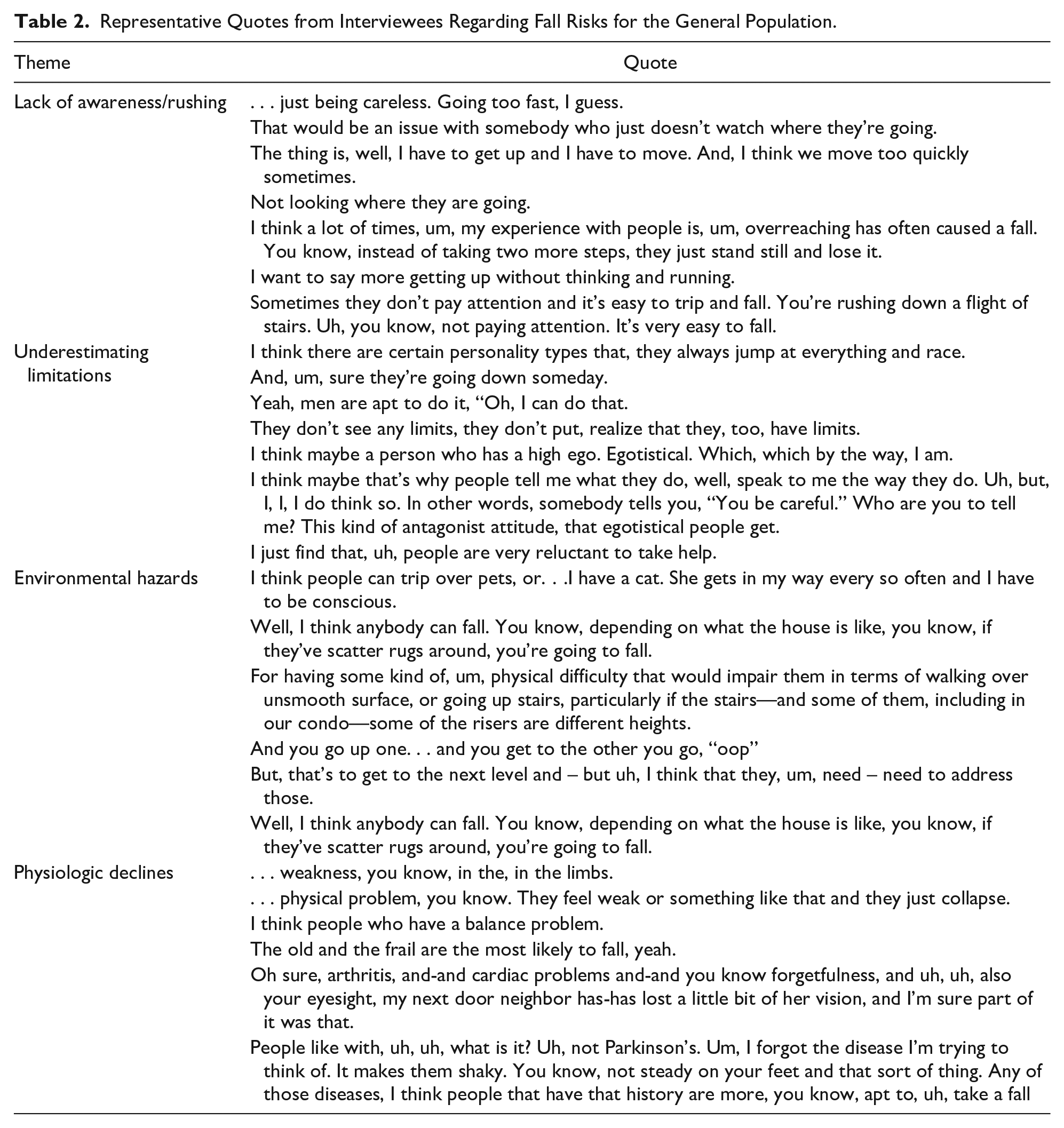
Patient Identified Fall Risks
Overall, patients identified several factors that would predispose an individual to a fall (“fall risks”) and also reflected on the causes of their own falls (“fall causes”). Quotes regarding patient perceived fall risks can be found in Table 2. The most commonly identified fall risk was
Representative Quotes from Interviewees Regarding Fall Risks for the General Population.
Patient Perceptions of Their Own Fall Causes
Patients were asked to comment on factors they believed contributed to their own falls. Themes identified were similar to those identified as fall risks but were mentioned with different frequencies. For example, only 2/10 participants stated that their fall was due to
Representative Quotes From Interviewees Regarding Causes of Their Own Falls.

Discussion
In this qualitative study of a cohort of older adult patients, we found that, although our participants believed that falls were a common and serious problem for people their age, participants were not personally concerned about falling. This is despite that all of them had either fallen themselves, or known someone who had fallen and been injured during said fall. In general, our cohort successfully identified what placed individuals at risk for falling and were able to list many risks that are commonly reported in the literature. However, when asked what caused falls either in their own lives or for those they knew, they often did not list the same factors as contributory. This indicates that although older adults may understand fall risks on the conceptual level, they may be less likely to see them as applicable to their own life situation, which they seemed to view through rose-colored lenses. This implies that fall education may need to focus less on the facts and didactics of fall risks and place greater emphasis on making risk modification seem personally relevant. Importantly, the majority of our cohort did believe that their falls could have been prevented with appropriate interventions, indicating that there is an opportunity for effective fall education in this population.
In this study, nine of our ten participants had personally suffered a fall and eight participants knew someone who had fallen, with seven participants reporting that both they and people they knew had fallen, a testimony to the ubiquitous nature of falls in the elderly population. Our participants generally seemed to understand both the commonality and seriousness of falls and specifically alluded to the potential of falls to cause serious mental and physical harm. This is an important concept in the fall literature as falls can often cause injuries that can subsequently cause anxiety and avoidance of physical activity leading to further physiologic decline (Delbaere et al., 2004; Friedman et al., 2002). Our findings indicate that this fear is indeed pervasive in community-dwelling older adults and fall education that exacerbates this anxiety and perpetuates sedentary behavior could therefore be counterproductive, given that maintaining daily physical movement is known to be an important preventative measure for fall reduction over time(Hamed et al., 2018; Liu-Ambrose et al., 2019; Roitto et al., 2018).
The literature has demonstrated that older adults often have difficulty assessing their functional and physiologic decline and frequently overestimate their general health(Ferraro, 1980; Idler, 1993). This is likely due to multiple factors, such as the slow pace of decline which may make it hard to notice and an unwillingness to accept changes in baseline status. Our study echoes these findings, as when asked about their perception of their own health nearly all of our cohort believed they were at least as healthy as other people their age, and all but one believed they were healthier than their peer despite the fact that the majority of our cohort had major health issues. Additionally, very few cited physiologic decline as being a cause of their own personal fall despite the fact that the majority had stated they knew that physical decline is a general fall risk. This indicates a disconnect between what our population knew to be generally true on a conceptual level and what they felt was true and applicable for their circumstances. Similarly, despite understanding the serious nature of falls for individuals in their age group, and that nearly all of them had suffered a personal fall, our cohort did not personally worry about falling. It is difficult to know if this represents cognitive avoidance of anxiety-provoking issues (both falls and physiologic decline in general) or if they truly see themselves as healthy and low risk for falls, as is common in this age group (Hughes et al., 2008; Shuman et al., 2019) Regardless, these intellectual barriers may be difficult to overcome during fall education. Presenting fall prevention strategies in a positive light that emphasizes preserving current health and function rather than correcting “deficiencies” perceived by the provider may fit better with patients’ worldview and make fall education more palatable to patients.
When asked about general fall risks, our cohort was able to identify several environmental hazards that can increase ones’ risk of falling, such as household obstacles, improper or non-use of mobility aids, and improper footwear. They also mentioned these as causes of their own falls indicating that as a group they are relatively accepting of the role of their physical surroundings in whether or not they suffer a fall. However, fall prevention programs focused on environmental modifications, such as grab bars in showers or traction rugs, have had varying levels of success in the literature (Cumming et al., 1999; Gill et al., 2000; Lord et al., 2006). One reason for this could be lack of awareness or rushing (another theme identified by our cohort) which has the potential to obviate the benefits of environmental modifications. Importantly, the most commonly listed cause of personal falls in our cohort was “not being careful,” indicating that patients do understand the importance of environmental awareness and may be open to fall education that address this area. Our results indicate that focusing on environmental awareness not only could increase the effectiveness of environmental modifications but, crucially, also represents an area of fall education that older adults may be particularly open to.
Our cohort did not mention clinical factors, such as polypharmacy, hypoglycemia, or postural hypotension, as either known fall risks or causes of their fall. However, aging-associated problems such as accumulating co-morbidities, polypharmacy, malnutrition, and cognitive impairment have been implicated in among older adult patients(Boyd et al., 2005; Di Iorio et al., 1998; Fried et al., 2004; Hickey et al., 1997; Higashi et al., 2007). This represents an important gap in patient understanding of physiologic causes for falls and should be emphasized in fall education programs. Importantly, however, the technical nature of these elements may mean that clinicians may need to assume the responsibility for modifying these risk factors by monitoring patients’ medications and checking parameters, such as blood glucose and orthostatic blood pressures, at visits. Our results suggest that patients are unlikely to be able to adequately asses these elements or make the connection between them and their falls.
Limitations of this study included the small sample size and the demographics of the study participants, as only ten patients were interviewed in this study and all were Caucasian. There was also a sample bias because all patients were community-dwelling. Additionally, there is likely a degree of recall bias which could be further exacerbated due to our patients’ age and social desirability bias among those who felt that interviewers would want to hear certain responses. However, overall, we believe our study highlights many important gaps in both patient knowledge of fall risks and what they are willing to accept as being personally applicable. Using these findings to create a fall education program that addresses these issues could result in more successful implementation of risk factor modification.
Footnotes
Acknowledgements
We are grateful to Jennine Weller, MD now in the Department of Surgery at Johns Hopkins Medical School for her early efforts organizing this project.
Authors’ Note
This research was previously presented at the American Geriatrics Society Annual Scientific Meeting, Orlando, FL May 4, 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.