
Abstract
Alzheimer’s Disease and related dementias affect 3.4 million community-dwelling adults in the United States. Given the burden of disease, a greater understanding of modifiable risk factors is crucial for targeted public health strategies. Social determinants of health (SDOH) are modifiable risk factors categorized in five domains: economic status, education, healthcare access, environment, and community context. Although individual SDOH have been linked to dementia, limited research exists on the interaction of SDOH with dementia across multiple domains. The aim of this study was to evaluate the association between SDOH across all five domains and dementia among community-dwelling adults in the United States. A cross-sectional study was performed on community-dwelling adults aged ≥65 years from the 2019 National Health Interview Survey (NHIS). Respondents (N = 9,277), of whom 303 (4%) self-reported positive dementia diagnosis, were predominantly female (55%), white (76%), and non-Hispanic (91%). Residing in a non-metropolitan area, having a usual place for healthcare, and receiving annual eye or dental exams were negatively associated with dementia. Minority compared to white status was not significantly associated with dementia, suggesting underdiagnosis of dementia within minority groups in the NHIS. We present the first comprehensive national view of SDOH among community-dwelling dementia patients in the United States.
Introduction
Alzheimer’s Disease and related dementias affect 5 million adults 65 years and older in the United States (Matthews et al., 2019). Of these patients, 3.4 million are characterized as community-dwelling, defined as residing outside of an institutionalized home (Chi et al., 2019). Dementia is characterized by cognitive decline resulting in impairment of independent function, placing a heavy burden on patients, caregivers, and healthcare providers (Duong et al., 2017; Majoka & Schimming, 2021). In 2015, an estimated 5.7 million informal caregivers provided unpaid care for older adults with dementia (Chi et al., 2019). The United States health care system spends $594 billion on dementia-related expenditures, which is projected to rise to 11% of all health spending in 2050 as the population ages (Pedroza et al., 2022). Given projected healthcare costs and the burden of disease, global research has focused on identifying and assessing modifiable risk factors to reduce the onset or prevalence of dementia (Majoka & Schimming, 2021).
Lifestyle interventions targeting modifiable risk factors are being evaluated for their impact on reducing the onset of dementia (Röhr et al., 2022). The 2020 Lancelet Commission found that 40% of all dementia cases could be prevented through addressing 12 modifiable risk factors, including physical activity, depression, and smoking (Livingston et al., 2020). Multicomponent interventions targeting factors such as diet and physical exercise have been found to improve cognition in older adults with high dementia risk or mild cognitive impairment (Ngandu et al., 2015; Yang et al., 2022).
Social determinants of health (SDOH), sometimes referred to as health-related social risks, have been shown to heavily influence lifestyle choices, which in turn shape individual dementia risk (Cockerham, 2021). These social determinants are the environmental conditions in which people are born, live, learn, work, play, worship, and age. The U.S. Department of Health and Health Services defines five categories of SDOH: economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and social and community context (Braveman et al., 2011). Previous research has linked individual social determinants of health with dementia, although few studies identify and evaluate such factors (e.g., education) as SDOH (Chi et al., 2019; Majoka & Schimming, 2021). There is also a lack of literature on the interaction of multiple SDOH across all five domains in the context of dementia risk (Majoka & Schimming, 2021). This study is the first to provide a comprehensive national view for various SDOH and their interactions among community-dwelling dementia patients in the United States.
Thus, the aim of this study is to evaluate the cross-sectional correlates of modifiable factors representative of all five domains of the social determinants of health with dementia in U.S. patients over the age of 65. Improved understanding of the relationship between SDOH and dementia will promote identification of vulnerable populations and enable better informed public health strategies.
Methods
The National Health Interview Survey (NHIS) is a nationally representative household interview survey of the U.S. civilian noninstitutionalized population. The survey has been administered annually since 1957 by the National Center for Health Statistics’ (NCIS) under the Centers for Disease Control and Prevention for the purpose of providing health, geographic, and social demographic information of the U.S. population. In 2019, the survey was redesigned for the first time in 22 years to improve coverage of health topics, reduce respondent burden, and incorporate advances in survey methodology. Questions were divided into four categories: annual core, rotating core, sponsored content, and emerging content. Content included in the NHIS every year is identified as part of the annual core, while questions in the rotating core appear on a periodic basic at a minimum of once every 3 years. Sponsored content is included when funding by agencies is provided and contributed to topics such as food security, food program and participation, and arthritis in 2019. Emerging content is sponsored by the NCIS on emerging topics and included prescription opioid use and pain management. Data from the 2019 adult injury and episode files were obtained online from the CDC for the purpose of this study. Each sample adult, aged 18 and over, was randomly selected from a household chosen with geographically clustered sampling techniques.
The unweighted survey population was restricted by age to include 9,278 sample adults, representative of the U.S. population aged 65 and over. Face-to-face interviews were conducted by trained Census interviewers in participants’ homes. Interviews via telephone were available when requested by the survey participant. If the sample adult was unable to answer due to limited mental or physical capabilities (N = 318), an informed member of the same household was selected as a proxy to answer on the respondent’s behalf (N = 303). If a household member or relative was not available, a knowledgeable proxy was allowed to respond (N = 14). If a proxy was not available, the sample adult was excluded from the study (N = 1). Previously built statistical programs incorporating survey weights, strata, and cluster information were used calculate population estimates (National Center for Health Statistics, 2019). All methods adhered to the tenets of the Declaration of Helsinki. The de-identified NHIS data and this study were considered exempt by the Northwestern University Institutional Review Board, which stipulates that analysis of de-identified, publicly available data does not constitute human subjects research and does not require IRB review.
The outcome of interest was a self-reported diagnosis of dementia, defined by a response of “yes” to the question: “Have you EVER been told by a doctor or other health professional that you had dementia, including Alzheimer’s disease?” Survey responses were recorded as “yes,” “no,” “don’t know,” or “refused” to answer the question. Participants without a “yes” or “no” response to the question were excluded from the study. The final unweighted survey population of dementia patients included 303 survey respondents.
The Healthy People 2030 approach to the social determinants of health was used to select factors for analysis (Gómez et al., 2021). A review of available literature was performed to select survey questions most closely aligned with a social determinant of health. The five domains of SDOH were represented by survey variables as follows: economic stability (employment, poverty status, ability to pay medical bills, food insecurity), education access and quality (high school or college), healthcare access and quality (insurance, consistent point of healthcare access, visual and dental exams), neighborhood and built environment (geographic region), and social and community context (urban/rural county classification). Category-level variables, such as education, were stratified and analyzed independently. Employment was defined by having worked in the previous week. Health insurance was separated into four categories: Medicare Advantage, dual eligibility for Medicare and Medicaid, Medicare or other insurance types, and the uninsured. Poverty was determined by a < 1.00 ratio of family income to poverty threshold, based upon the poverty threshold published by the Census Bureau in 2018. Respondents self-reported if they had worried whether food would run out in the past 30 days before they had money to buy more and if they had a usual place for receiving health care services. Having received an eye or dental exam was marked “yes” if the exam occurred within the previous 12 months. Following literature review, all variables were identified as outcome, exposure, confounder, or collider variables within a causal directed acylic graph to direct modeling strategy (Figure 1) (Lipsky & Greenland, 2022).
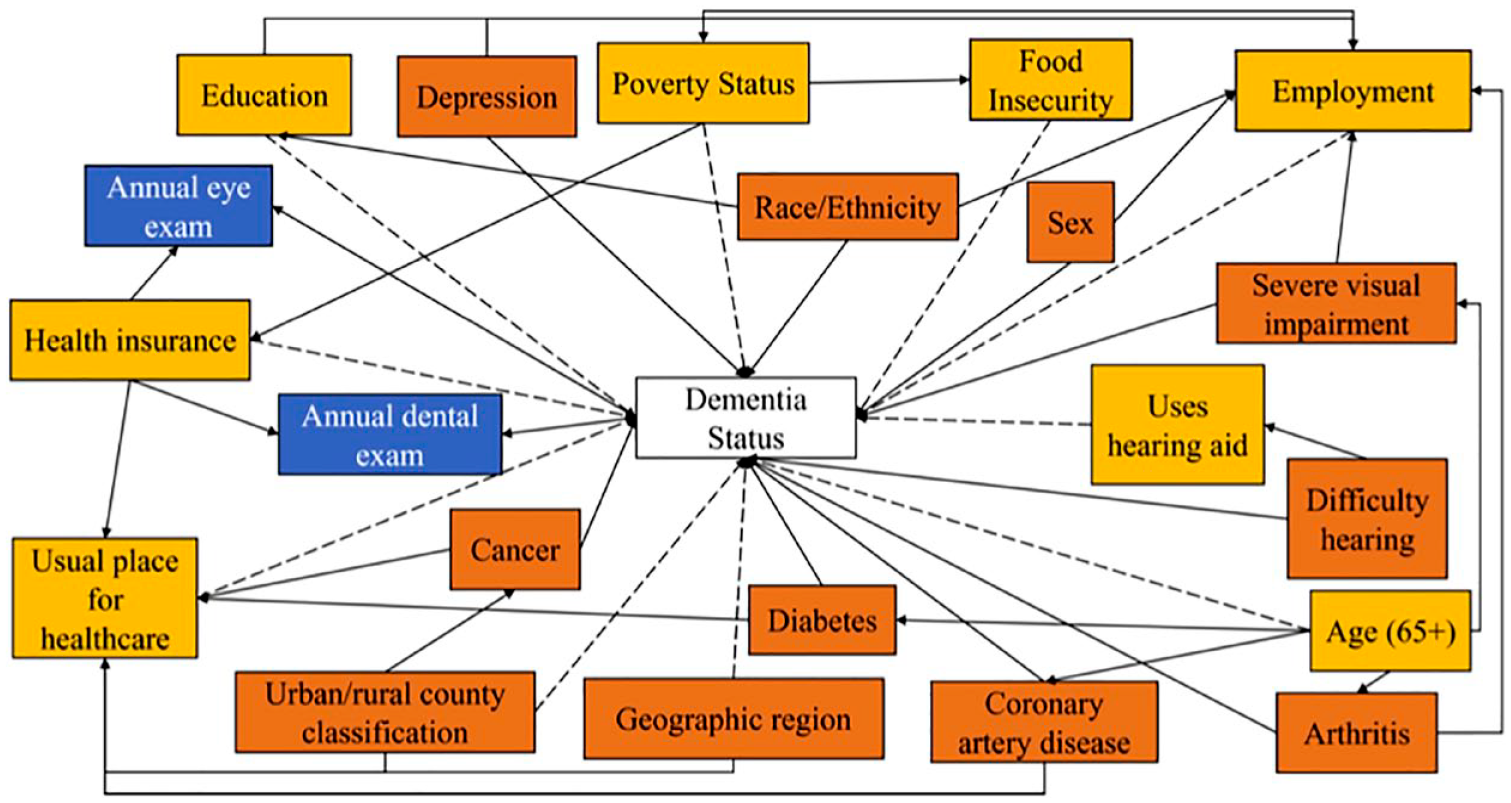
Causal directed acyclic graph representing hypothesized causal effects between study variables. The study outcome is a self-reported previous diagnosis of dementia by a health professional. Exposure, confounding, and collider variables are shown in yellow, red, and blue boxes, respectively. Dashed arrows represent hypothesized causal paths, and solid arrows represent biasing paths.
A multivariate logistic regression model was created with Statistical Analysis Software (SAS) Version 9.4, SAS Institute Inc. Cary, NC using the proc surveylogistic procedure, controlling for sex, race (white, black, Asian, Non-Hispanic American Indian or Alaskan Native, and other), ethnicity (Hispanic and non-Hispanic), and other co-morbidities (severe visual impairment, hearing difficulty, diabetes, arthritis, cancer, coronary artery disease, and depression). Odds ratios (OR) and 95% CI values were generated to quantify outcomes. Missing independent variable values were imputed using the mode when comprising of <5% of the sample. A pairwise Pearson’s Correlation analysis with a threshold of .3 was performed between independent variables to test for multicollinearity (Mukaka, 2012).
Results
The population of 9,277 survey respondents was reweighted using cluster, weight, and strata information to extrapolate the 2019 total U.S. population of adults ages 65 and older. Table 1 indicates demographic characteristics of the population diagnosed with dementia. Table 2 reveals findings from a multivariate analysis of the social determinants of health and self-reported dementia diagnosis. The multivariate logistic regression model found that dementia was inversely correlated with age, with participants aged 65 to 70 (OR 0.21; 95% CI [0.13, 0.34]) and 70 to 75 (OR 0.36; 95% CI [0.25, 0.51]) reporting lower odds of dementia compared to participants older than 75 years of age. Dementia patients were less likely to report having received some college education (OR 0.58; 95% CI [0.36, 0.92]) or minimally a bachelor’s degree (OR 0.44; 95% CI [0.26, 0.74]). Respondents living in a non-metropolitan area were inversely associated with dementia (OR 0.59; 95% CI [0.37, 0.95]). Having a usual place for healthcare was negatively associated with dementia reports (OR 0.44; 95% CI [0.24, 0.81]). Receiving an eye exam (OR 0.65; 95% CI [0.48, 0.88]) or a dental exam (OR 0.71; 95% CI [0.52, 0.96]) in the previous year was inversely associated with dementia. Minority status, employment, health insurance, geographic region, food insecurity, poverty, and use of hearing aids were not associated with dementia.
Characteristics of U.S. Adults Aged 65 and Over Stratified by Dementia Status.

Note. The study population was n = 9,277 (weighted n = 52,590,377) sample adults over the age of 65 with n = 303 (weighted n =2,086,042) dementia patients.
p < .05.
Multivariate Logistic Regression for U.S. Adults Ages 65 Years and Older.
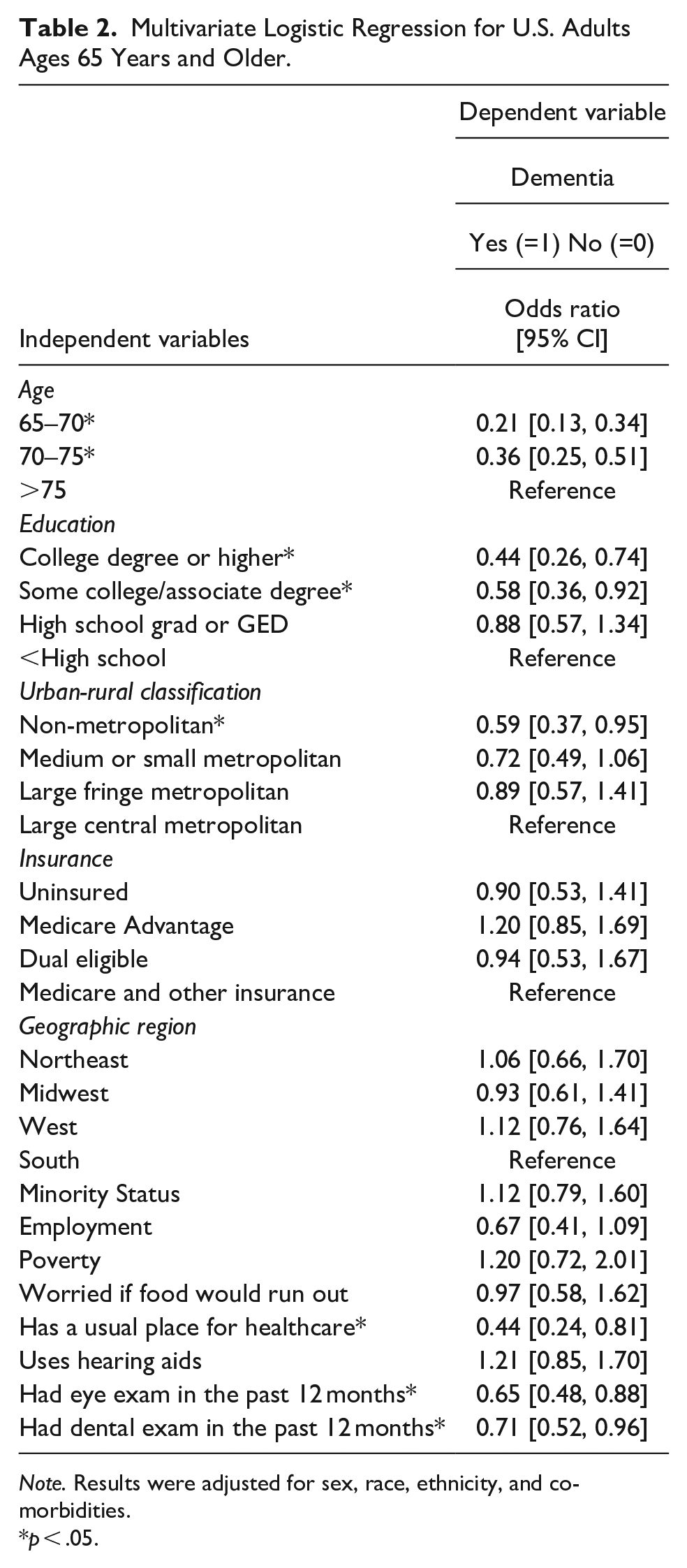
Note. Results were adjusted for sex, race, ethnicity, and co-morbidities.
p < .05.
Discussion
Our study found an inverse relationship between having a college education and self-reported dementia diagnosis. This is consistent with past literature in which higher levels of educational attainment were found to be correlated with a reduced risk of dementia (Livingston et al., 2017; Maccora et al., 2020; Xu et al., 2016). While educational attainment and income are often correlated, the variables representing poverty, employment, and food insecurity were not associated with increased dementia risk. There has been differing consensus on the importance of education in relation to socioeconomic status in the context of dementia risk (Cha et al., 2021). After accounting for poverty and food insecurity, our study suggests that education may be a greater predictor of dementia onset in comparison to wealth (Cha et al., 2021; Karp et al., 2004; Strand et al., 2015). Most importantly, minority status compared to white status was not a significant indicator of dementia. Previous literature has established a two-fold increase in the incidence of dementia among minority-status patients compared to whites (Barnes & Bennett, 2014; Lennon et al., 2022; Matthews et al., 2019). This finding points to underdiagnosis of dementia in minority populations within the NHIS.
Interestingly, we found that living in a non-metropolitan area was inversely correlated with dementia. This result differs from previous findings of increased dementia risk in rural patients. Many of these studies cited lower educational attainment and healthcare access as factors contributing to increased dementia risk in rural areas (Rhew et al., 2023; Russ et al., 2012; Weden et al., 2018). In 2012, there were only 39.8 physicians per a rural population of 100,000 patients compared to 53.3 physicians in an urban population of 100,000 patients (Hing & Hsiao, 2014). An underdiagnosis of dementia due to limited healthcare access may have contributed to findings of decreased risk in rural populations in this study (Rahman et al., 2021). Surprisingly, geographic region was not significantly associated with dementia. However, the NHIS dataset includes only community-dwelling elders. When including institutionalized elders, the South has previously been found to have the highest prevalence of dementia patients (Ailshire et al., 2022). As such, our study suggests a need for greater focus on the incidence rates of community-dwelling dementia patients, particularly in rural areas.
Another finding from our study was that healthcare insurance was not associated with dementia. Still, we found that having a consistent place to access healthcare was inversely correlated with dementia. We also found that use of hearing aids was not significantly associated with dementia. Although there is a strong link between increased hearing loss and dementia (Chern & Golub, 2019; Liang et al., 2021; Loughrey et al., 2018), limited and contradictory literature exists on the use of hearing aids and cognitive outcomes (Dawes, Cruickshanks, Fischer, et al., 2015; Dawes, Emsley et al., 2015; Hubbard et al., 2018). Health insurance reveals a patient’s financial ability to access a service but does not explicitly represent whether the patient chose to access the service. Since direct utilization indicators were significant, our results suggest that downstream factors representing utilized healthcare services are more closely associated with dementia. Furthermore, the self-report nature of the dementia variable and the impact of unrecognized dementia may have contributed to the lack of associations.
Our study found that having an eye exam in the previous year was inversely correlated with dementia, which could be attributed to potential barriers in accessing eye care faced by patients with impaired cognitive function (Vu et al., 2022). Another study found that older women with dementia were less likely to receive eye care compared to men, who tended to have younger spouses able to provide transport for eye exams and assist with treatments (Pershing et al., 2020). Similarly, the necessity of a caregiver may explain why respondents who had a dental exam in the past year were less likely to report a diagnosis of dementia. Patients with dementia often have difficulty maintaining their personal hygiene and frequently miss important dental appointments, leading to a decline in oral health (Schaper et al., 2021). Since declines in both visual impairment and dental health have been found to be bidirectionally linked with dementia (S. P. Chen et al., 2021; X. Chen et al., 2019; Lauritano et al., 2019; Schaper et al., 2021), our results highlight the importance of routine eye and dental care for elderly patients.
Our study employed a large dataset including comprehensive information on respondent’s health status, in addition to various demographic, socioeconomic, and geographic factors. Using data from a national population sample representative of the United States, our study both evaluates a comprehensive group of modifiable factors spanning all five domains of the SDOH and identifies factors most associated with self-reported dementia. Our study is the first to report associations of dementia with consistency in healthcare access, yearly eye exams, and annual dental exams in a sample of community-dwelling elders. These findings may play an important role in identifying potential target areas for future public health interventions to reduce the prevalence of dementia.
This study has several limitations. First, NHIS data consists of self-reported observations that are not confirmed by clinical diagnosis or the electronic medical record. However, self-reported measures are important because they are an accurate representation of a participant’s awareness of their diagnosis. Secondly, we referenced literature to place relevant NHIS variables in a SDOH domain. Still, there are data and interpretation limitations in aligning a theoretical SDOH framework to a national study that was not explicitly developed to investigate SDOH. Additionally, self-reported measures may lead to underreporting of dementia. While older adults with dementia may be either undiagnosed or unaware of a diagnosis of dementia, this may also be attributed to clinical shortcomings in detection and communication of diagnosis (Amjad et al., 2018). Although bias in diagnosis awareness across demographic groups is unlikely due to the national sampling strategy, the NHIS is not specifically designed to address sampling of diagnosis awareness in people groups. To address the possibility of dementia under–sampling, we are implementing the U01 (U01 NS105565-07), or the “5-Cog Paradigm to Improve Detection of Cognitive Impairment in Primary Care,” funded by the National Institute of Neurological Disorders and Stroke. Investigators at Einstein, Indiana University, and Northwestern are also collecting key information on SDOH to further inform this preliminary investigation. Our parameter estimates within this study are likely a conservative estimate, as underdiagnosis would impact effect size by lowering observation of the primary outcome (i.e., a reported diagnosis of dementia) and thus push SDOH and key covariates away from the null, decreasing the likelihood of achieving statistical significance. Nonetheless, SDOH remained statistically significant in our model, highlighting the importance of SDOH regarding dementia risk. More research is required to estimate the magnitude of SDOH effects. Finally, this study has directional links that are unable to be drawn between the independent variables and dementia risk, as all information was reported at a singular point in time. Future research should be conducted to clarify the specific mechanisms by which SDOH affect dementia risk and progression.
Conclusion
This study places in context a variety of modifiable factors representative of all five social determinant of health domains using a nationally representative population of community-dwelling U.S. elders. College education, consistency of a healthcare access point, yearly eye exams, and annual dental exams were found to be inversely associated with self-reported dementia. These results may identify areas to be targeted by future public health interventions to reduce the burden and prevalence of dementia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study resulting in this publication was assisted by a grant from the Baker Program in Undergraduate Research, which is administered by Northwestern University’s Weinberg College of Arts and Sciences (1516WCASSUM2222145). However, the conclusions, opinions, and other statements in this publication are the authors’ and not necessarily those of the sponsoring institution.