
Abstract
Tele-rehabilitation (TR) can limit physical contact in older patients if long transportation times or physical attendance challenges their health. Digital literacy decreases with age, which might interfere with geriatric patients’ ability to benefit from TR. The purpose was to describe the TR intervention, adherence to training sessions, and level of digital literacy. TR via videoconferencing was delivered both individually and in groups where more were challenged by joining training outside their homes. Improvements in functional capacity were found. Combining individual and group exercises, high adherence to the TR programme was achieved. Digital literacy was on par with younger adult computer users. Individual-and group TR sessions might secure high adherence to the exercise programme. Digital literacy at a certain level might be a prerequisite when supplied with both oral and written material Suggestions on how to raise older people’s digital literacy to use telehealth solutions in the future are provided.
Introduction
More and more countries are demanding that their citizens use digital solutions (Digital Nations, 2020). This also applies to older people, who have to acquire digital skills in their adult lives (Wang et al., 2013). Coping with the increasing use of digitalisation in society and diminishing physical activity are challenging in older people’s everyday lives.
Physical Activity
Impaired physical activity affects the functional capacity of frail older people. Regular weekly training sessions can deter the negative spiral, yield safer walking capabilities and thus prevent falls (Campbell & Robertson, 2007).
Tele-Rehabilitation
Tele-rehabilitation (TR) can effectively prevent loss of functional capacity (Hansen et al., 2020) but TR is often a plan B for older people who wish to avoid exhaustion and prefer exercising at home (Franco et al., 2015). For others, social distancing may be a condition, as seen during the ongoing coronavirus pandemic (Taylor et al., 2021).
Tele-Rehabilitation Via Videoconferencing
TR performed in groups via video-conferencing approximates the face-to-face supervision that occurs when patients receive conventional training in groups at a training centre (Hansen et al., 2020). However, conducting TR with geriatric inpatients was not feasible (Jørgensen et al., 2021) but TR is often successfully used in patients with many different diagnoses (Hansen et al., 2020; Hwang et al., 2017; Scherrenberg et al., 2020). What distinguishes these groups from geriatric inpatients is that they are often younger and likely more digitally literate.
Objectives
The purpose of this study was to describe the TR intervention, the pedagogical initiative needed, adherence to the TR intervention and the level of digital literacy.
Cases
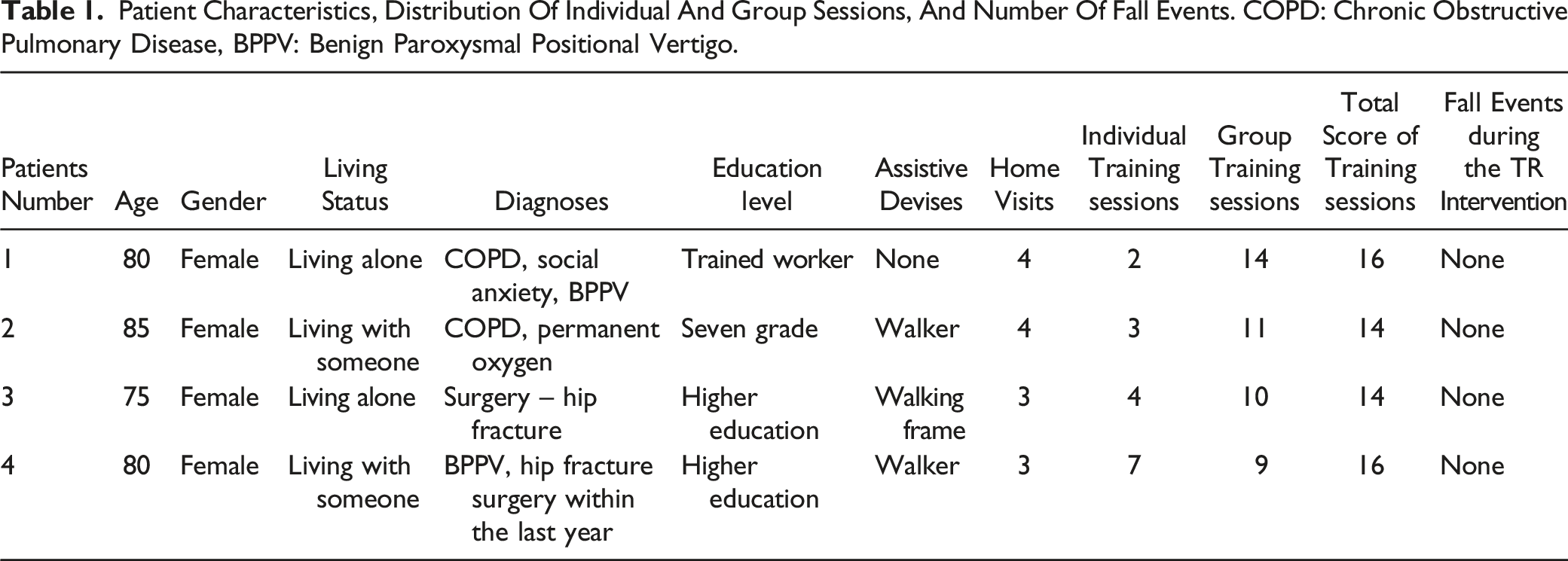
Patient Characteristics, Distribution Of Individual And Group Sessions, And Number Of Fall Events. COPD: Chronic Obstructive Pulmonary Disease, BPPV: Benign Paroxysmal Positional Vertigo.
TR Intervention
The patients were offered TR via a real-time video-conferencing system for 8 weeks, resulting in a total of 16 TR sessions possible. We used the Otago Exercise Program (OEP) which can be performed by leaning on a chair or without support (Campbell & Robertson, 2007). We strived to conduct the group TR with three people, but also accepted pairs of two.
The patients were placed in their own home. The physiotherapist at the hospital. The videoconferencing system made it possible for all involved to communicate and see each other during sessions. All used a 21-inch screen, external webcam, and microphone/loudspeaker. Supervised TR was planned for the first 4 weeks, and for the next 4 weeks, the TR intervention was planned to be performed via video-taped OEP still conducted as group-based exercises, but because of technical issues we continued the supervised TR for the following 4 weeks. Periods in which the participants were unable to participate in the group TR intervention were compensated with individual training sessions, if possible.
Outcomes: The patients were scored at baseline and again after the 8-week training period. The Functional Recovery Score (FRS) (Zuckerman et al., 2000) the De Morton Mobility Index (DEMMI) (de Morton et al., 2013), the Falls Efficacy Scale-International (FES-I) (Yardley et al., 2005) were used, and the digital part of the eHealth Literacy Assessment Toolkit (eHLA) questionnaire at baseline (Karnoe et al., 2018). All total scores were presented separately. For the eHLA questionnaire an individually and overall mean score was found by first adding the scores within each item and then dividing the number of questions within each item. We registered adherence to the intervention through attendance during the TR sessions, group-based or individual TR, as well as the number of falls.
Functional Assessment, Fear Of Falling And Digital Literacy
Scores in FRS, DEMMI, FES-I and eHLA.

FRS: Functional Recovery Score (max. 100 points), DEMMI: The De Mortons Mobility Index (max. 100 points), FES-I: Falls Efficacy Scale-International (max 64 points), eHLA: eHealth literacy assessment toolkit-digital part, *8-weeks' follow-up.
Therapeutic Intervention And Pedagogical Initiatives
For Patient 3, who had surgery for a hip fracture, the video-conferencing system was installed in her kitchen, and a kind of parallel bars were established between two tables. All patients were instructed on the computer’s use and received a very detailed written guide with step-by-step picture illustrations.
We quickly learned that retaining patients at pre-planned times in the TR intervention was difficult. Patients had to cancel the TR appointment due to private arrangements or examination- and/or treatment appointments at the hospital. This resulted in a more flexible approach with individual and group TR interventions to avoid losing too many TR sessions.
Therefore, after adding the number of individual- and group TR sessions, we came close to 16 possible sessions during the 8 weeks' intervention (Table 1). Home visits were primarily used to install the technical devices, introduce the patients to the computer, the TR application and the OEP.
Discussion and Conclusion
This case report shows that it was possible to perform a TR intervention among a non-randomised group of older geriatric patients. Continuously, we optimised our written material with accompanying images based on feedback from the patients. This case report does not directly investigate whether this enhancement of the written material improved their digital literacy through continual practice and influenced their willingness to participate. This target group has more competing diseases; it is unknown whether making the training appointments as flexible as possible by combining individual- and group interventions during the 8 weeks' intervention might have affected adherence to the TR programme. However, this flexible approach might be challenging for the physiotherapist and may not be realistic to fully implement in their often-packed work programme.
Digital literacy at a certain level might be a prerequisite if TR or other telehealth solutions are to be implemented in this population of very old people. Therefore, it is necessary to make suggestions on how to improve older people’s digital literacy both now in the ongoing COVID-19 pandemic and in the future (Doraiswamy et al., 2020).
A limitation of this study was that all four patients were women. Unfortunately, it was not possible to recruit men, and this could possibly have changed the results. Future TR studies involving both sexes are needed. Do men require different pedagogic initiatives than do women? The fact that there were no reference values concerning the eHLA questionnaire combined with the small number of patients in our study compared to other studies should be taken with caution. This study could appropriately have been followed up with interviews of the patients, focusing on the experiences they have gained.
In conclusion, this case report showed that TR, both individually and in groups, is successful at a certain level of digital literacy when they are aided by both oral and written material. Furthermore, a certain level of flexibility, might ensure greater adherence to the TR programme. The TR experiences described in this case report should be able to be generalized to other geriatric patients in need for physical exercises but where physical presence challenges them.
Footnotes
Acknowledgments
The authors will like to thank all who has made this case report possible including patients and the staff involved at the rehabilitation centre Vikaer Garden, Municipality of Aarhus, and in the Fall Clinic at Aarhus University Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
The study was approved by the Central Denmark Region Committees on Health Research Ethics (1–10-72–394-17) and by the Danish Data Protection Agency (1–16-02–201-17) and was conducted in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Patients gave written informed consent and were informed that they could withdraw at any time. Communication between patient and therapist during the tele-rehabilitation interventions was carried out over the internet using a secure system.
Disclosures
The Case Report was approved by the Central Denmark Region Committees on Health Research Ethics (1–10–72–394–17) and by the Danish Data Protection Agency (1–16–02–201-17). The patients gave written informed consent and were informed that they could withdraw at any time. Communication via videoconferencing was carried out over the internet using a secure system.