
Abstract
Objectives: Older adults have been disproportionately affected by COVID-19. The primary goal of this study is to determine the socioeconomic effects on psychosocial factors among low-income independent-living older adults, in an urban setting, during the COVID-pandemic. Methods: Participants were recruited through Virginia Commonwealth University’s Richmond Health and Wellness Program. Telephone surveys (n=100) were conducted using the Epidemic – Pandemic Impacts Inventory Geriatric with the Racial/Ethnic Discrimination addendum. Responses were analyzed for income and education effects across seven domains: home life, social activities/isolation, economic, emotional health-wellbeing, physical health, COVID-infection history, and positive change behaviors/experiences. Results: The sample population was between 51 and 87 years of age, 88% were Black, 57% reported incomes of $10,000/year or less, and 60% reported a high-school education or less. There were income effects for social activities/isolation (f = 3.69, p<.05) and positive change (f = 8.40, p<.01), and education effects for COVID History (f = 4.20, p <.04). Discussion: Overall results highlight the social patterns for a diverse sample of low-income urban older adults; education and income are identified as risk factors for social losses, COVID-infection experiences, racial/ethnic discrimination during the COVID-pandemic, and positive change behaviors.
In late 2019, a viral pathogen causing severe respiratory issues and deaths was detected in Wuhan, China (severe acute respiratory syndrome coronavirus 2; SARS-CoV2) triggering multi-national lockdowns. By March 11, 2020, the World Health Organization declared COVID-19 a pandemic, since this time communities have implemented several unprecedented changes that have greatly affected many lives (World Health Organization, 2020). Unfortunately, the impact of COVID-19 and its particular effects have not been analogous for all populations, as many vulnerable populations were already facing challenges related to health and social disparities that were only intensified as a result of the pandemic. Although certain communities have been able to make necessary adjustments, this has been more difficult, and in some instances, not as feasible, for older and lower-income adults. There are a range of contextual factors that are important to understand in order to determine the resources needed by vulnerable populations. The primary goal of this study is to determine the socioeconomic effects on psychosocial factors among low-income independent-living older adults, in an urban setting, during the COVID-pandemic.
Specifically, in Richmond, Virginia, data reveals that African American communities have been disproportionately affected by COVID-19 as they have comprised most hospitalizations and deaths, even though African Americans and White, Non-Hispanics, are equally represented within the city. African American residents account for more than 60% of hospitalizations and deaths, while whites made up about 14% of COVID-19 patients and a third of the fatalities in the same timeframe (Northrop, 2020; Virginia Department of Health, 2021a). This trend is not exclusive to Richmond either, as similar numbers have been evident nationally (Artiga et al., 2020; Thebault et al., 2020). A June, 2021 Virginia Department of Health report (Virginia Department of Health, 2021b) found that people living in census tracts where more than 40% of the population is below the poverty level were 2.3 times more likely to die from COVID-19 than residents in areas with the lowest poverty rates. Census tracts are geographic regions that frequently coincide with the limits of cities and often mark areas of persistent poverty. These findings highlight the fact that poverty is complex and not evenly distributed resulting in group differences for individuals living below the poverty level. It is suspected these COVID-related health disparities may be due to long-standing systemic health and social disparities that have placed racial and ethnic minority groups at greater risk for infection (Centers for Disease Control and Prevention, 2020a).
Data has shown vulnerable minority populations are more likely to live in densely populated urban areas, like Richmond, with many residing in multi-family dwellings or crowded living conditions, where social distancing is challenging (Artiga et al., 2020; Centers for Disease Control and Prevention, 2020b). Racial and ethnic minority groups are also disproportionately overrepresented urban settings; with high utilization of resources such as healthcare facilities and public transportation, where they face an increased COVID-19 risk exposure (Centers for Disease Control and Prevention, 2020a). For lower-income groups, this can be detrimental to their health, because they face more challenges accessing COVID-19 related testing and treatment due to health care barriers (Artiga et al., 2020). In addition, African American individuals are more likely to have underlying conditions, such as obesity, hypertension and diabetes, which have higher risk for severe COVID-19 outcomes (Centers for Disease Control and Prevention, 2020a).
Many of these concerns are significant to the older adult population, considering 80% of older adults have at least one chronic condition, and 65% have two or more (National Council on Aging, 2017). The vulnerabilities of the older adult population have continued to be elucidated as eight out of ten COVID-19 related deaths in the United States have been among adults 65 years of age and older (Centers for Disease Control and Prevention, 2020c; Centers for Disease Control and Prevention, 2020d). As part of the pandemic, newly developed restrictions and social distancing measures have reduced access to necessary medical and psychosocial support resources for community-dwelling older adults, which has increased the risk for worsening current chronic conditions (Mills et al., 2020). Virtual visits with loved ones and healthcare providers have shown improvements in mitigating these effects; however, this has only been beneficial for those who have access to telemedicine/internet resources (Mills et al., 2020). It is especially pertinent to recognize the role socioeconomic factors have on high-risk marginalized populations of low-income older adults, many whom prior to the pandemic were already struggling with healthcare access and social isolation, factors that complicate one’s ability to safely navigate and adjust to COVID-19 related challenges (Healthy People, n.d.; Rollston & Galea, 2020).
In this study, we report on the self-reported negative and positive changes experienced by a low-income community-based older adult populations living in an urban city setting during COVID-19. The primary goal of this research is to increase an understanding of how the COVID-19 pandemic is impacting low-income minority older adults with known increased risks of health disparities, multiple chronic conditions, disabilities, and shortened longevity. Additionally, we examine self-reported positive change experiences used by low-income older adults to maintain resiliency in response to changes caused by the pandemic. These observational results will support future intervention-based research to personalize support services for low-income community-based older adults.
Methods
Setting and Participants
The setting includes five Section 8 housing buildings in which residents receive rent subsidies and income-based rent adjustment and individuals residing in the East End of the city. The VCU Richmond Health and Wellness Program (RHWP) is available to residents in the Section 8 housing buildings and provides an established model to interface with Richmond older adults. RHWP provides care navigation and support services to individuals residing in five housing apartment buildings designated for low-income older and disabled adults
Procedure
This cross-sectional pilot study used a convenience sampling approach, was approved by VCU’s Institutional Review Board to ensure standard ethical considerations in research including privacy, confidentiality, protections of vulnerable populations and all participants provided verbal consent. Because of the need for rapid data collection and analysis to identify and quickly respond to any identified needs, a mixed-method convergent design (qualitative and quantitative data were collected in a parallel process) was used for this study. This paper reports on the quantitative survey data collected with the qualitative interviews reported in a separate publication. Data collection took place from the 25th of June to 17th of August 2020, in Richmond, Virginia, 3 months after the first confirmed COVID-19 case in the state, with 16,096 cases and 255 deaths (Virginia Department of Health, 2021c). Mask mandates were in effect, with retail and places of worship re-opened with capacity restrictions in place. Study participants were recruited during the RHWP telephonic wellness visits and through community partner referrals. All participants received gift card incentives. Two trained research assistants conducted the surveys through telephone interviews with data collection in Research Electronic Data Capture (REDCap) (Harris et al., 2009).
Pandemic Survey
Demographic data collected include age, sex, race, ethnicity, income before taxes, social living situation (i.e., living alone), and education. The Epidemic – Pandemic Impacts Inventory Geriatric Adaption (EPII-G, 92 items) survey is used to learn about the impact of the coronavirus disease pandemic across social, physical, and emotional health domains (Grasso et al., 2021; Manning et al., 2020). Participants are asked “Since the coronavirus disease pandemic began, what has changed for you?” with response options of “yes”, “no” or “not applicable” (NA) across each domain. The positive changes domain of the EPII-G includes 19-items used to assess positive change behaviors which are measured across a range of social and physical domains (e.g., relationships, physical activity, sleep, substance use). Examples of questions included, “improved relationships with family and friends,” “increased exercise or physical activity,” and “more time outside and less screen time on devices.” A racial/ethnic discrimination addendum (15-items) was added to measure the impact of the COVID-19 pandemic on individuals in the context of discrimination in physical health, infection history, physical distancing, and quarantine domains (Grasso et al., 2021; Yang et al., 2022).
Each item in the EPII surveys contains a response set that includes an answer that pertains to the participant (Yes and No, and Not applicable). A score for each participant was computed by scoring 1 for a “yes” and zero for “no”. A total score for the EPPI-G and racial/ethnic discrimination addendum was computed which comprised of the sum of the “yes” responses for each participant. This was then converted to a percentage score by dividing the total score by the sum of “yes” and “no” responses. NAs were removed from the analysis since individuals could not increase their score by responding to a question which did not apply to them. A higher percentage positive score indicated a greater proportion of positive changes.
Preliminary empirical tests were completed using person-centered latent class analysis (LCA) supporting the EPII as an instrument for evaluating sociodemographic differences across domains of home life, social activities and isolation, economic, emotional health and wellbeing, physical health, infection history, and positive change behaviors (Grasso et al., 2021). In this study, the EPII scales are found to have good internal consistency and reliability (Cronbach’s α= .66).
Additionally, participants’ emotional state since the COVID-pandemic were assessed by asking if participants, “since the corona disease pandemic have you felt or experienced any of the following?” (0 = No, 1 = Yes); depression, fears, nervousness, sadness, worry, loss of interest in usual activities, and loneliness. These surveys were combined with qualitative interviews designed to measure meaningful experiences of a high-risk population in the context of an unprecedented pandemic. Qualitative results findings are published separately (under review).
Analysis
Descriptive statistics are used to summarize baseline demographic outcomes. Data is analyzed using mean (SE) for continuous variables and frequencies and percent for categorical variables. Group differences based on income and education were analyzed using analysis of variance/covariance (continuous dependent variables) and chi-square (categorical dependent variables) analyses. Income is grouped by participants with an income of less than 10,000 and 10,000 to 45,999 per year. Education is grouped by participants with a high school degree or below and greater than a high school degree including some college, no degree and trade/technical/vocational training.
Results
Sample Demographics.

Note. No significant Income*Education group differences identified.
The participants reported using the following social services: Meals on Wheels (12%), Supplemental Nutrition Assistance Program (46%), Food Commodity (19%), Local Food Program (34%), Feed More Food Pantry (47%), and RHWP (47%). The most common negative emotional state participants reported experiencing since the coronavirus disease pandemic was worry (50%), followed by sadness (44%), loneliness (42%), nervousness (41%), depression (36%), fears (34%), and loss of interest in usual activities (28%). Regarding negative emotional states, 73% of the total sample reported at least one negative emotional state. Sixteen percent of the sample endorsed all seven negative emotional states. Furthermore, impact of racial/ethnic discrimination during the COVID-pandemic was noted to impact physical health in 12% of participants; 9% reported increased exposure of contracting the coronavirus due to race; 15% felt unsafe wearing a mask or bandana; and 13% felt less safe with police or law enforcement during the coronavirus pandemic.
Epidemic Pandemic Impacts Inventory Geriatric Adaption Ranked Domains by Income and Education Analysis of Variance/Covariance.

Note. Covariate models include Age, Sex, and both Income/Education. Significant effects for COVID Infection, Social, and Positive Change Experiences. No significant Income and Education interactions identified.
Independent Income and Education item groups differences depicted in Tables 3-5.
Geriatric Adaption Social Activities and Isolation Domain
Epidemic Pandemic Impacts Inventory Geriatric Adaption Social Activities and Isolation Domain.
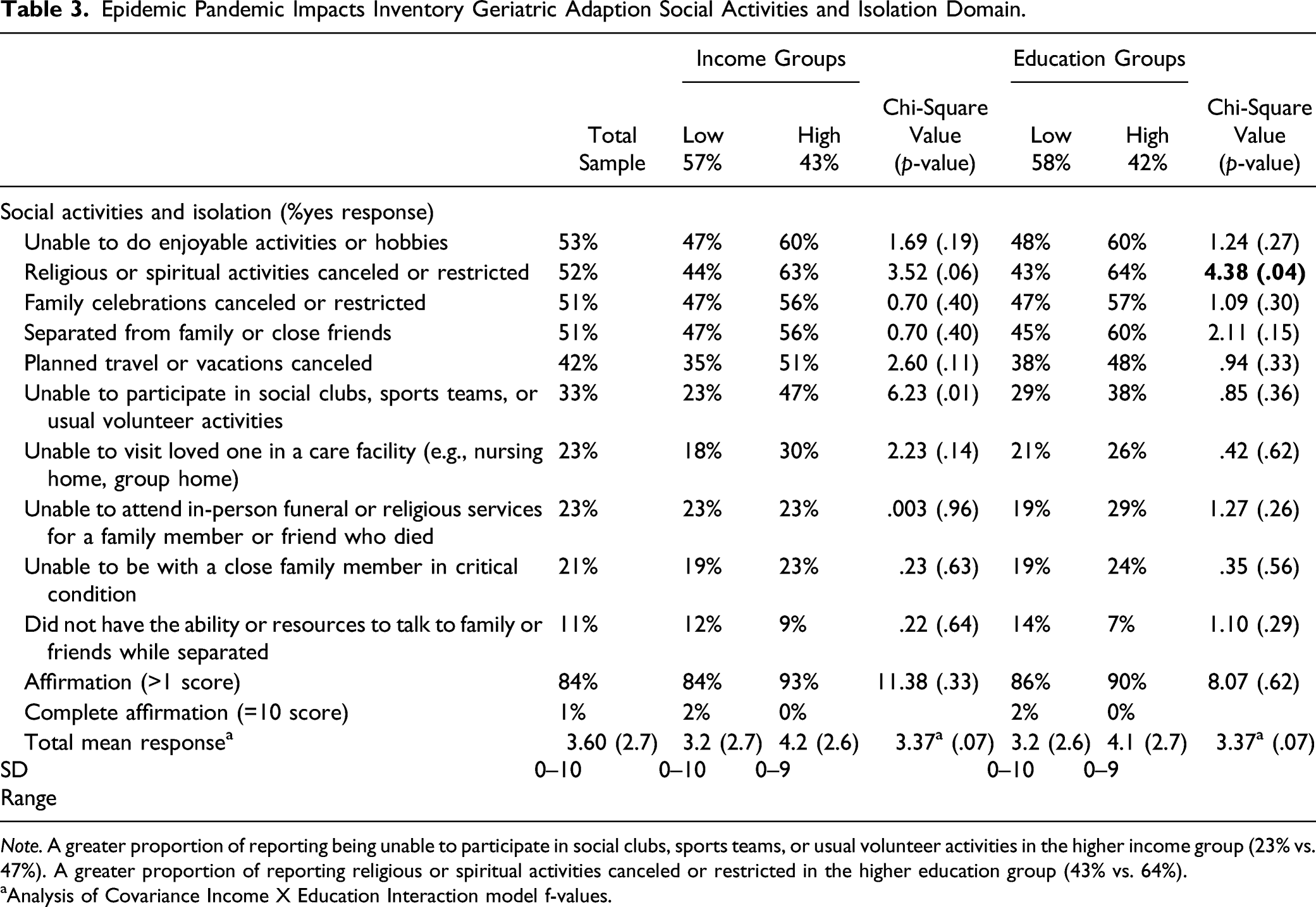
Note. A greater proportion of reporting being unable to participate in social clubs, sports teams, or usual volunteer activities in the higher income group (23% vs. 47%). A greater proportion of reporting religious or spiritual activities canceled or restricted in the higher education group (43% vs. 64%).
aAnalysis of Covariance Income X Education Interaction model f-values.
Geriatric Adaption Positive Change Domain
Epidemic Pandemic Impacts Inventory Geriatric Adaption Positive Change Domain.

Note. Total positive experience domain mean and a greater proportion of more quality time with children (11% vs. 35%) and volunteering (26% vs. 49%) in the higher income group.
aAnalysis of Covariance Income X Education Interaction model f-values.
Geriatric Adaption COVID-Infection History
Epidemic Pandemic Impacts Inventory Geriatric Adaption COVID-Infection History.

Note. Total COVID infection domain mean and a greater proportion of close family/friend deaths from COVID in the higher education group (2% vs. 12%).
Note. No significant Income*Education group differences identified.
aAnalysis of Covariance Income X Education Interaction model f-values.
Discussion
Multiple studies have highlighted the negative impact of COVID-infections on vulnerable populations. A survey of 5412 community dwelling adults across the US, conducted in June 24–30, 2020, and published by the Centers for Disease Control and Prevention, reported significantly lower percentages of anxiety disorders, depressive disorder and trauma- or stress-related disorder among participants aged 65 years or older than in younger age groups (Czeisler, et al., 2020). A cross-sectional study of 515 community dwelling adults ages 20 to 79 years, found that proactive coping was a stronger resilience factor for stress in older adults compared to younger adults (Pearman et al., 2021). A critical review on the impact of the prolonged pandemic across waves, (Manchia et al., 2022) that at least a sub-population of older adults are remarkably resilient, potentially due to their complex experiences during their previous lives. Our findings complement and broaden the understanding of this work by describing the self-reported positive change experiences of a vulnerable population of older adults. Additionally, understanding within group differences for low-income African American older adult populations helps us develop targeted and personalized interventions for the most vulnerable impoverished older adult populations.
Findings suggest that older adults with incomes less than $10,000 a year experienced fewer positive changes behaviors during the pandemic, highlighting an essential sub-population of older adults at increased risk for adverse effects. Furthermore, highlighting the diversity and heterogeneity of our sample, those in relatively higher income and education groups were more likely to experience COVID-related social consequences and death of a family/friend. These disparate findings highlight a greater loss/greater gain economic paradigm that can occur when examining equity disparities and SODH, reinforcing the need for individual and equitable community resources. Additionally, while higher income older adults may have access to technology to sustain social connectedness, low-income populations have limited access to resources to maintain connections during times of isolation thereby, increasing their risk for loneliness and depression. Regardless of group differences, our sample did report on average two instances of emotional health/well-being, physical health, and emotional health problems. On average, three social COVID-related negative consequences were reported, with the greatest experience being an average of seven negative consequences. However, it is encouraging to note that a substantive majority of participants in both income and education groups reported positive change behaviors due to the pandemic.
The cross-sectional nature of the study does not allow for drawing any causal conclusions about the relationship between SODH and well-being overtime. Given the rapid onset of the pandemic, we were unable to measure positive change behaviors and mental health functioning before the lock-down and social restrictions. In addition, given the sample was collected from older adults for whom most are already participating in a care-navigation and support services program (RHWP), selection bias may be of concern. To address selection bias, we expanded our recruitment to areas of the city that do not receive services from the RHWP care coordination program. Our results from the qualitative arm of the study are published separately and are crucial for understanding the contextual factors for variables such as positive change behaviors and socioeconomic factors found in this study. Despite these limitations, this pilot study adds to the literature by comprehensively exploring everyday challenges and positive change behaviors and highlights differences of vulnerability by examining within group differences in socioeconomic and education factors as critical for health and well-being for a low-income older adult population.
Conclusion
The pandemic has highlighted factors of resilience with participants reporting positive change behaviors to maintain physical and mental health. Findings also point to the fact that while some groups experienced resiliency with positive behavior changes in their lives, the lowest income group did not. It is possible that adversity experiences may also provide opportunities to develop adaptive strategies that foster resilience. Intervention efforts should consider leveraging such adapted behaviors to reduce the many negative pandemic impacts. Complementary to our qualitative findings, we also found that the challenges our participants faced, while exacerbated by the pandemic, were not new. Together these findings highlight the complexities of the social and political environment, beyond just that of the pandemic, that impacted personal and environmental resources and the complex adaptive systems that effect vulnerable populations (Coe et al., 2018). Future research should focus on collaborating with low-income older adult communities to understand coping and resilience factors used to improve health and well-being. This understanding will help improve care coordination and targeted support services for the most vulnerable populations.
Footnotes
Declaration Of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Virginia Commonwealth University COVID-19 Rapid Research Funding and the Virginia Commonwealth University Institute for Inclusion, Inquiry and Innovation.