
Abstract
Background
People with dementia often experience stigma, abuse and social exclusion in their communities. Thus, developing dementia-friendly communities is a priority in the fight against dementia.
Objectives
This study investigated communities' attitudes towards people with dementia by exploring the colloquial terms referring to dementia and the social tolerance toward people with dementia.
Methods
A cross-sectional household study, using individual interviews, was conducted in the iLembe district, South Africa, with 300 participants aged ≥18 years. Data was collected between 2018 and 2019. Data was analysed using descriptive and reflexive thematic analyses.
Results
Two themes related to local dementia terms were identified: (i) There are no known local terms synonymous with the term dementia; (ii) Communities use inaccurate and stigmatizing terms to describe dementia. The terms identified did not accurately describe dementia, and others had negative connotations toward people with dementia. Although most participants reported being tolerant, neighbourly, and friendly towards people with dementia, their tolerance decreased when personal interaction was required with a person with dementia. Most participants reported a more agreeable attitude when considering being neighbours rather than family members of people with dementia, and 50.3% reported that their communities discriminate against older people with dementia.
Conclusion
The identified dementia terms did not promote dementia-friendly societies. Appropriate dementia terms are crucial for changing social intolerance and negative perceptions of people with dementia and promoting a dementia-friendly culture in South African communities. Terms that encourage and perpetuate stigma against people with dementia must be replaced with terms that promote inclusion and tolerance.
Keywords
Background
People with dementia often experience stigma, abuse, and social exclusion in their communities (Hung et al., 2021; Khonje et al., 2015; Mkhonto & Hanssen, 2018). Evans (2018) refers to three forms of stigma that impact people with dementia: self-stigma, public stigma, and stigma by association. Stigma and discrimination include intolerance of people with dementia and their families, negative attitudes, or behaviour such as the use of negative language or terminology, stereotyping, alienation, isolation and exclusion, and lack of access to essential care and support services (Link & Phelan, 2001; Mukadam & Livingston, 2012; Swaffer, 2014). Developing dementia-friendly communities is a priority area in the fight against dementia stigma, and it is one of the seven 2017–2025 guidelines in the World Health Organization’s (WHO) public health response to dementia (WHO, 2017). According to the WHO (2017), a dementia-friendly society provides an inclusive and accessible community environment, with enhanced opportunities for participation, health, and safety for all people, to ensure a good quality of life and dignity for people with dementia and their families. Dementia-friendly communities further create opportunities for awareness about dementia, provide support, make people with dementia feel confident about contributing to the community, and foster social inclusion and tolerance of people with dementia (Hung et al., 2021; Wu et al., 2019).
Communities’ attitudes and stigma against people with dementia can be apparent in the colloquial language used to refer to dementia (Swaffer, 2014). When used correctly, language can reduce stigma, promote social inclusion and show respect for the personhood of someone with dementia. However, when used prejudicially, language harms and stigmatizes people with dementia. Therefore, to create dementia-friendly communities, it is important to start changing the negative everyday terms used to describe dementia or those with dementia.
In the past, researchers have used derogatory, dehumanising, stigmatising, and discriminatory language toward people with dementia, such as ‘demented’, ‘victims’ and ‘not all there’ (Swaffer, 2014). Stigmatising colloquial terms, such as “crazy, possessed, spoiled ‘fsoesh’, or as having a confused head” (Berdai Chaouni & De Donder, 2018: p. 8), and ‘kharaf’ (translated as ‘loss of mind’) (Cipriani & Borin, 2015), were also used to refer to people with dementia in different communities where they live. Further terms such as ‘mental’ or ‘getting off your brain’ (Alzheimer’s Europe, 2018; Antelius & Plejert, 2016; Lawrence et al., 2011), ageing disease, disease of insanity, disease of forgetfulness, madman, and dull brain (Adebiyi et al., 2016) were also used. While these terms might be part of everyday social language, they also implicitly reinforce the stigma, social exclusion, and intolerance of people with dementia. Swaffer (2014) stated that if the language used is inclusive, non-judgmental, and person-centered (rather than centered on the disease), the social care system and language trends can help people with dementia to have better health outcomes and quality of life.
Dementia is a Western biomedical construct and as such many African languages do not have terms synonymous with the biomedical concept of dementia as found in other studies (Khonje et al., 2015; M’belesso et al., 2016). For example, researchers found that there are no dementia synonymous terms in Brazzavillean Sango, Lingala or Kituba (M’Belesso et al., 2016), Asian Punjabi (Alzheimer’s Europe, 2018), South African Xhosa (Khonje et al., 2015) and Tanzanian Swahili (Hindley et al., 2016), to name a few. The lack of appropriate terminology leads to the persistent use of inappropriate terminology in non-Western communities. Berdai Chaouni & De Donder (2018) advocate for diverse ethnic communities to construct appropriate terminology and produce dementia information in their languages. Developing simple, inclusive, and positive language can help communities replace harmful and negative terms that make the disease to be associated with shame and reinforce stigma towards people with dementia.
In some communities, dementia is associated with shame and embarrassment and because of this, some people prefer not to know or let others know that they have the disease (Adebiyi et al., 2016; Evans, 2018). Also, some relatives of people with dementia hide the status of their loved ones for fear of prejudice or violence from the community (Mkhonto et al., 2018). Therefore, societies that show prejudice and negative attitudes towards people with dementia perpetuate the isolation and exclusion of those with dementia and their families from the community. Excluding people with dementia from community interaction robs them of a good quality of life (Cohen-Mansfield & Parpura-Gill, 2007). The value of social interaction, community participation, and good social relationships with family, friends and neighbours are key elements of quality of life for older people (Bowling, 2011), regardless of their health condition. A UK report found that 33% of those living with dementia had lost friends following the diagnosis, and 39% felt lonely and not included in their communities (Alzheimer’s Society, 2013). Maintaining social inclusion and community engagement can be particularly challenging for people with dementia and their families when communities are not dementia friendly.
This study explored communities' attitudes towards people with dementia by considering the colloquial terms referring to dementia, the social tolerance toward people with dementia and the availability of dementia-inclusive services in South African communities.
Methods
Study Design and Setting
This was a mixed method, cross-sectional household study conducted in the iLembe district. iLembe district is one of the 11 districts in KwaZulu-Natal (KZN), South Africa. It has four municipalities: KwaDukuza, Mandeni, Ndwedwe, and Maphumulo. It is predominantly a rural district, with isiZulu-speaking and black African population.
Participants
We recruited 300 participants aged ≥18 using multi-stage cluster sampling with simple random sampling (Terre Blanche et al., 2006). As this study was part of a more extensive study on dementia prevalence and care, a simple random method was used to select iLembe from the 11 KwaZulu-Natal districts. Secondly, two ward areas were sampled from each of the four iLembe municipalities. After that, the participants were selected by sampling the first household in the area, followed by every fifth household. Ethical approval for the study was obtained from the University of KwaZulu-Natal (UKZN)’s Humanities and Social Sciences Research Ethics Committee (HSS/1016/017D), and the participants provided informed consent.
Procedure
Data was collected for a period of 6 months between October 2018 and November 2019. In some communities, households were too far apart, which prolonged the data collection process in those communities. Interviews were conducted at the participants’ homes in either isiZulu or English. A semi-structured questionnaire with biographical and study specific questions were used. The questionnaire included a vignette of a person with symptoms of dementia. The vignette was designed using the DSM-5 criteria for dementia (APA, 2013), which included symptoms of memory loss and other cognitive and behavioural difficulties noticed by family members and others. The following questions were asked to explore the colloquial terms used by participants to refer to dementia, as well as participants’ attitudes toward people with dementia: (1) Is there a name used to refer to dementia or people with dementia in your language or community? (2) What is the name? (3) Would you have a problem with being neighbours, friends, and family/date a person with dementia? (4) How do you think other people in your community would treat a person with dementia? (5) In your community, are there services for people with dementia?
The participants’ responses were captured using Mobenzi Researcher software (Mobenzi, 2021), which is a digital data collection tool that captures data electronically during fieldwork. After collection, data was exported into a password-protected Microsoft Excel file for cleaning and analysis. Responses in IsiZulu were translated into English by the first author and reviewed for accuracy by two independent professionals who are bilingual.
Data Analysis
The Statistical Package for Social Sciences 27 (SPSS) was used for descriptive analysis of participant characteristics and question responses (IBM Corp, 2020). Qualitative data was analysed using reflexive thematic analysis (RTA) following the stages of familiarisation, generating codes and themes, sorting, reviewing data extracts, and writing up (Braun & Clarke, 2019). RTA focuses on “the researcher’s reflective and thoughtful engagement with their data and their reflexive and thoughtful engagement with the analytic process” (Braun & Clarke, 2019, p. 594). Through the RTA, themes are not predefined to ‘find’ codes. Instead, themes are produced by organizing codes around a relative core commonality, or ‘central organizing concept,’ that the researcher interprets from the data (Braun & Clarke, 2019 Campbell et al., 2021).
To ensure the rigour of the study, credibility, conformability, transferability, and dependability (Lincoln & Guba, 1985) were considered. Firstly, a rigorous external review of the study design and procedures was conducted during the ethical clearance process. Secondly, during data collection, the researchers were in the field for a prolonged period. As suggested by Patton (2001), the researchers' prolonged engagement and persistent observation ensured that they learned more about the culture, the social and natural setting of the participants and the topic of study. Moreover, the use of triangulation (Cresswell, 1998) by the researchers ensured the accuracy of the data – i.e., this study was part of a larger study on dementia prevalence and care, where both quantitative and qualitative data was collected from multiple sources. In addition, responses in IsiZulu were backward translated into English by the researchers and confirmation of the translation and meaning were reviewed by independent professionals for accuracy. Similarly, interpretations of the findings and some cultural explanations were verified with peers who were more familiar with concepts such as amafufunyana.
Findings
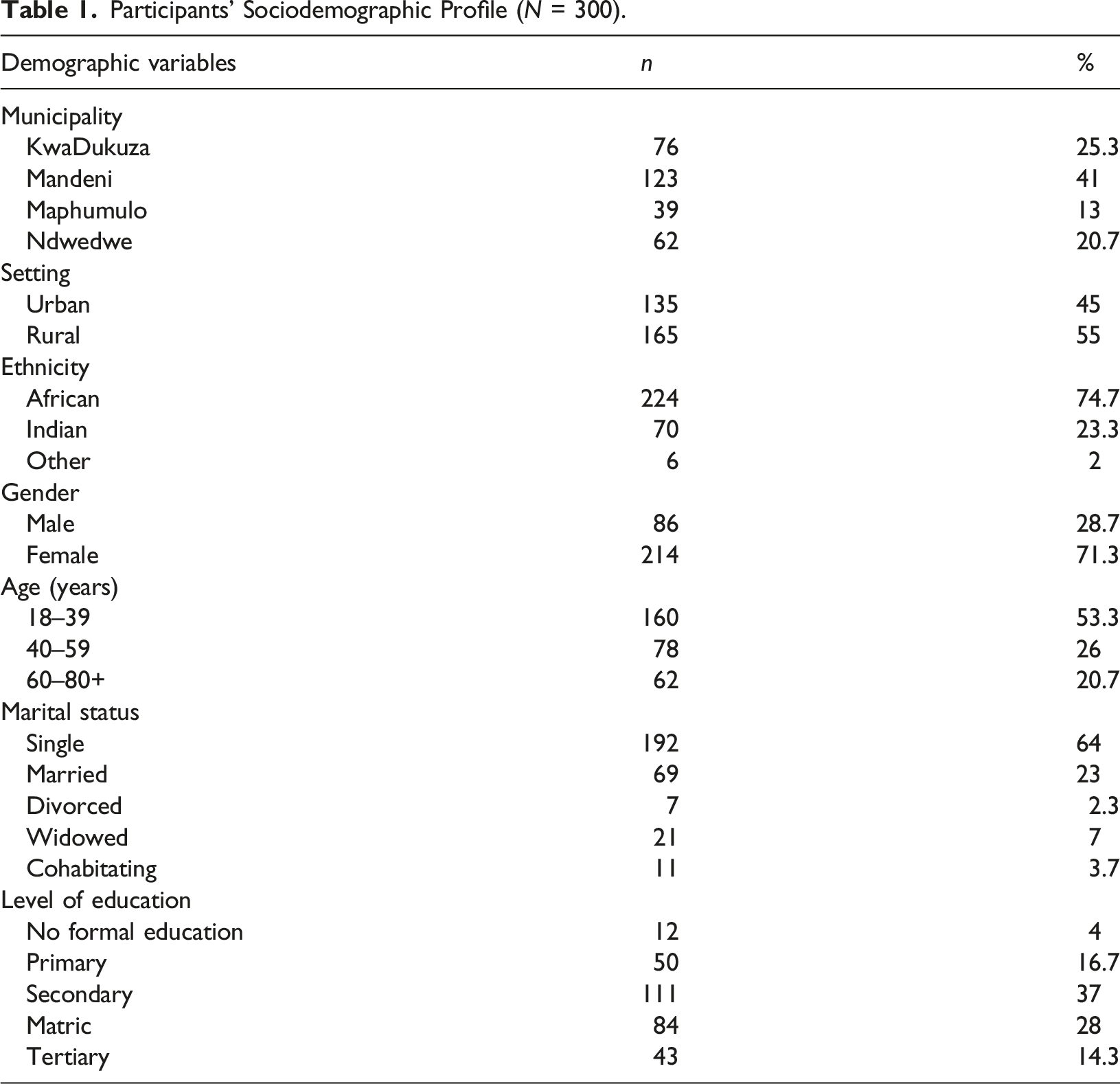
Participants’ Sociodemographic Profile (N = 300).
The Colloquial Terminology Used to Describe Dementia
Two themes emerged concerning the local terms used to describe dementia: (i) There are no known local terms synonymous with the term dementia; (ii) Communities use inaccurate and stigmatizing terms to refer to dementia, as shown in Figure 1 of the thematic map. In the extracts, the participants are identified by their municipality (KwaDukuza, Mandeni, Maphumulo, Ndwedwe), ethnicity (Black, Coloured, Indian, White), gender (female or male) and their participant number (e.g., KFB66 = KwaDukuza, female, black and participant number 66 and MaMB22 = Mandeni, male, black, participant number 22). Thematic map demonstrating the themes and terms. *Amafufunyana means that a person has been bewitched to be possessed by an evil spirit that changes their behavior.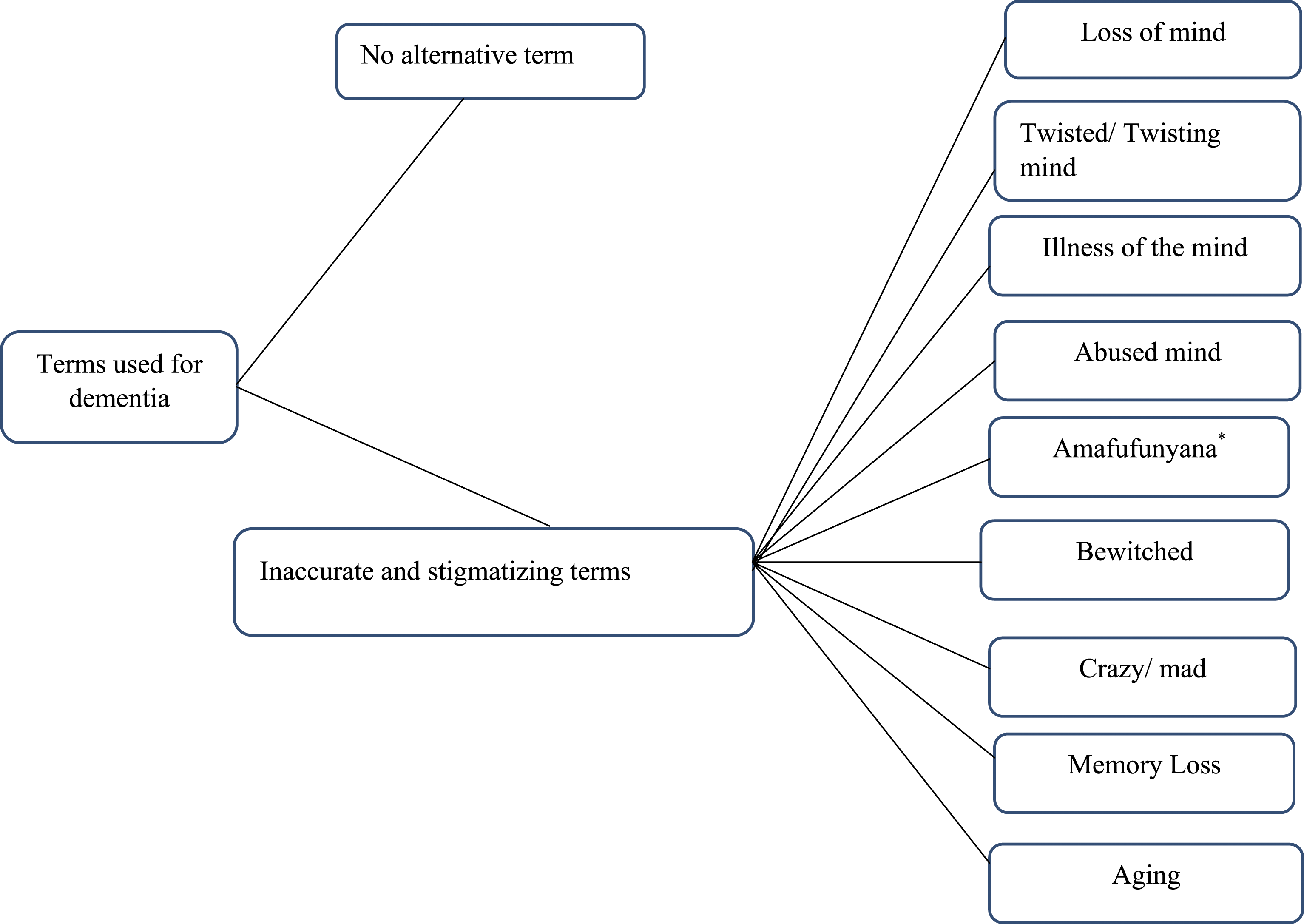
Theme 1: No known local terms are synonymous with dementia.
Most participants (n = 256; 85.3%) reported that there was no term synonymous with the biomedical term dementia in their languages and communities. A small proportion of the participants (n = 44; 14.7%) reported a term used in their communities to describe dementia. Nine colloquial terms were reported, as seen in Figure 1. These were primarily reported in the participants’ language, and from these descriptions, four subthemes emerged and are presented below.
Theme 2: Communities use inappropriate and stigmatizing terms to refer to people with dementia.
Of the 44 participants reporting a term, 72.7% reported terms that were not accurate and sometimes stigmatizing. Four subthemes emerged and participants used terms such as loss of mind’, ‘sickness of the mind’, ‘twisting of the mind’, culture-bound illness, crazy or mad, and ‘abused mind’ as seen in the subthemes below.
Dementia as a Mind Disturbance
The participants reported this subtheme as illustrated in the following extracts: KFB66: “Sikubiza ngokuphambana umqondo.” [We call it twisting of the mind.] KFI38: “It is called losing your mind.” MFB53: “Kunjengokuhlukumezeka komqondo, so sikubiza kanjalo.” [It is like an abuse of the mind, so that is how we call it.]
The excerpts imply that dementia alters a person’s mind, leading to the person losing their mind or the mind getting twisted or abused. Although these descriptions do not adequately describe the construct of dementia; they indicate that the participants understand dementia as a disease that affects and changes a person’s mind.
Some participants moved beyond the notion of dementia affecting the mind but recognised that it was also a sickness, which is involuntary. They also recognised that calling it a sickness of the mind is not its name, but they use this description in the absence of a name: NFB29: “Noma kungasilona igama kodwa sikubiza ngokugula…ukugula ngomqondo.” [Although it is not a name, but we call it being sick, being sick in the mind.]
People with Dementia were Referred to as “mad” or “crazy”
Some participants referred to dementia as being called mad or crazy in their communities. The term was presented in different languages by the participants, with one Tamil-speaking participant calling it paittiyam and isiZulu-speaking participants calling it ukuhlanya: NMB71: “Kuyafana nomuntu osuke ehlanya, ukuhlanya.” [It is like a person who is crazy…it is being crazy.] KFI61: “Oh, we call it like a mad person, like paittiyam in our language.” MaFB158: “Ukuhlanya lokho.” [That is being crazy.]
The notion that having dementia is the same as being crazy is usually associated with understanding dementia as a mental or mind illness. However, negative undertones suggest that some lose control of themselves (being mad or crazy), which could also imply a loss of autonomy, and in this way, dementia is seen as a dehumanising illness.
Dementia is Culturally Constructed
The terms reported in this subtheme were bewitched, witchcraft and amafufunyana; the latter refers to an African cultural illness that results when people are possessed by evil spirits through witchcraft, and therefore present with aberrant behaviour and psychological concerns. These words described the concept of dementia as a culture-bound illness: NFB47: “Sithi amafufunyana.” [We call it amafufunyana.] MMB34: “Kuvame ukuthi kube izifo zabantu njengokuthi uthakathiwe.” [It is usually illness caused by other people, such as being bewitched.]
The participants suggested that, in some African communities, people with dementia are seen as people who have been bewitched because they exhibit behaviours usually associated with possession by an evil entity. When dementia is equated to amafufunyana, it means that person has been bewitched to be possessed by an evil spirit that causes them to present with dementia symptoms. Also, attributing dementia to a particular cultural construct implies that dementia might only occur within that culture and not in other cultures. On the other hand, these terms show that although dementia is a western biomedical construct, the experience of it may vary across cultures.
Dementia is Identified based on its Characteristics
In this theme, 27.3% of the 44 participants reported that dementia was called ukuguga or ageing, memory loss or forgetfulness. These participants identified dementia based on when and how it occurs. MMB42: “Angithi yenziwa ukuguga, sikubiza ngokuguga.” [It is caused by old age; it is called ageing.] KFI53: “It is called memory loss.”
Dementia commonly affects older people, making the community believe it is an ageing disease. The terms ‘memory loss’ and ‘ageing’ focus on the characteristics of dementia rather than the disease itself. Although these terms describe some aspects of the disease such as that dementia affects old people and one of its primary symptoms is memory loss, they do not give a complete picture of what dementia is.
Community Reactions and Attitudes Towards People with Dementia
One hundred and 51 participants (50.3%) believed that people with dementia would be discriminated against in their community, 66 (22%) reported they would be treated well in their community, 45 (15%) believed they would not be discriminated against, and 38 (12.7%) participants were unsure how they would be treated in their community.
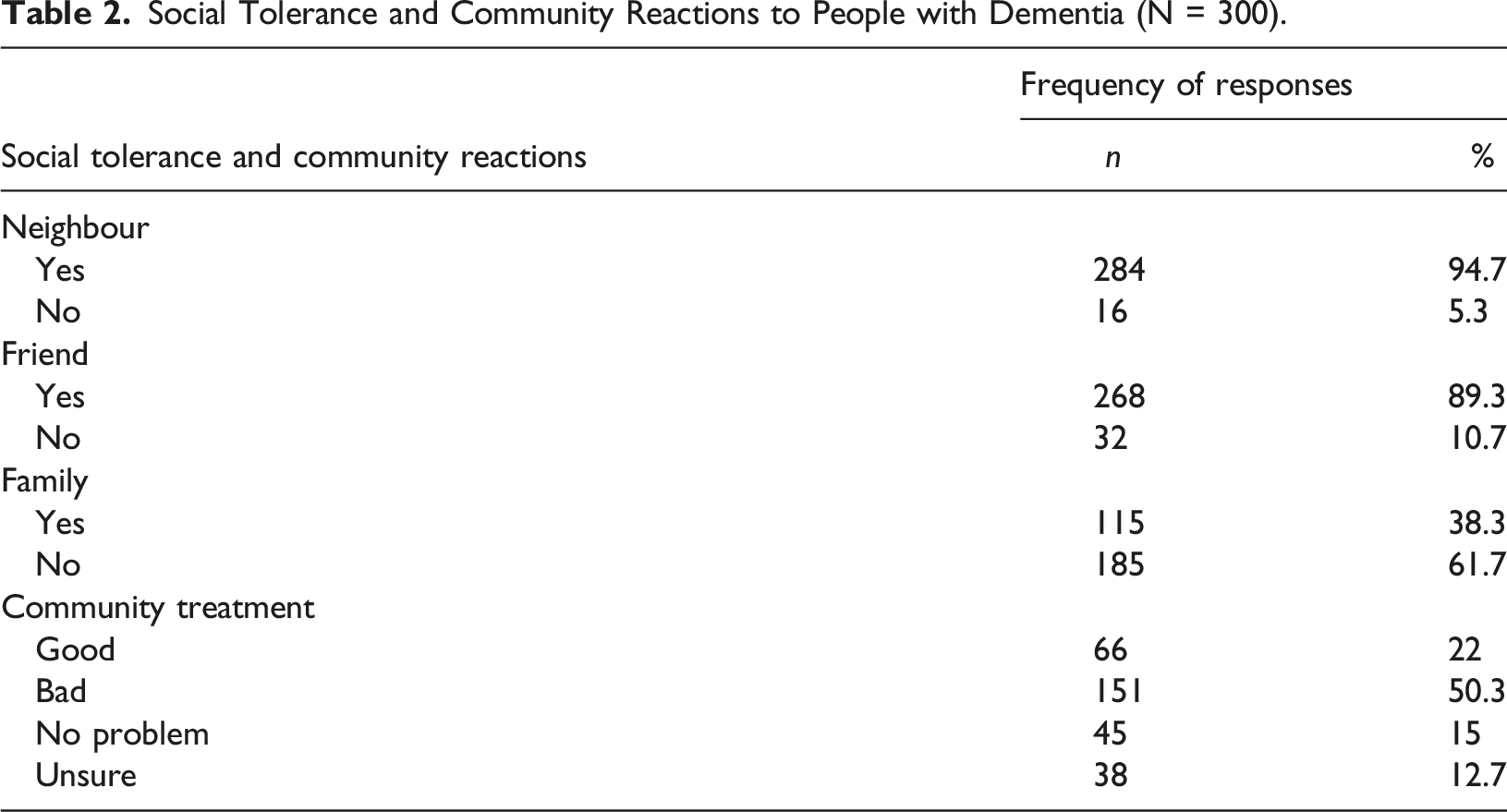
Social Tolerance and Community Reactions to People with Dementia (N = 300).
Of the 300 participants, 77 (25.7%) reported having a person living with dementia in their families. Of these 77 participants, 51.9% reported ambivalence and shame about being related to a person with dementia. In addition, of these 77 participants, 49.4% believed their communities discriminated against people with dementia. Of all participants, less than a third (30.3%) reported that their communities had services for people with dementia.
Discussion
This study investigated communities' attitudes toward people with dementia by exploring how people spoke about people with dementia and their reactions towards people with dementia. It was observed that stigma existed in the studied communities, which might act as a barrier to creating dementia-friendly communities. Most participants reported the lack of adequate dementia synonymous terms in their communities. The lack of appropriate dementia terminology has also been reported in other African countries (Hindley et al., 2016; Khonje et al., 2015; M’belesso et al., 2016). When appropriate terms are unavailable, communities commonly develop their own colloquial terms based on their understanding of the symptoms and experience of the disease. For example, in this study, communities created their own terms or descriptions because there were no official terms. Some of these descriptions, i.e., dementia being called ‘crazy’, ‘madness’, ‘twisting or loss of mind’, ‘witchcraft’ and amafufunyana, had negative connotations and stigmatised people with dementia. Communities are encouraged to construct simple, inclusive, and accurate dementia terms in their languages to replace harmful terms that devalue people with dementia and reinforce their social exclusion in South African communities (Berdai Chaouni & De Donder, 2018).
Secondly, the participants understood that dementia occurred in older people and that the symptoms included forgetfulness; therefore, they described dementia as old age or forgetfulness. When symptoms of dementia are normalised as part of ageing, they depict ageing as being unhealthy. Therefore, older people are treated as different and with prejudiced. Older people are already marginalised in most communities due to age (Evans, 2018). This is commonly known as ageist discrimination (Evans, 2018) and often crosses with other forms of stigma and discrimination (Jacobs et al., 2022). This means that older people then experience double stigmatisation - discrimination because of their age and dementia. Also, when dementia is recognized simply as ageing, it is normalised and not seen as a disease. Therefore, families might be reluctant to seek help when their loved ones start presenting with dementia symptoms (Jacobs et al., 2022). Normalizing dementia symptoms also means that the development and provision of services for people with dementia might not be prioritised in these communities because of the perception that the demand for services is low. Dementia community-based services in South African communities are already limited, as only a third of the participants reported having dementia services in their communities.
In many African communities, dementia has also been associated with cultural syndromes or being culture-bound (Berwald et al., 2016; Milne, 2010; Mkhonto & Hanssen, 2018; Mukadam & Livingston, 2012; Sayegh & Knight, 2013). In this study, dementia was also referred to as amafufunyana. Amafufunyana as a cultural construct is usually observed in African cultures. In addition, people with dementia were associated with other cultural phenomena, such as witchcraft (being bewitched or being a witch). This was also seen in another South African study (Mkhonto & Hanssen, 2018). Although witchcraft is not particular to Africa, in South Africa, it is a phenomenon that is associated with specific African traditions and cultures (de Jong et al., 2022). In South African communities, it is not uncommon for older women suspected of dementia to be accused of witchcraft and murdered by their communities (de Jong et al., 2022; KwaZulu-Natal Legislature, 2022), particularly in KZN and Eastern Cape provinces. Mkhonto & Hanssen (2018) reported that when people with dementia are associated with witchcraft, their lives are in danger as they can be abused, ostracised, and even killed. When dementia is associated with phenomena related to particular cultures, it discriminates against those with the disease and entire cultural groups.
Some families may prefer to conceal dementia within their families as they are afraid of being stigmatised or associated with the disease – stigma by association (Evans, 2018). Almost a third (61.7%) of the participants shared this view; they would prefer being neighbours over being related to a person with dementia. More than half of the participants (51.9%) with family members living with dementia reported negative reactions to being connected to a person with dementia. In addition, 64% of those who described dementia as a disease that affects the mind and 50% as a culture-bound syndrome were unwilling to be personally associated with people with dementia. Showing a link between the terms used and the participants' perceptions and attitudes towards people with dementia. When people with dementia and their families are stigmatised, it can impede help-seeking and increase feelings of low self-esteem, shame, and dehumanisation (Urbańska et al., 2015), as well as increase loneliness and isolation (Mukadam & Livingston, 2012).
Although some terms captured characteristics of dementia (i.e., dementia is a brain disease characterised by memory loss that can affect older people), some terms were offensive and discriminatory. Discriminatory terms seemed normalised and shared in some communities, indicating the possibility of unveiled or implied stigma (Adebiyi et al., 2016) against people with dementia. Stigma leads to social exclusion and rejection, making these communities unfriendly and unsafe for people with dementia.
Social tolerance and inclusion of people with dementia are crucial to creating dementia-friendly communities. The study found that tolerance of people with dementia was high when participants were asked to consider people with dementia as neighbours (94.7%) and friends but lower (38.5%) when they had to consider them as relatives or loved ones. This showed that, possibly due to social desirability, communities might display an attitude of tolerance towards people with dementia while simultaneously harbouring stigma. This was also suggested by 49.4% of the participants with relatives diagnosed with dementia. These participants reported that people with dementia were discriminated against in their communities. The discrimination of families might be one of the reasons why more than half of the participants (51.9%) who have a family member with dementia reported ambivalence and shame about being related to a person with dementia. Dementia discrimination can lead to families being socially excluded and ostracised (Gurayah, 2015; Mkhonto & Hanssen, 2018), and because of this, caregivers are likely to resent their role (Brodaty & Donkin, 2009), hide relatives with dementia and not seek help from formal health institutions and community services (Mukadam & Livingston, 2011; Jacobs et al., 2022).
There is an urgent need to reduce the stigma and negative connotations associated with dementia to improve the lives of people with dementia and their families, especially in low- and middle-income countries such as South Africa. Communities need to encourage acceptance and friendliness towards people with dementia. The South African government, in particular ministries of health, needs to prioritise dementia education and awareness, especially in KZN and Eastern Cape provinces, where dementia is still strongly associated with witchcraft and other negative perceptions.
Limitations
Data were not audio-recorded but were manually written into the data collection tool; audio-recording the interviews could have improved the richness of the extracts. This is because although all research assistants received training and captured data as verbatim as possible, some researchers wrote more information than others; for example, when participants were asked to give a name for dementia, some responses had more detail, whereas others just gave the term. It is unclear if this was because the participants did not elaborate or because of how data was captured. It is recommended that a voice recording function is added to the Mobenzi software.
Conclusion
The study found that some South African communities lack relevant and accurate terms to describe dementia. Most of the terms reported in this study showed that the communities have negative attitudes and might perpetuate stigmatisation of people with dementia. The terms were also inappropriate and did not correctly present or describe what dementia is. Updated and representative terms, and public awareness about dementia, might significantly reduce the stigma associated with dementia. The terms used to describe dementia need to focus on the abilities (rather than the deficits) of people with dementia and promote dignity while accurately depicting the disease. Tolerance of people with dementia might be superficial, with participants wanting to look or seem appropriate, but the language used shows the implicit presence of socially accepted public stigma. More intentional efforts are needed to use dementia-friendly terms and include services for people with dementia in South African communities.
Footnotes
Author Contributions
All authors listed contributed to the study’s conceptualisation and writing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of KwaZulu-Natal’s UCDP.
Ethical Approval
Ethical approval for the study was obtained from the University of KwaZulu-Natal’s Humanities and Social Sciences Research Ethics Committee (HSS/1016/017D),