
Abstract
Summary Statement of Implications for Practice
This study advances the understanding of the current landscape of efforts in developing dementia-friendly and inclusive communities
Planning and Implementing dementia-friendly and inclusive interventions require direct involvement of people with dementia
The findings highlight the need of using theories to inform strategy development and implementation
Introduction
The number of people with dementia is projected to reach 82 million by 2030 and 152 million by 2050 (World Health Organization [WHO], 2020). The World Health Organization (WHO) has declared dementia as a public health priority (WHO, 2020), and has called for global action to establish dementia-friendly initiatives. It is widely recognized that people with dementia and their informal caregivers face significant challenges that include stigma, social exclusion, and difficulty accessing local support resources. The recent COVID-19 pandemic has impacted people across the world, further challenging people with dementia and their informal caregivers. The concept of inclusive dementia-friendly communities has potential to promote social inclusion, change attitudes and behaviors, and support people with dementia to live in their community in meaningful ways, and examples are increasingly evident in countries around the world.
Dementia-Friendly and Inclusive Community, Social Inclusion
An inclusive dementia-friendly community can be defined as a place where people with dementia can be understood, respected, supported, and feel confident about being able to contribute to the community (Wu et al., 2019). Social inclusion refers to a dynamic process where people engage with, and are part of, their social networks in the community to maintain meaningful social relations (Wiersma & Denton, 2016). Social inclusion refers to characteristics of (a) social integration, (b) social support, and (c) access to resources (Newman et al., 2019). Raising awareness and education across all societal sectors helps to minimize stigma and enable social acceptance. Social connection and a sense of belonging are essential to well-being and quality of life. Purposeful connection, engaging in meaningful activities with other people, are important to a person with dementia and their families/care providers (Phinney et al., 2016). People with dementia can benefit from their local community network; social inclusion and social participation promote a sense of social citizenship, safety, and contribution (Wiersma, 2008). Considering that stigma and social exclusion are important issues for people with dementia living in the community, interventions that engage and include people with dementia in their community activities would seem vital to help support people with dementia and to assist them to remain living in their personal residential house or as long as possible.
The notion of dementia-friendly community has been drawn from the Age-Friendly Cities initiative of the World Health Organization (Ogilvie & Eggleton, 2016). Age-friendly communities involve bringing stakeholders together to help create inclusive environments in local communities in order to promote active and healthy aging (Hebert & Scales, 2019). Age-friendly communities contribute to good health and allow people to continue to participate fully in society (Webster, 2016). A similar guiding principle that dementia-friendly and age-friendly strategies both embody is empowering local stakeholders to collaborate and contribute to social inclusion. Public education, reduction of stigma, and removal of barriers in physical and social environments are common themes in both age-friendly and dementia-friendly initiatives (Phillipson et al., 2019).
With the development of inclusive dementia-friendly communities that have the potential to empower people with dementia, it is important to better understand what strategies make dementia-friendly and inclusive communities effective (Heward et al., 2017; Phillipson et al., 2016). There has been a shift toward using an asset-based approach to include the voices of people with dementia in building dementia-friendly communities (Rahman & Swaffer, 2018). “Nothing about us without us” is a phrase borrowed from the disability movement which has been frequently expressed by people with dementia in public campaigns (Wolfe, 2017). However, to date, robust knowledge about inclusive dementia-friendly communities remains limited. This scoping review aims to identify current evidence about strategies being used to create inclusive dementia-friendly communities (DFC) that support social inclusion.
Methods
Scoping reviews are useful to systematically map and synthesize the current state of evidence when a research topic is new and has not been fully established (Peters et al., 2015). The study question that guided this review was: What are the strategies used for developing inclusive dementia-friendly communities to improve social inclusion? This scoping review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology for scoping reviews (Peters et al., 2015), which involved a three-step search approach: (1) identifying keywords from the initial broad search of two databases CINAHL and AgeLine; (2) conducting a second search using all identified keywords and index terms across seven databases (CINAHL, AgeLine, MEDLINE, PsycINFO, Web of Science, ProQuest and Google); and (3) hand-searching the reference lists of all included articles and reports for additional studies. Our project team consisted of patient partners (n = 3) and family partners (n = 4), nurse researchers (n = 2), and a student in the faculty of medicine. The search strategy included identifying published journal articles and gray literature to cover the breadth of the available research literature reporting strategies used for developing inclusive dementia-friendly communities to improve social inclusion. The study took place between April and September 2020. The inclusion and exclusion criteria are included in Table 1.
Inclusion and Exclusion Criteria.

Participants
We included studies that focused on people with dementia of all ages living at their personal residential house in the community. Studies that focused on neighbors, local citizens, public, and private service providers, informal caregivers, and families of people with dementia in the community that promoted dementia-friendly community were also included.
Concept
This review considered any and all strategies that aimed to create positive impact to improve social inclusion and social participation of people with dementia, including public education activities to change attitudes and behaviors, and thus reduce stigma in community. For example, we included articles that reported on public awareness initiatives, education and training about dementia, and development of physical environment guidelines.
Context
We included studies conducted in community, with people residing at their personal residential house. Studies in targeted formal healthcare organizations and congregate living facilities such as hospitals, assisted living, and long-term care facilities, were not considered in this review.
Search Strategy
As recommended in JBI review guidelines, we applied a three-step search strategy. The first search of MEDLINE and CINAHL involved the following keywords: dementia or Alzheimer’s, (community or communities) OR (city or cities) OR (neighborhood or neighborhood) OR (environment or environments), friendly or capable or inclusive or inclusion. In the second step, we used all keywords and index terms identified from step one to search six databases: MEDLINE, CINAHL, Ageline, PsycINFO, Web of Science, and ProQuest for thesis and dissertation. Google was also searched using phrases, such as: “dementia-friendly” OR “dementia friendly” OR “dementia-inclusive” OR “dementia inclusive” OR “dementia-capable” OR “dementia capable.” Thirdly, the reference lists of all included articles and reports were screened for additional studies.
Study Selection and Reviewing Results
A bibliographic reference management tool, Mendeley, was used to ensure that all references and articles were systematically organized. All identified relevant articles were uploaded into Mendeley and duplicates were removed. The review process involved two levels of screening: a title and abstract review followed by a full-text review. In the first level of screening, three investigators independently screened the title and abstract for relevancy. In the second level of screening, the full text of relevant articles was examined for inclusion against the inclusion criteria: (a) focusing on people living with dementia, (b) home settings, (c) strategies for creating dementia-friendly communities. A data analysis software program, NVivo12, was used to conduct coding for full-text review of selected articles to identify themes that summarized the literature and answered the review question. We included studies published in English with no time limit, including a wide range of study designs from randomized controlled trials to descriptive studies, quantitative and qualitative designs. The database search initially yielded 1,029 publications and an additional 12 publications identified through Google search. After screening, 53 articles were identified. Of these, 24 records were excluded for not being relevant to the review question. After assessment for eligibility of the 29 articles in our team discussion with patient and family partners, one study was excluded. We also found one additional relevant study in the reference list and included it in the review. The final review included a total of 29 publications (n = 29). See Figure 1 for the PRISMA flow diagram (Peters et al., 2015) that describes the review process.

PRISMA flow diagram.
Mapping
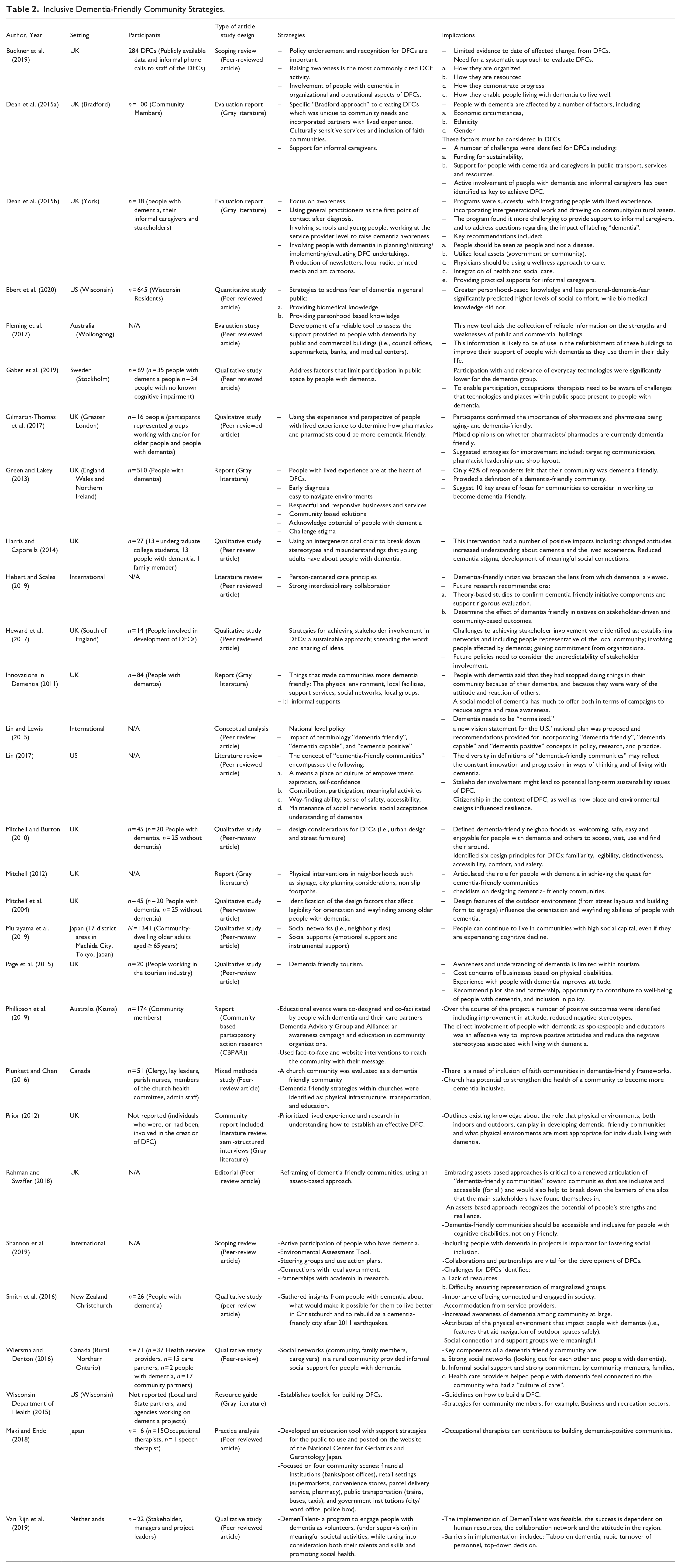
We mapped the selected articles in a summary table (see Table 2) by domains: author and country, setting, participants, strategies, and implications (lessons learned). In research meetings, the whole team including patient and family partners took part in analyzing the extracted data, sorted according to potential themes. We compared and discussed different interpretations to resolve conflicts.
Inclusive Dementia-Friendly Community Strategies.
Summarizing Results
The extracted data were collectively evaluated, refined and collated into categories to develop the final themes. Themes were validated by patient and family partners. See Table 2 for the results charted to answer the scoping review study question: strategies and impact for inclusive dementia-friendly communities.
Ethical Consideration
Research ethics approval and consent to participate was not required for this scoping review because the methodology of the study only consisted of data from articles in public domains. As a team that included academic scholars and a trainee (student in medicine) working with people living with dementia, we engaged in team reflection in our regular meetings and used the guidance of the ethical framework “ASK ME” specifically developed for co-research with people with dementia (Mann & Hung, 2019). The voices of patient and family partners enriched researchers’ understanding of the topic. The researchers and medical resident also gained skills in the project for engaging patient and family partners through developing an awareness of the different styles of communication, exploring experiential views, and lived experience perspectives.
Results
Table 2 describes the characteristics of the 29 studies that met the eligibility criteria, including strategies and impact reported. Of the 29 publications, 14 were from the United Kingdom and three were identified as multi-country. The remainder were from Canada (2), the United States (2), Japan (2), Australia (2), New Zealand (1), and the Netherlands (1). From these publications, only three followed a quantitative study design, eight followed a qualitative study design, and the remaining publications were a mix of reports, review articles or gray literature (including documents from community and government organizations. Analysis across the 29 studies yielded the following themes: Active involvement, Inclusive environmental design, Public awareness education, and Customized approach adapting to local context.
Active Involvement
Active involvement in the running and organization of dementia-friendly communities by people living with dementia and their informal caregivers was identified as a valued strategy in the development of dementia-friendly communities (Buckner et al., 2019; Dean et al., 2015a, 2015b; Ebert et al., 2020; Heward et al., 2017; Phillipson et al., 2019, p. 30). Knowledge shared by people with lived experience was identified as important within the process of designing inclusive dementia-friendly communities (DFC) interventions and was also seen as a means to instill a sense of value and autonomy for people living with dementia (Buckner et al., 2019; Dean et al., 2015b; Heward et al., 2017). Across the literature reviewed, examples of active participation included: participation in designed activities, engagement with community resources, involvement in development of educational resources/programming, delivery of educational materials, involvement on an organizational level, and promotion/advertisement of DFCs (Buckner et al., 2019; Dean et al., 2015b; Ebert et al., 2020; Heward et al., 2017; Phillipson et al., 2019). Personhood-based knowledge was specifically highlighted as beneficial in results when educating the public about dementia (Ebert et al., 2020; Phillipson et al., 2019). Involvement by people with dementia and their informal caregivers was also identified as important for sustainability of projects/organizations, as investment from community organizations was not always as consistent (Heward et al., 2017).
Active involvement was identified as a key to the success of DFCs; however, it was also recognized that within many existing DFCs, the organization had not been designed with active involvement from people with lived experience (Buckner et al., 2019; Van Rijn et al., 2019). In particular, a lack of first-person knowledge was felt to impact participation in DFCs (Dean et al., 2015b). There were a number of barriers to active involvement which were identified across the literature. Dean et al. (2015a, 2015b) conducted evaluation reports about two dementia friendly programs in the UK, primarily using qualitative interviews. Within these reports, themes of physical barriers; and socioeconomic status, gender, and ethnicity all had impacts on the individual’s active engagement in the dementia friendly communities. For example, individuals of certain ethnicities were found less likely to be referred to the program by health care providers. It was also recognized that gender and cultural experience had an impact on the way’s individuals experienced available programing, and as such influenced participation. In a 2019 scoping review, informal caregivers speaking on behalf of people with dementia and fear/concern of being negatively labeled if speaking about dementia were identified as themes which impacted involvement and prevented lived experience voices from being included in development of dementia friendly programs (Shannon et al., 2019). Increased involvement by people with lived experience was felt to improve the quality and success of DFCs.
Inclusive Environmental Design
Environmental design that considers the unique needs of people with dementia and their informal caregivers can meaningfully contribute to DFCs (Dean et al., 2015b; Fleming et al., 2017; Gaber et al., 2019; Gilmartin-Thomas et al., 2017; Prior, 2012; Shannon et al., 2019; Wiersma, 2008). A review of 284 DFC programs in England highlighted that “enabling people living with dementia to access mainstream services is where DFCs should start” (Buckner et al., 2019). It was recognized within this review that many dementia friendly communities were formed specifically due to the need for environmental adaptations to support people with dementia using community services such as churches and shops. Similarly, a practice analysis conducted with occupational and speech therapists identified that many people with dementia were significantly limited in function and engagement in community due to environmental considerations, such as street design impacting wayfinding (Maki & Endo, 2018). Environmental considerations encompassed social interactions, physical design elements, and technological considerations. Supportive staff/community members and general friendliness were identified as essential strategies to help people with dementia engage in their communities (Smith et al., 2016; Wiersma, 2008). Placement and legibility of signage, and general consideration for wayfinding needs were also highlighted as common strategies employed to support people living with dementia (Maki & Endo, 2018; Mitchell, 2012; Mitchell et al., 2004; Mitchell & Burton, 2010; Shannon et al., 2019). Accessibility was another essential consideration related to environmental design, with particular consideration for transportation and access to public transit (Fleming et al., 2017; Mitchell, 2012). In a qualitative study conducted by Gilmartin-Thomas et al. (2017) both formal and informal caregivers highlighted pharmacies as an essential location, frequently visited by people with dementia. As pharmacies were felt to be an important touchstone for people with dementia the participants felt this would be a valuable location to employ dementia-friendly strategies (Gilmartin-Thomas et al., 2017). Technology was also identified as a potential barrier for people with dementia, and the importance of low technology spaces/programs was felt to be beneficial in supporting DFCs (Gaber et al., 2019).
Public Awareness Education
Stigma and lack of public awareness were identified as significant concerns for people living with dementia. Public awareness and education were identified as an essential strategy to target stigma within the general community (Buckner et al., 2019; Harris & Caporella, 2014; Hebert & Scales, 2019). Within studies evaluating the activities of existing DFCs, education and raising awareness were identified as the most common activities performed by DFCs (Buckner et al., 2019). Specific awareness-raising strategies have included educational campaigns including pamphlets, social media presence, and memory cafes (Buckner et al., 2019; Hebert & Scales, 2019; Maki & Endo, 2018). Promotion of intergenerational relationships was also identified as a public awareness tool. A qualitative study looking at the use of intergenerational choirs found that young adults involvement in this program resulted in a positive change in attitude and reduced stigma toward dementia (Harris & Caporella, 2014). In studies that explored the delivery of educational materials, people with lived experience were seen as valuable contributors (Ebert et al., 2020; Phillipson et al., 2019).
Customized Approach Adapting to Local Context
People living with dementia belong to many different communities, with variable geographic and cultural contexts. Within this scoping review, authors recognized that DFCs should be designed with the specific needs of the local community in mind (Dean et al., 2015b; Smith et al., 2016; Van Rijn et al., 2019; Wiersma, 2008; Wiersma & Denton, 2016). There are many factors which may influence the experience of people living with dementia, including socioeconomic status, ethnicity, gender, and culture (Dean et al., 2015b). Development of DFC interventions with support from people with lived experience and varied backgrounds was highlighted as a useful strategy to address this need (Dean et al., 2015b). The geography of a DFC may also influence individual community needs; for example, a rural DFC might have different considerations compared to an urban DFC (Wiersma & Denton, 2016). Local partnerships with other community organizations were felt to be another essential strategy for the creation of sustainable DFC structures (Heward et al., 2017). Failure to value a customized approach and reliance on top-down decision making was identified as a barrier to the development of successful DFCs (Van Rijn et al., 2019).
Discussion
The goal of this study was to explore key strategies for creating inclusive dementia-friendly communities that support people with dementia and their informal caregivers. Our findings are congruent with the four dementia-friendly principles promoted by the Alzheimer Disease International (ADI, 2016): people (involvement of people living with dementia), communities (supportive physical and social environments), organization (dementia-friendly businesses and organizations), and partnerships (relationships with local governments, service agencies). Although each place (neighborhoods, cities, and countries) may have different strengths and needs with regard to their local culture, there are similar key strategies to promote social inclusion.
The direct involvement of people with dementia is a growing demand from advocacy organizations such as ADI and Alzheimer Societies across the world. More attention should be paid to structural support to enable meaningful involvement of people with dementia. When considering the promotion and development of dementia friendly communities, people with dementia should be invited into the development of strategies and technologies from early phases through to dissemination to ensure these approaches are relevant, useful, and usable.
Within the literature included in the current study, there was limited discussion around the impact of gender, ethnicity, culture, and socioeconomic status, on DFCs and the experiences of people with dementia and their caregivers. Of the studies which addressed these themes it was recognized that each had a significant impact on both individual experience and systems level functioning for DFCs. The authors of this paper recognize that these are essential factors which require careful consideration and thought as they pertain to the development and running of DFCs.
One important gap in the current efforts for inclusive dementia-friendly communities is the involvement of young informal caregivers to include their perspectives of needs and experiences. The current literature has drawn attention to educating young children and young adults and involving them in intergenerational activities; however, there were no studies specific to dementia friendly communities that highlighted voices of young informal caregivers. Although intergenerational contacts and education are crucial for creating future inclusive dementia-friendly generations, further knowledge is required to gain a better understanding of young informal caregivers’ perspectives. Young informal caregivers of parents with young-onset dementia can be children at a very young age. The first author in her clinical work has met with young children in schools, even including some under 10 years old. These children have very different needs and creative strengths compared to adults and older caregivers. In the study by Hall and Sikes (2017), young informal caregivers reported that they provide substantial levels of care, which affected their health, school education, and childhood social life.
Strengths and Limitations
This scoping review offers three contributions. First, we provide a robust synthesis of updated evidence to report 29 articles from 2004 to 2019, thus building upon a previous review (Shannon et al., 2019) of eight papers from 2011 to 2016. Second, we mapped accessible literature, including gray literature to provide a comprehensive overview of evidence to inform education, practice, policy, and research. Third, by including patient and family partners in conducting the scoping review, we ensure the relevance and quality of the study, including transparency and accountability.
Here we must also acknowledge some of the study limitations. We focus on strategies for social inclusion in this study. “Inclusive dementia-friendly” is still a new term in development and as such, it has not been consistently defined. Dementia friendliness may mean different things to different people. The results of this scoping review did not highlight a complete breadth of current dementia care approaches. For example, no studies in the review addressed the role of animal companions despite this being an area discussed in dementia literature. Also, this scoping review did not include non-English literature. It is possible that we missed important dementia-friendly interventions implemented in non-English speaking countries. Future research should investigate efforts invested in non-English speaking and developing countries.
Future Areas of Study
Future research should investigate how different theories can be applied to guide implementation and evaluation of outcomes. International research to compare findings across inclusive dementia-friendly communities will allow sharing of useful lessons for collective and individual progress. Implementation science theories can inform strategies in developing inclusive dementia-friendly community projects. For example, future projects should consider applying an established framework such as the Consolidated Framework for Implementation Research (CFIR) to optimize process and outcome evaluations (Damschroder et al., 2009).
This review identified a need for additional voices and perspectives regarding dementia friendly communities to be included in the academic literature. In particular we identified the need for studies regarding young-informal-caregivers, individuals from varied backgrounds (with regards to sex, ethnicity, culture, and socioeconomic status) and the perspective of individuals with more variability in severity of dementia symptoms. It was also recognized that additional literature identifying specific facilitators and barriers for involvement in research for inclusive dementia friendly communities by people with dementia would be beneficial.
Lastly, now more than ever, as we live through the COVID-19 pandemic, there is an even greater need for innovative approaches to promote inclusive dementia-friendly communities for social inclusion. With the rise of technologies and virtual platforms, it may be possible to explore how touchscreen phones and tablet devices may be used to support people with dementia in active engagement in DFCs, promote social inclusion, and expand public education.
Conclusion
This scoping review identified four key strategies of creating inclusive dementia-friendly communities that support people with dementia and their informal caregivers: (a) active involvement of people with dementia and their informal caregivers; (b) inclusive environmental design; (c) public education to reduce stigma and raise awareness; and (d) customized strategies informed by dementia-friendly and inclusive theories. This study has yielded insights into the key DFC strategies that provide learning opportunities for global communities with evidence to take into account for their inclusive dementia-friendly agenda. Theories in implementation science should be applied to guide research and projects to optimize the process and outcome evaluations.
Footnotes
Acknowledgements
The authors wish to thank the funding support by the Michael Smith Foundation for Health Research #18 773.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the Michael Smith Foundation for Health Research #18 773.