
Abstract
Telehealth has been widely accepted as an alternative to in-person primary care. This study examines whether the quality of primary care delivered via telehealth is equitable for older adults across racial and ethnic boundaries in provider-shortage urban settings. The study analyzed documentation of the 4Ms components (What Matters, Mobility, Medication, and Mentation) in relation to self-reported racial and ethnic backgrounds of 254 Medicare Advantage enrollees who used telehealth as their primary care modality in Southern Nevada from July 2021 through June 2022. Results revealed that Asian/Hawaiian/Pacific Islanders had significantly less documentation in What Matters (OR = 0.39, 95%, p = .04) and Blacks had significantly less documentation in Mobility (OR = 0.35, p < .001) compared to their White counterparts. The Hispanic ethnic group had less documentation in What Matters (OR = 0.18, p < .001) compared to non-Hispanic ethnic groups. Our study reveals equipping the geriatrics workforce merely with the 4Ms framework may not be sufficient in mitigating unconscious biases healthcare providers exhibit in the telehealth primary care setting in a provider shortage area, and, by extrapolation, in other care settings across the spectra, whether they be in-person or virtual.
Introduction
Telehealth holds great promise for enhancing primary care access among older and vulnerable adults especially if they need transportation support (Gibbs et al., 2022). Studies have shown that telehealth utilization is associated with better outcomes in chronic disease management and reduced healthcare disparities across racial and ethnic boundaries (Bose et al., 2022; Dryden et al., 2022; McQuown et al., 2022). The emergence of the COVID-19 pandemic highlighted the need for telehealth for these individuals (Friedman et al., 2022; Patel et al., 2021; Powers et al., 2021). The CARES Act led to the rapid implementation of telehealth across the United States. Despite the CARES Act implementation, racial and ethnic minority individuals were found to lack access to telehealth and were at higher risk of discontinuation of care with resultant adverse outcomes (Adepoju et al., 2022; Rivera et al., 2021; Ryskina et al., 2021, Williams et al., 2023). Social determinants of health (SDH) encompass lack of access to information technology (i.e., broadband access) and low health literacy status, contributing to reduced telehealth utilization among racial and ethnic minority patients, especially among older adults (Bhatia et al., 2022; Frydman et al., 2022; Lam et al., 2020; Roberts & Mehrotra, 2020).
The Age-Friendly Health System (AFHS) aims to provide evidence-based care aligned with older adults and their caregivers’ preferences and goals (Age Friendly Health Systems, 2023; Fulmer et al., 2018). Embedded within locally available healthcare services, the AFHS is implemented for their beneficiaries (Phillips et al., 2021). The 4Ms framework of the Age-Friendly Health Systems model focuses on What Matters, Mobility, Medication and Mentation as essential components of evidence-based geriatric care across all care settings. (Age Friendly Health Systems, 2023; Dryden et al., 2022; Fulmer et al., 2018).
The 4Ms framework has been adopted as the standard for Nevada Geriatrics Telehealth Collaboration (NGTC). As the key metric for proper training on the 4Ms framework, we review documentation frequencies of the 4Ms components in primary care services, delivered via telehealth, in provider shortage areas of Southern Nevada. This study is an extension of our overarching endeavor into the particularly relevant topic of the racial and ethnic disparity in the care of older adults as the 4Ms framework is applied to their primary care via telehealth.
Methods
Design Overview and Recruitment Flow
This was a retrospective cross-sectional study of Medicare Advantage enrollees, 65 years of age and older, cared for by telehealth primary care providers in an urban not-for-profit organization in Southern Nevada. There were seven primary care sites, and over 100 providers. Supplemental Figure 1 depicts the recruitment flow diagram. Electronic Health Records (EHR) of 5,488 patients with video telehealth visits between July 1, 2021, and June 30, 2022, were compiled. Among 5,381 patients with active telehealth primary care visits, 301 patients were excluded due to incomplete data, and 107 patients were excluded due to either demise or attrition from the health system. Among 5,080 eligible patients, computer-assisted 5% random selection was then performed. We applied a weighting process of race and ethnicity proportions in a 5% random selection strategy (Gopal, 2016; von Elm et al., 2007). A total of 254 patients were then amassed for the final sample analysis, as it was estimated that a sample size of 254 was required for a 5% random selection from eligible 5,080 patients with a 95% confidence level and a 2.62% margin of error (Power and Sample Size in STATA Features, n.d).
4Ms Elements and Measurable Variables
The main outcome was the 4Ms components (What Matters, Mobility, Medication, Mentation) as documented in EHR. Two reviewers independently reviewed healthcare providers’ narratives (i.e., progress notes and phone notes) and billing information (Table 1. Definition of 4Ms elements) in EHR. Each 4Ms element was counted separately for a single encounter. When a single patient had multiple telehealth visits, 4Ms documentation was counted cumulatively. For example, Mentation was documented in the telehealth visit in September 2021; What Matters and Medication were documented in another telehealth visit in March 2022 for the same patient. Three elements of the 4Ms (What Matters, Medication, Mentation) were then counted for this patient. Each 4Ms element was counted dichotomously (yes or no). If disagreements arose between the reviewers, additional two reviewers were consulted until a consensus was formed.
Definition of 4M Elements.

CPT® = current procedural terminology is a uniform nomenclature for coding medical procedures and services by the American medical association; HCPCS® = healthcare common procedure coding system® is a set of healthcare procedure codes based on the American medical association’s current procedural terminology.
Measurable variables were race and ethnicity, age, gender, educational attainment, English proficiency, disability status, and weighted Charlson Comorbidity Index (CCI). Age was automatically generated from the participant’s date of birth to the data review date. Race and ethnicity, age, and gender information were extracted from the EHR administrative database. Race and ethnicity, education attainment, and English proficiency were self-reported. Race was divided into White, Black, and Asian/Hawaiian/Pacific Islander. Ethnicity was divided into Hispanic and non-Hispanic. Education attainment was structured into three categories—less than high school, high school, and college or more (Roberts et al., 2020). Limited English proficiency was defined as English not being the primary language, and if a patient reported difficulty communicating effectively in English with their healthcare providers, requested an interpreter, and marked their preferred language as “other than English” in EHR (Rodriguez et al., 2021). The “disability” variable was defined by any documentation of the following: 1) ambulatory difficulty (e.g., difficulty walking or frequent falls with or without injury); 2) self-care difficulty (e.g., difficulty bathing or transportation); 3) cognitive difficulty (e.g., difficulty with memory, recall, or decision-making due to a physical or behavioral health problem); 4) hearing difficulty; 5) vision difficulty (Roberts et al., 2020). As a measure of comorbidity, the weighted CCI was calculated (Charlson et al., 1987).
Statistical Analyses
To test our hypothesis that non-White patients were less likely to have 4Ms elements documented, we estimated multivariate logistic regressions with each 4Ms element as the dependent variable. We estimated two regressions for each outcome; the explanatory variable in the first model was race and the explanatory variable in the second model was ethnicity. Control variables included age, gender, educational attainment, limited English proficiency, disability status, and the weighted CCI.
Next, we evaluated the association between patient characteristics and 4Ms elements. We estimated multivariate logistic regressions with each 4Ms element as a dependent variable; age, gender, educational attainment, limited English proficiency, disability status, and weighted CCI were independent variables. We re-estimated the aforementioned model with either race or ethnicity as control variables. To avoid multicollinearity problems that were detected among the independent variables during the preliminary analysis, the stepwise approach was applied to obtain results from the parsimonious regression models (Stevens, 1996). All statistical analyses were two-tailed and a p-value less than 0.05 was statistically significant. STATA, version 17 (Stata Corp, TX, USA), was used for statistical analysis. This work was determined to be quality improvement/evaluation by the University of Nevada, Las Vegas Institutional Review Board (IRB), and not subject to IRB approval and oversight as human subject research.
Results
The sample in Table 2 consisted of 254 patients. In terms of race, 50.3% were White, 26.4% were Black, and 23.3% were Asian/Hawaiian/Pacific Islander. Among the patients, 24.4% were of Hispanic ethnicity. The mean age was 76.2 years with a standard deviation of 6.9 years. Regarding age distribution, 59.0% fell between 65 and 79 years old, while 41.0% were 80 years and older. Females accounted for 55.9% of the sample. In terms of education attainment, 31.9% had a high school diploma or less. Additionally, 30.7% had limited English proficiency. Concerning health conditions, 42.1% reported difficulties in ambulation, self-care, cognition, hearing loss, or vision. The distribution of patients based on the CCI was as follows: 31.9% had a CCI of zero, 50.8% had a CCI between one and two, and 17.3% had a CCI of three or higher.
Descriptive Statistics of Patient Characteristics.

Overall, What Matters was the 4Ms component with the highest documentation (62.2%) and Mentation the lowest (23.6%). Medication (48.4%) and Mobility (27.0%) were in the middle (Table 3). All 4Ms elements except Mobility were more frequently documented for White patients. Mobility was more frequently documented both in Asian/Hawaiian/Pacific Islander patients and non-Hispanic patients. What Matters was documented for 81.3% of White, 56.7% of Black, and 33.9% of Asian/Hawaiian/Pacific Islander patients. What Matters was documented for 77.6% of non-Hispanic patients and 14.5% for Hispanic patients. Mobility was documented for 32.7% of White, 11.9% of Black, and 33.9% of Asian/Hawaiian/Pacific Islander patients. Mobility was documented for 24.2% of Hispanic and 28.1% of non-Hispanic patients. Medication was documented for 54.7% of White, 37.2% of Black, and 47.4% of Asian/Hawaiian/Pacific Islander patients. Medication was documented for 38.7% of Hispanic and 51.6% of non-Hispanic patients. Mentation was documented for 28.1% of White, 17.9% of Black, and 20.3% of Asian/Hawaiian/Pacific Islander patients. Mentation was documented for 16.1% of Hispanic and 20.3% of non-Hispanic patients.
Descriptive Statistics of 4M Elements by Race and Ethnicity.
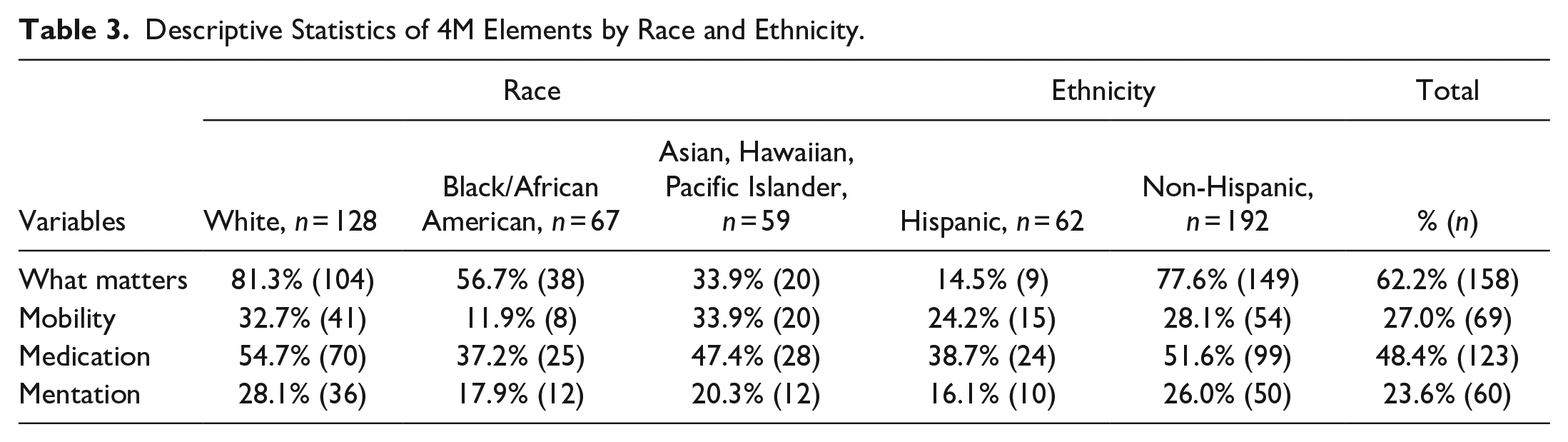
Table 4 demonstrates the association of race/ethnicity and 4Ms elements. Compared with White counterparts, Asian/Hawaiian/Pacific Islander patients were less likely to have documented for What Matters (adjusted odds ratio, aOR [95% confidence intervals, CI], 0.39 [0.13, 0.94] (p = .04)). Compared with non-Hispanic, Hispanic patients were less likely to be documented for What Matters (0.18 [0.04, 0.59] (p < .001)). Compared with their White counterparts, Black patients were less likely to be documented for Mobility (0.35 [0.17, 0.90] (p < .001)). There was no association between race/ethnicity and Medication. Similarly, no association was found between race/ethnicity and Mentation.
Association of Race/Ethnicity and 4M Elements.

Note. aOR = adjusted odds ratio; CI = confidence intervals.
Table 5 presents the association of patient characteristics and 4Ms elements. Compared with those who are 65 to 79 years of age, those who are 80 years and older were more likely to have documented What Matters, 1.37 [1.05, 2.04] (p = .01) and Medication, 1.55 [1.20, 1.90] (p < .001). Compared with those with high school or less education attainment, those with some college or higher education attainment were more likely to have been documented for What Matters, 1.64 [1.30, 1.96] (p < .001); Mobility, 1.39 [1.18, 1.62] (p < .001); Medication, 1.57 [1.32, 1.86] (p < .001); and Mentation, 1.92 [1.43, 2.50] (p < .001). Compared with patients with English proficiency, patients with limited English proficiency were less likely to have been documented for What Matters, 0.35 [0.14, 0.90] (p < .001); Mobility, 0.61; [0.32, 0.95] (p < .001); Medication, 0.55 [0.24, 0.93] (p < .001); and Mentation, 0.36 [0.08, 0.92] (p < .001). Compared with non-disabled patients, disabled patients were more likely to have been documented for What Matters, 1.82 [1.34, 2.65] (p < .001); Mobility, 2.54 [1.69, 3.68] (p < .001); Medication, 1.73 [1.19, 2.47] (p < .001); and Mentation, 2.26 [1.80, 2.96] (p < .001). Higher CCI score was associated with higher frequencies of documentation for What Matters, 1.11 [1.04, 1.17] (p < .001); Mobility, 1.18 [1.05, 1.46] (p < .001); Medication, 1.08 [1.02, 1.25] (p = 0.03); and Mentation, 1.17 [1.06, 1.20] (p < .001). These findings, including direction of the association and statistical significance, were unchanged in the model with either race or ethnicity as covariable.
Association of Patient Characteristics and 4M Elements.

Note. aOR = adjusted odds ratio; CI = confidence intervals.
Discussion
The purpose of the study was to examine the disparities across racial and ethnic boundaries in the 4Ms framework among telehealth recipients in primary care settings in a provider shortage area. This study examines the 4Ms documentation frequencies as key metrics for care quality in primary care delivered via telehealth and uncovers the disparities across the racial and ethnic groups when the 4Ms framework was applied. The overall frequencies of the 4Ms framework documentation, irrespective of the racial and ethnic groups, showed a lack of adherence by healthcare providers and varied highly among the four elements: 62.2% for What Matters, 48.4% for Medication, 27.0% for Mobility, and 23.6% for Mentation. While What Matters showed the highest adherence, there were significant differences among racial and ethnic groups. Only 33.9% of Asian/Hawaiian/Pacific Islander patients and 14.5% of the Hispanic patients had What Matters documented, whereas 81.3% for White patients and 77.6% for non-Hispanic patients showed documentation thereof. This disparity finding is consistent with previous national and local surveys which demonstrated comparatively less awareness of advanced care planning in racial and ethnic minority communities (Luth et al., 2022; Koss & Baker, 2017; Shen et al., 2020). In contrast, for Mobility, a statistically significant disparity was observed between Black and White patients only; Asian/Hawaiian/Pacific Islander patients showed higher documentation frequencies for Mobility than their White counterparts, though statistically non-significant (33.9% vs. 32.7%).
Of the 4Ms elements, Mentation was least documented overall. This is consistent with the study which speculated whether primary care providers were not proactive in managing mental health and neurodegenerative conditions (i.e., ADRD) via telehealth, as shown by the nationwide Medicare Advantage telehealth primary care claims data analyses (Powers et al., 2021). Telehealth may have exaggerated the disparity findings, as one recent study performed in one large healthcare system in the northeastern part of the U.S. showed non-White patients were less satisfied when telehealth was used as primary care modality during the COVID-19 pandemic (Bhatia et al., 2022).
Older patients had higher frequencies of 4Ms documentation across all elements. The same trend was also seen for those with higher educational attainment, English proficiency, comorbidity score, and disability status. These patterns were consistent with previous findings in telehealth primary care for Medicare enrollees, which showed higher claims rates for those with higher education attainment, comorbidity score, and disability status (Friedman et al., 2022; Powers et al., 2021).
The results of our study are limited by a single urban geographic area, study subjects being Medicare Advantage enrollees, in a non-profit healthcare organization, and in a provider-shortage area. Further studies are being planned for racial and ethnic disparities in 4Ms documentation at the NGTC partner sites with different profiles, both at the level of organizations and study subjects. Another limitation of the study was using self-reported race and ethnicity information, which was simplified into three races and two ethnicities and may not represent all races or those of mixed races.
Limitations notwithstanding, disparities across racial and ethnic boundaries in the 4Ms application, as shown in our study, are alarming. Greater awareness of their existence alone is not sufficient; methods to evaluate and mitigate them should be developed and implemented in geriatrics workforce training, especially for those who are at the frontline such as primary care, be it in-person or telehealth modality. Especially in a provider shortage area, such workforce training should be a high-priority strategy to enhance healthcare outcomes rather than a structural investment strategy (Griswold, 2022). As discussed, the Age-Friendly Health System 4Ms framework is an easily adoptable toolkit for promoting geriatrics workforce competency in local healthcare systems and other care settings (Age Friendly Health Systems, 2023; Fulmer, Mate, & Berman, 2018).
Conclusion
This study examines racial and ethnic disparities in 4Ms documentation frequencies in telehealth primary care settings in a provider shortage area. The findings highlight the need for greater awareness of unconscious biases healthcare providers may exhibit in the care of older adults from racial and ethnic minority groups. Mitigation strategies may need also to be developed and implemented to achieve equity in the care of older adults, irrespective of racial and ethnic backgrounds. Incorporating the findings of this study may play a pivotal role in delivering high-quality primary care to older adults in a provider shortage area via telehealth.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214231189053 – Supplemental material for Racial and Ethnic Disparity in 4Ms among Older Adults Among Telehealth Users as Primary Care
Supplemental material, sj-docx-1-ggm-10.1177_23337214231189053 for Racial and Ethnic Disparity in 4Ms among Older Adults Among Telehealth Users as Primary Care by Ji Won Yoo, Hee-Taik Kang, Ian Choe, Laurie Kim, Dong-Hun Han, Jay J. Shen, Yonsu Kim, Peter S. Reed, Iulia Ioanitoaia-Chaudhry, Maria Teresa Chong, Mingon Kang, Jerry Reeves and Maryam Tabrizi in Gerontology and Geriatric Medicine
Footnotes
Author Contributions
All authors meet the criteria for authorship stated in the Uniform Requirements for Manuscripts Submitted to Biomedical Journals. Ji Won Yoo, Hee-Taik Kang, Laurie Kim, Dong Hun Han, and Jay J. Shen conceived the study and acquiesced, analyzed, and interpreted the data. Yonsu Kim, Ian Choe, Peter Reed, Jennifer Carson, Patti Swager, Leslie Baker, Iulia Ioanitoaia-Chaudhry, Maria Teresa Chong, Mingon Kang, and Maryam Tabrizi conceived the study and interpreted the data. All authors drafted the work and revised it critically. All authors gave the final approval of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Ji Won Yoo, Jay J. Shen, and Peter Reed’s HRSA GWEP U1QHP33069; CARES ACT COVID-19 Telehealth T1MHP39045; Nevada Aging Disability Services Division Older American Act Infrastructure and Capacity Building. Sponsor’s Role: The funding sources had no role in the design or conduct of the study; in the collection, analysis, or interpretation of the data; in the preparation, review, or approval of the manuscript; or in the decision to submit the manuscript for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.