
Abstract
In Hong Kong, the number of South Asian (Indian, Pakistani, and Nepalese) older adults is projected to increase. However, academic and policy research in Hong Kong exploring the aging experience among ethnic minority older adults remains scarce. Drawing on in-depth interviews with South Asian older adults in Hong Kong, this paper examines the challenges they face in the economic, health, and social domains to maintain their quality of life in old age. Our analysis illustrates the significant cultural values, family obligations, and ethnic networks that shape the quality of life of South Asians in Hong Kong. These findings can help advance active aging policy in Hong Kong as they examine how to enhance the quality of life and facilitate social integration among ethnic minority older adults in this multicultural society.
Introduction
The demographic landscape of Hong Kong is changing significantly as both the ethnic Chinese population and ethnic minorities reach old age. In Hong Kong, 91.6% of the residents are ethnic Chinese and 8.4% are non-Chinese ethnic (Census andStatistics Department, 2022). Among non-Chinese ethnic groups, South Asians (Indian, Nepalese, and Pakistani) are the major ethnic groups (excluding foreign domestic workers from the Philippines and Indonesia). The South Asian community has an aging population (Census andStatistics Department, 2017). The proportion of adults aged 65 years or above increased from 966 in 2006 to 2,858 in 2016 for Indians, 529 in 2006 to 633 in 2016 for Pakistan, and 327 in 2006 to 713 in 2016 for Nepalese older adults (Census andStatistics Department, 2017). This recent growth in the number of older South Asian adults, combined with its expected increase in the future, highlights the importance of recognizing, revealing, and exploring the diverse and heterogeneous nature of old-age experiences and needs in this multicultural society. However, academic and policy research in Hong Kong exploring the aging experience among ethnic minority older adults—or focusing generally on issues relating to ethnicity in old age—remains scarce (Chui et al., 2020). This study emphasizes the importance of greater engagement with issues regarding ethnic minorities in aging policy studies.
The Hong Kong government first expressed its intention to develop an age-friendly environment in its 2016 Policy Address. The government subsequently invested in implementing long-term care policies and measures to facilitate aging and optimize the quality of life (QoL) for older adults in Hong Kong (Chui et al., 2020). The element of diversity is a crucial factor in the formation and implementation of an active aging policy in a multicultural society such as Hong Kong, which hosts a substantial ethnic minority population. In the aging policy, long-term social and medical care for older adults in Hong Kong is designed and implemented based mainly on the needs and experiences of ethnic Chinese (Wong & Lum, 2015). Thus, it fails to acknowledge the circumstances of those from culturally and linguistically diverse backgrounds. Chui et al. (2020) examined the long term care needs of Nepalese older adults. The lack of cultural sensitivity within public services and insufficient information prevent ethnic minority older adults from accessing the services they are entitled to as residents of Hong Kong. The South Asian community hosts diverse cultures, creating unique differences that disallow a homogenous consensus on the aging experiences of ethnic minority older adults (Victor & Zubair, 2015). Peng et al. (2003) explored how South Asians in Hong Kong perceive dementia and related help-seeking behaviors in their communities. This study adds to the current debate on the old-age experiences of ethnic minorities. It aims to examine the well-being of South Asians—Indian, Pakistani, and Nepalese—in Hong Kong, and particularly seeks to identify the challenges they face in the economic, health, and social domains in order to maintain their QoL in old age.
Active Aging and QoL Among South Asian Older Adults in Hong Kong
Active aging can be understood from four perspectives: focus, process, enabling factors, and domains (United Nations Economic Commission for Europe, 2012). First, the focus of active aging is not simply on individuals, but also on groups and populations. Second, active aging is not merely a state that may be achieved by a few people; rather, it is a continuous undertaking to improve aging trajectories. Third, enabling factors and societal structures, including personal, social, behavioral, environmental, and institutional factors, shape the aging process. Finally, active aging covers broad domains of life that are highly important for QoL, including health, economic well-being, and social relationships. In Hong Kong, the policy framework for active aging proposed by the Elderly Commission in 2006 consists of three interrelated components: (1) security of living, (2) health maintenance, and (3) social participation (Chan & Cao, 2015). These three components must be implemented together with the active participation of older adults, while the government builds a supportive environment in the form of age-friendly neighborhoods. The physical and social features of age-friendly neighborhoods are important because they recognize older adults as part of an age-integrated society. They can freely participate in community services and social gatherings to help maintain and improve their QoL (Chan & Cao, 2015). According to Chan and Cao (2015), the main feature of developing an age-friendly neighborhood in Hong Kong is the mixed use of top-down and bottom-up approaches. At the policy level, the Hong Kong government followed the guidelines of WHO and promoted its “healthy and active aging” policy. At the operational level, non-governmental and faith-based organizations have carried out several age-friendly projects focused on increasing the social participation and empowerment of older adults. These projects encourage the elderly to actively participate in the programs to increase their sense of belonging and to build a harmonious, united, and age-friendly community (World Health Organization, n.d.) The baseline assessments were conducted in different districts, mainly focusing on ethnic Chinese residents who regularly visited the District Elderly Community Centers. This approach generates one major problem. Most South Asian older adults do not regularly visit their District Elderly Community Centers. In fact, they regularly participate in activities and gatherings organized by their own ethnic community associations in different districts. Among South Asians in Hong Kong, ethnic networks play an important role in their old-age experience, which is an under-researched area in aging studies in Hong Kong.
Since migration and aging are an integral part of Hong Kong’s landscape, it seems appropriate to focus on the levels of life satisfaction and well-being among South Asian older adults in this active aging city. QoL, a crucial concept in aging research (Walker & Mollenkopf, 2007), comprises both subjective and objective elements that serve as the conditions and experience of life (Lau et al., 1998). Objective QoL can be measured by the degree to which older adults have access to and control over resources such as income, health, and social networks that help them pursue their goals and living conditions (Erikson, 1974). Conversely, subjective QoL focuses on older adults’ perceptions and evaluations: by using their own internal values and standards, people compare their subjective expectations with the objective living situation. Many scholars argue that an approach based on subjective self-assessment of QoL may provide more accurate information than objective factors in explaining variations in QoL ratings (Walker & Mollenkopf, 2007). Existing research has shown that health and social relationships are among the most important aspects of subjective QoL (Diener et al., 1998). Public policy interventions should thus lead to active participation in society. Accordingly, this study focuses on the subjective assessment of three important life domains: health, social relations, networks, and economic well-being. As suggested by Walker and Mollenkopf (2007), these domains represent the dimensions of QoL in old age that affect each other in multiple ways. Good health is a precondition for active social relationships and participation in old age. Social networks and relationships positively affect the economic well-being and health status of older adults. Hence, this study conceptualizes active aging among South Asian older adults as a process that leads to a subjective QoL in old age. This research primarily seeks to examine how the participants perceive aging care services in Hong Kong, how their family and cultural values and ethnic networks shape the caring relationships and responsibilities of older adults, and how their aspirations of return migration may affect their integration in old age.
Research Methods
The research team conducted face-to-face, semi-structured interviews with 58 South Asian participants between June 2021 and July 2022. The eligibility criteria for inclusion in the study were: (1) aged 60 years or above, (2) Indian/Pakistani/Nepalese, and (3) permanent Hong Kong residents. The research participants were identified, contacted, and selected from various non-governmental organizations (NGOs), ethnic associations, and religious bodies. The use of these institutions as a starting point was based on three considerations. First, these organizations provide diverse social and cultural services for South Asian older adults. Second, the Principal Investigator has maintained personal relationships with the leaders of the ethnic community associations for several years; therefore, he can help recruit research participants from these associations. Third, leaders of ethnic community associations can introduce older South Asian adults who are willing to be interviewed. Choosing key participants in a research project is a type of purposive sampling (Bernard, 2006, p. 191). The sample was selected on the basis of the abovementioned criteria. After obtaining informed consent from the participants, the research team first studied a purposive sample of six South Asian individuals (two Indians, two Nepalese, and two Pakistani) who were association leaders. The research team used the key research participants to locate one or two South Asian older adults in their neighborhoods through the snowball technique. Three interpreters fluent in Hindi/Urdu/Nepalese and English served as interpreters. The research team had a female Research Assistant who was mainly responsible for conducting interviews with female South Asian research participants. Ethical approval was obtained from the Research Ethics Committee (name of the university, reference number). At the beginning of the interviews, the researchers asked the participants questions related to their personal understanding of QoL, including the following: What does it mean for you to have a good life? Which component do you feel is most important for you to have a good life? Have you heard of the term “‘quality of life’?” If so, what does it imply? These questions were used to determine the participants’ familiarity with and understanding of the term QoL as well as the quality of their own lives in Hong Kong. To obtain a deeper understanding of South Asian older adults’ attitudes toward QoL, the researchers asked participants a series of questions constructed under three subcategories of QOL: physical health and psychological conditions, social relationships, and financial circumstances. In the interviews, the research team collected the participants’ views on elderly services and the function of their respective ethnic community associations in Hong Kong during the aging process. Sociodemographic information, such as personal and household characteristics, family relationships, traditional cultures and values, and return migration aspirations, was also collected during the interviews. The interviews lasted between 45 min and 1.5 hr. No incentives were provided to the participants. The interviews were recorded (with consent) and transcribed. The interview transcripts were subjected to thematic content analysis using NVIVO 12. The research team adopted three coding phases for data analysis. First, the research team read and reread the interview transcriptions line-by-line to develop abstracts and refined categories for analysis (Miles & Huberman, 1994). Second, they reread and recorded all interview transcriptions using established categories. Finally, they returned to the coded qualitative data to establish patterns for analysis after all data was coded (Lofland & Lofland, 1995). The links between the code categories address the most common challenges faced by older South Asian adults in Hong Kong. The goal was to define the relationship between the everyday problems of South Asian older adults, deterioration of well-being, and tactics to address challenges. All participants were assigned pseudonyms to protect their privacy.
Results
Of the 58 South Asian older adults, 21 were from Pakistan, 18 from Nepal, and 19 from India. Among the Pakistani research participants, 7 were male, with an average age of 71 years and 14 were female, with an average age of 65. Among the Nepalese research participants, 4 were male, with an average age of 79 years, and 14 were female, with an average age of 72. Among the Indian participants, 6 were male with an average age of 74 years and 13 were female, with an average age of 70. The participants’ profiles are presented in Table 1. Only one research participant was born locally in Hong Kong, whereas the other 57 South Asian older adults migrated and lived in Hong Kong for 7 to 66 years, living with up to nine family members. Twenty-nine live in public housing and pay an average monthly rent of $3,063 (US$393); twenty three in private housing with an average monthly rent of $8,660 (US$1,110). Six people lived in housing owned either by themselves or their children. Their homes, on average, consist of two rooms.
Characteristics of the South Asian Research Participants (N = 58).

The following sections present the results of their (1) main constituents of QoL, (2) language barriers to accessing health services, (3) role of cultural practices and family values in aging, (4) value of social networks, and (5) sense of belonging.
Family, Health and Money Are the Main Constituents of QoL
In this research, 24 people did not understand what QoL was or had never heard of the term before. The research participants were also asked what a good life meant to them, where more people chose to answer the question, and similar answers were given. In the interviews, participants listed things that were important to them for a good life. Family, health, and money were the most commonly mentioned components across all three nationalities. Thirty-two people mentioned family; 15 mentioned health, 12, money; and 6, people mentioned happiness and basic needs. Table 2 summarizes the constituents of QOL among the participants.
Constitutes of Quality of Life among the South Asian Older Adults (N = 58) N (%).
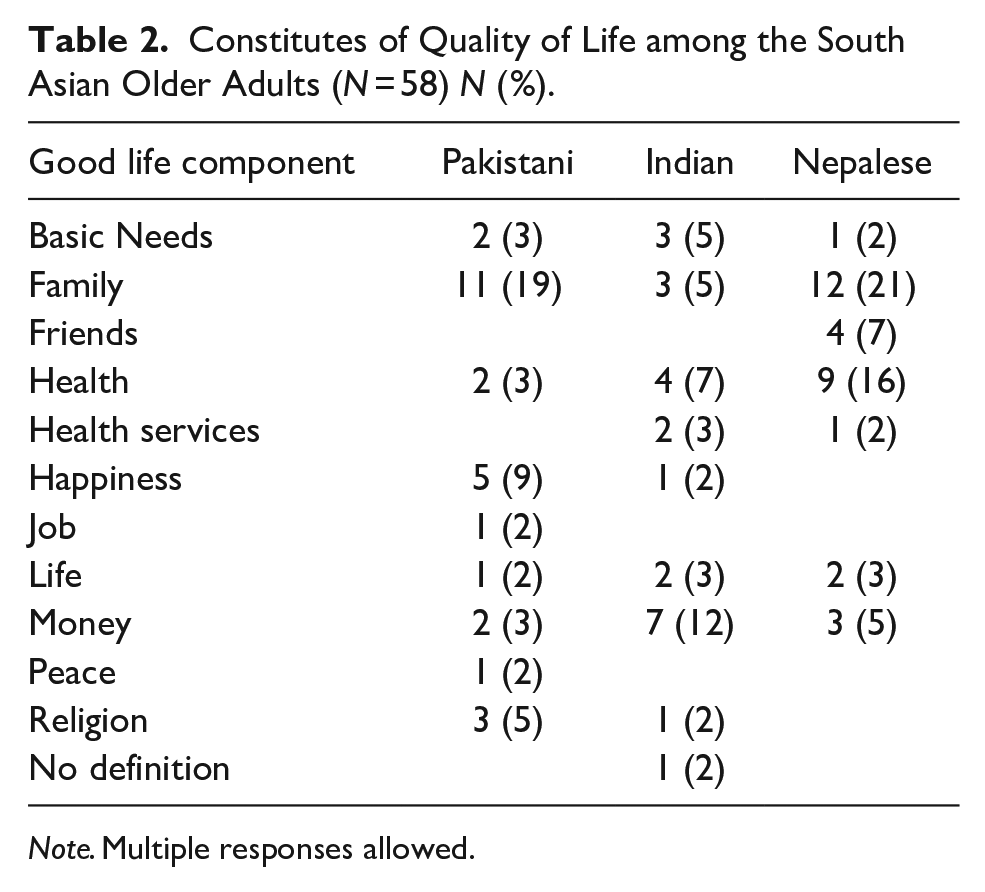
Note. Multiple responses allowed.
Family is one of the most commonly mentioned QOL components across all three nationalities. Fred is a 73-year-old Pakistani man who has been living in Hong Kong for more than 50 years. His QoL was determined by his relationships with his family. He explained, “This life is very good for me. It has been very good. I have my family my kids. It is very and I have been very blessed.” Comparing women from low-income and non-low-income families, this study found that factors such as family, health, and money showed no discernible differences between the two groups of women. Basic needs (e.g., housing, food, and enough income to sustain the household) were only mentioned in the low-income group as key to a good life. Karen, a 76-year-old Indian woman from a low-income family, defined good life as the ability to maintain her basic needs. She said, “I think that if whenever our needs are meet that’s what good life means.” Similarly, Venus, a 74-year-old Indian woman from a low-income family, explained QoL means to her: Every person has a need as long as you alive, but depends on you how much you can gain from them. Like, you know, sometimes you’re not able to fulfil your needs, so you have to be able to make yourself understand that you can’t get everything in your life. You have to limit yourself and survive with what you have.
All the participants expressed that good health was important for a good life. However, they all suffer from various health problems. Tables 3 and 4 summarize the health conditions of the participants. Hypertension, cholesterol, and arthritis were the most commonly reported health conditions among participants. Previous studies have stressed the importance of health for older adults among the various QoL domains (Seymour et al., 2008). The poor health conditions of South Asian older adults affect their everyday lives. For example, Venus is a 74-year-old Indian woman from a low-income family. She was wheelchair-bound with leg and back pains. When asked how her health affected her daily life, she said the following:
Health Conditions of South Asian Research Participants (N = 58) N (%).

Note. Multiple responses allowed.
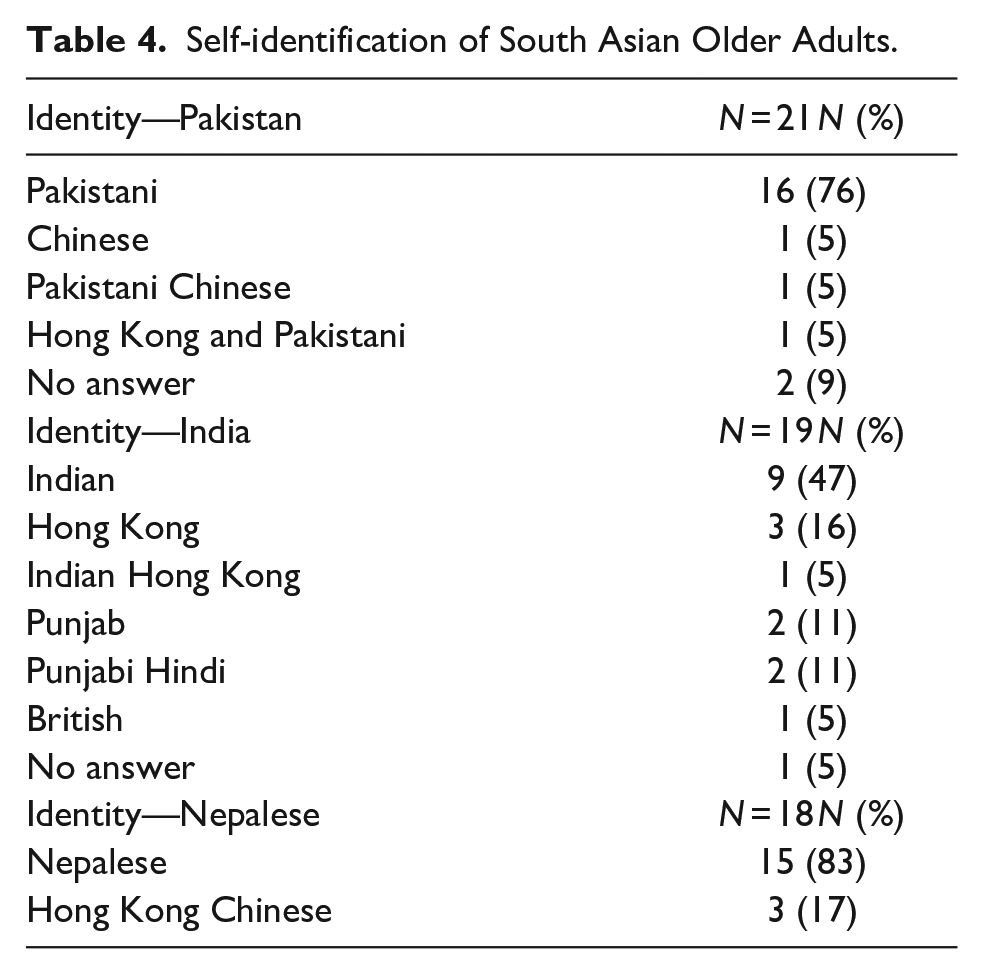
Self-identification of South Asian Older Adults.
Because I have leg problems, my nervous system has some problems with the legs. I don’t really leave my house. I try to do housework as much as I can but I have a lot of limitations because I can’t walk.
Venus’s health severely affects her QoL, as her inability to walk confines her to her house, and she rarely travels anywhere without the aid of her husband. She lives in public housing with one living area that acts as a bedroom and a living room, which is not big enough for a wheelchair to comfortably move in. She has to sit on the floor and move herself by sliding on the floor. She is trying to purchase an electric wheelchair, but currently cannot afford it. Similarly, Fathi, a 77-year-old Pakistani man, described his health as troubling. I have knee pain. I am stuck in this health problem for many years. It is not getting any better even after years of medication. I found it painful whenever I go downstairs to buy things. My son needs to work, so I have to go alone and walk slowly. The health issue is very frustrating, always on my mind for 24 hours. I don’t feel comfortable.
Money is another component of QoL. Among the research participants, 17 were receiving Comprehensive Social Security Assistance (CSSA), with an average of $5,368 (US$688) per month; five, an old-age living allowance, of $3,800 (US$487) per month; one, the Working Family Allowance of $8,000 (US$1,026) every 6 months. Full reliance on social welfare is insufficient to sustain the high cost of living in Hong Kong (fourth among 178 cities worldwide) (The Standard and Bloomberg, 2022). Older adults are unable to meet their basic needs. Large households are especially vulnerable to poverty because there may not be enough earning members to support the entire family. Karen, a 76-year-old Indian woman and her husband, also received CSSA at $4,000 (US$513) each; however, she said it was not enough to sustain both: Every time I just go to supermarket, the minimum I spend is $200 (US$26) or $300 (US$38). Even when I try to save a lot of money, fruits are expensive and our diet is really important. So, most of the time welfare is not sufficient.
Language Barrier Hinders Access to Health Services
Language barriers are a major challenge faced by older South Asian adults in Hong Kong. They all attend regular medical checkups at public hospitals. Interpretation services are available at public hospitals; however, owing to the COVID-19 pandemic, this service was temporarily suspended. In this study, most participants attended their medical appointments with a family member, usually their children or grandchildren, who could speak both English and Chinese. Only four research participants utilized the interpretation services provided by hospitals and had an interpreter accompanying them to appointments. Nora, a 67-year-old Indian woman, has eye problems. She noted that not all hospitals provide this service, which may cause problems for people with communication difficulties. She said: I requested them many times, but they told me that they are unable to provide any because, uh eye hospitals don’t provide any interpreters. So I’m not sure why they have stopped all of the sudden, but other hospitals still provide me with this service.
Ben, a 78-year-old Nepalese man, states that he is concerned about why doctors take large amounts of blood during his blood test but is unable to ask why due to the language barrier: One concern is that whenever I go for the blood test, they get so much blood that it means three to four small bottles, so I am wonder why it is necessary. Because of language problems, we could not ask anything.
A lack of communication between doctors and patients creates confusion and can lead to undiagnosed or misdiagnosed underlying medical conditions. In the interviews, many participants expressed their frustration at not being understood, and in turn, not understanding the doctor’s actions, which builds mistrust between the two and could deter them from seeking professional medical help in Hong Kong in the future.
Cultural Practices and Family Values Shape South Asians’ Aging Experiences
Cultural food practices play a role in what South Asians eat. For example, fried and oily food (such as samosas) and sweet deserts are served in most meals in the South Asian community in Hong Kong. All female participants stated that they had to use traditional cooking methods to maintain the authenticity of South Asian dishes. One Indian female older adult said, “we need to use ghee, butter, coconut, or palm oil in cooking so that the taste is good’.” Although cholesterol was a common health problem among the participants, they were not aware of the consequences of the daily intake of cooking ingredients high in saturated fat.
Facing different challenges, prayers are both psychologically and theologically important, as they relate to an improved sense of well-being, social connectedness, emotional management, and dealing effectively with anger (Spilka & Ladd, 2012). Turning to faith was essential for older South Asian adults to cope, heal, and adjust to their new surroundings, accompanied by a strong belief that God could solve their problems. Almost all Pakistanis and Indians expressed that aging does not matter, as it is a natural process that cannot be stopped and is in God’s hands. Norman, an 81-year-old Indian man, said, Basically, we think that, you know, we don’t really think about getting old a lot because, you know, if you say you won’t die ever, that’s impossible. And whenever the God needs you back, he will return you.
Another defining characteristic of South Asian culture is its values, which place importance on the family and family based systems. It is almost always assumed that adult children take care of their aging parents. They act as their parents’ translators, financial support providers, and primary caregivers, especially when their parents are new to Hong Kong. Of the 23 participants who received social welfare support, 18 received pocket money from their children. There is no set sum of financial support that their children provide; in most cases, whenever they need money, they will ask their children. Children would provide both personal and household expenses. The participants would ask for $300 (US$39) or up to $3,000 (US$385) at one time. Rebecca, a 64-year-old Indian woman, stated that it was a child’s duty to take care of their parents as they grew older: The government also has a duty but when the children are supportive why go at least they are liable to take care of their parents. As a culture also but as human being also if the children are well off why should they not take care.
When questioned about their thoughts about care homes, all participants rejected the idea of care homes and instead planned to grow old at home. In accordance with cultural norms, the concept of sending aged parents to care homes is almost nonexistent and looked down upon, with some saying it is a sin. All of them were confident that as they grew older, their children would take care of them. Nora, a 67-year-old Indian woman, said, Like, typical Chinese families in the old days, the kids will take care of them. If their kids are not, then their brother’s kids because they have big houses.
Value of Social Relations and Networks
The social relationships of all 58 participants were primarily composed of people from their own communities. Some were friends made before their migration to Hong Kong, whereas others were friends made in religious places, ethnic communities, or NGOs after their arrival. Nikki, a 75-year-old Pakistani woman, described how she made friends with Pakistani women in Hong Kong. I knew my Pakistani woman friends from the mosque nearby my house. We meet almost every day. We talk about children’s education and where to buy food at low prices. I also often invite my friends to my house. They also invite me to their houses. And then we have food and drinks and chit chat.
Most research participants have a lot of free time, as many no longer work. When not completing household chores or performing caretaking, they often seek the company of friends. Simon, a 68-year-old Pakistani man, spent time with friends: Every morning, I go to the park downstairs, sit with my friends and talk to them. There are many Pakistani men in the park talking to each other. When it is time to pray, we go to the small mosque. After praying, we go back to the park and spend time together.
While the female research participants discussed family and children when they met people from the same community every day, the male research participants talked about social issues in their home country. All participants stated that they felt relaxed when interacting with their fellow ethnic members in Hong Kong because they could speak their native languages. Nikki, a 75-year-old Pakistani woman, added “Speaking and listening to Urdu here [Hong Kong] make me feel I am in Pakistan! I have the feeling of familiarity.” Ethnic network plays an important role in their old age experience because the main channel of information in their communities was word-of-mouth, especially at the beginning of the COVID-19 pandemic.
Nevertheless, almost two-thirds of the research participants expressed that they attempted to establish social networks with Hong Kong Chinese who they met regularly in places such as wet markets and parks. Gloria, a 72-year-old Nepalese woman, described this as follows:
We meet some Chinese old people in the park every morning. We teach them to say Namaste and they teach us to say zou san (Good morning). That’s how we greet each other every morning. Although we are not real friends, it is good to have friendly relationships with the locals.
While social relationships with Hong Kong Chinese remain peaceful and friendly, they still lack the vitality and dynamics that a bond with fellow ethnic minorities could bring through an understanding and appreciation of their shared culture.
Strong Emotional Attachment to Home Country While Staying in Hong Kong
Despite problems with health care and housing, 55 participants considered Hong Kong a better place to live than their home country, as the government provides plenty of services to its residents. Ken, a 74-year-old Pakistani man commented, “I prefer to stay in Hong Kong with the benefits because in Pakistan they’re not able to get all that.” Indeed, almost all research participants had strong emotional attachments to their home country while staying in Hong Kong. They identified themselves as Indians, Pakistanis, or Nepalese. Table 4 summarizes the participants’ self-identification. Most of them explained that they would never be considered Hong Kong Chinese because “we are different, culture is different, language is different, even our skin color is different!” Ken said.
When questioned about their return migration aspirations, almost all participants preferred to stay in Hong Kong because of the presence of family and friends. As their children grow older, they transition into informal caretakers, and their decisions to stay or leave depend on their children’s migration decisions. Bonnie, a 68-year-old Nepalese woman, said that she would follow her son. She said: I have a son only in Hong Kong. So, nobody in Nepal only some relatives there, my sister and all. So, not sure. It all depends on my son because wherever he goes, I want to go there.
Discussion and Policy Implications
This study examined the constituents of QoL among older South Asian adults in Hong Kong. While prior studies in Hong Kong only explored health-related issues and challenges in accessing healthcare services (Peng et al., 2003; Vandan et al., 2019), this study examined their health, economic security, and social networks. Health, family, and money are the main constituents of QoL. Previous studies have stressed the importance of health in various QoL domains from the perspective of older adults (Seymour et al., 2008). The research participants in this study also emphasized the importance of family, specifically children and partners, and financial status as the main factors contributing to their QoL. Family members are always seen as informal caregivers for minority older adults, especially when the family can provide them “with special resources through cultural norms which dictate strong ties among family members” (Gratton & Wilson, 1988, p. 84). The research participants relied heavily on financial and practical support from their husbands/wives and children. This was especially the case when they visited doctors in public hospitals where they needed interpretation.
Peng et al. (2003) argue that language barriers are a major hindrance for South Asian older adults in Hong Kong in accessing healthcare services. This study also found that trust among health and social service providers may prevent older adults from seeking help. South Asian older adults’ experiences have drawn attention to the cultural meaning of aging. The cultural aspect of QoL is particularly relevant because of the effects of ethnic characteristics and cultural codes on the life outcomes of ethnic minorities. Expectations, norms, and systems of meaning could stem from cultural and religious orientations, creating cultural codes that influence behaviors over the life course (Phillips et al., 2010). Specific cultural codes may require specialized attention in public policy to understand the protective factors that support this group (Ciobanu et al., 2017). Similar to previous studies in different societies (e.g., Chappell, 2007), this study found that culture and religion play an important role in South Asian older adults’ perceptions of aging and growing old, and how they find comfort. Religion significantly shapes their perspectives toward aging. It is believed that aging does not matter, as it is a natural process that cannot be stopped and is in God’s hands, a belief mostly shared among Pakistanis and Indians.
In Hong Kong, many older adults live in elderly homes. However, all participants rejected the idea of a care home and instead planned to grow old at home. In accordance with cultural norms, the concept of sending aged parents to care homes is almost nonexistent and looked down upon, with some saying it is a sin. When asked who would take care of them, their replies were their children. Family values significantly influence perceptions and aspirations for the future. Most participants had strong emotional attachments to their home country. They remained in Hong Kong because their children and/or grandchildren had families in the host society. Confident and secure knowledge of their children’s care and aid alleviated their worries about the future. Our results are consistent with those of previous studies on QoL in old age. Bowling (1995) found that family relationships and health are the main dimensions of QoL from an individual’s perspective.
If QoL is to be used as a measure to dictate active aging policy development, it is crucial to utilize the voices of older adults to understand the physical and social structures of their lives (Shin, 2014). In this study, older South Asian adults in Hong Kong were negatively affected by language barriers and financial difficulties. Family obligations, religious beliefs, and cultural perspectives play important roles in older adults’ experiences in Hong Kong. While the Hong Kong government recognizes the cultural diversity of the society (Hong Kong Government, 2017), the current active aging policy endorsed by the government in 2006 ignores the ethnic dimension of social inequality among older adults. This study suggests the following four strategies for fostering the development of an active multicultural aging policy in Hong Kong.
Establishment of Language and Cultural Interpreter Training Schemes
Although the Hong Kong Hospital Authority provides interpretation services to ethnic minorities, the accessibility of such services is unreliable. Based on foreign examples such as Australia and the United Kingdom, an accreditation system for interpreters in the main ethnic minority languages should be established by collaborating with academic institutions in Hong Kong. A holistic review of current service provisions should be conducted among all stakeholders, including key ethnic minority groups, social workers, existing interpreters, frontline officers in various government departments, and frontline medical practitioners. The Hong Kong government should ensure the quality of interpretation services by offering professional certification, which includes training on communication skills, interpretation competence, professionalism, and the use of terminology in public services. An accreditation system officially recognized by the government might enhance the professional image of minority language interpreters, thereby attracting more young people from key ethnic groups to become community language interpreters. Interpreters’ codes of ethics (Australian Institute of Interpreters and Translators, 2012) and complaints, and appeal mechanisms should be established. The authorities should also establish a review mechanism to collect comments and recommendations from relevant stakeholders to maintain and improve interpretation services in the long run.
Strengthening Medical Outreach Services to Ethnic Minority Older Adults
In this study, many older South Asian adults were unaware of their deteriorating health. To enhance early diagnosis and management, a holistic care service for older South Asian adults in their neighborhoods is recommended. Medical outreach services allow medical practitioners to gain a better understanding of the living environments of older South Asian adults and facilitate communication with their caregivers. This information is important for patient treatment. As their social relationships are largely composed of people from their own communities, the authorities should collaborate with ethnic community associations, religious bodies, and NGOs in arranging medical outreach services for South Asian older adults in different neighborhoods.
The Social Welfare Department of the Hong Kong government commissioned three NGOs to establish three outreach teams for ethnic minorities to proactively reach out to those in need of mainstream welfare services. To further utilize the functions of these outreach teams, the design and implementation of outreach medical programs should involve family members (in particular, the family caregivers) to understand the caregivers’ needs and concerns in providing care for their aging parents. Family caregiving is a part of active aging, as it allows older adults to age in their homes, alleviating the burden of residential services. If the government aims to adopt an active aging strategy regarding care for its older adult population, it must provide assistance to families who do not have sufficient resources to do so (Equal Opportunities Commission, 2020). Outreach teams should also establish good working relationships with ethnic community leaders and language and cultural interpreters, as well as recruit volunteers from minority communities in the information dissemination process. Most importantly, outreach teams should ensure that the program is located (if home visits are not possible) in ethnic neighborhoods where minority older adults can easily access and congregate.
Promoting Ethnic Minority Older Adults in Social Enterprises
The government should strengthen the promotion of social enterprise funding support in South Asian communities, making leaders of ethnic community associations aware of the funding scheme that can help older adults set up social enterprises to sell their handmade products, such as arts and crafts. Improving coordination among public entities at different levels during project implementation and providing basic business skills training in collaboration with NGOs is a key step toward empowering older adults from ethnic minorities in social enterprises. Active aging highlights the importance of lifelong learning. By promoting older adults from ethnic minorities in social enterprises, this arrangement economically empowers older adults and enhances their social relationships with different people in Hong Kong.
Promoting Ethnic Minority Neighborhood Support Scheme
In South Asian culture, care homes are not acceptable to older adults. Another alternative to care homes is a neighborhood support scheme in which friends or ethnic minorities can live together in a flat and support one another with occasional care visits. This can be in the form of non-subdivided senior housing, where an entire building is for older adults and is staffed with services such as a small clinic, a food hall, and prayer rooms. This allows South Asian older adults to gain independence while receiving support from their own people and professionals. Housing is a major social issue in Hong Kong. Many participants attributed their well-being and happiness to their housing conditions. In South Asian culture, adult children are expected to care for their aging parents and share the same accommodation. However, this might be difficult to achieve in Hong Kong. To support aging in place, when applying for public housing, larger families or older adults of South Asia have the option of being given housing near each other, whether it is flat next to each other, on different floors of the same building, or even adjacent buildings. This allows them to be close to people who can take care of them and ask for help if needed.
Limitations
This study has some limitations. First, the findings did not show gender differences in their old age experiences. For instance, for cultural and religious reasons, South Asian female older adults may spend most of their time at home, which may negatively impact their physical and psychological conditions. Future quantitative studies should be conducted on sex-based differences in health conditions. Additionally, the study only recruited research participants who had existing positive relationships with NGOs, ethnic associations, and religious organizations, thus possibly excluding other South Asian older adults who were relatively more homebound, with more severe problems. Finally, family caregivers were not interviewed; therefore, the discussion lacked a family perspective. Future research should focus on the needs and concerns of adult children when providing care for their aging parents.
Conclusion
This study highlights the significance of changes in old age and familial care preferences among South Asian older adults. The general consensus is that the aging process is natural and inevitable, and there is no need to worry about it. Children take care of them at home as they grow older and they reject the idea of living in care homes. All participants who had visited public hospitals emphasized the language barrier in accessing health services. Ethnic networks play a facilitating role in maintaining and improving the QoL among South Asian older adults. The accounts of South Asian older adults in this research clearly demonstrate that this group of marginalized populations experienced different everyday life challenges in old age. This research also highlights policy recommendations in the domains of health maintenance, security of living, and social participation that aim to foster the development of a multicultural active-aging policy in Hong Kong. As families play an important role in the aging experiences of South Asian older adults in Hong Kong, further research should be conducted on the needs and concerns of adult children in providing care for aging parents.
Footnotes
Acknowledgements
The author thanks Jamie Liu for her research assistance and the constructive comments from the reviewers on previous draft.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research (Project Number: 2020.B16.003.20D) was funded by the Public Policy Research Funding Scheme of The Government of the Hong Kong Special Administrative Region. The author would like to thank the Public and Social Policy Research Centre of Hong Kong Metropolitan University, which had been established and supported by a grant from the Research Grants Council of the Hong Kong Special Administrative Region, China (Project Reference No. UGC/IDS16/18), for its support.
Ethical Approval
This study was approved by the Research Ethics Committee (REC) of Hong Kong Metropolitan University (HE-OT2020/02).