
Abstract
There is limited empirical knowledge about how older adults living with dementia enact their social citizenship through out-of-home participation. This study aimed: (a) to investigate out-of-home participation among older adults with and without dementia in four countries and (b) to compare aspects of stability or change in out-of-home participation. Using a cross-sectional design, older adults with mild-to-moderate dementia and without dementia, aged 55 years and over, were interviewed using the Participation in ACTivities and Places OUTside the Home questionnaire in Canada (n = 58), Sweden (n = 69), Switzerland (n = 70), and the United Kingdom (n = 128). Data were analyzed using descriptive statistics and a two-way analysis of variance. After adjustment for age, diagnosis of dementia and country of residence had significant effects on total out-of-home participation (p < .01). The results contribute to policies and development of programs to facilitate social citizenship by targeting specific activities and places.
Keywords
What this paper adds
• A cross-national perspective of out-of-home participation among older adults living with and without dementia. • After adjustment for age, diagnosis of dementia and country of residence had significant effects on out-of-home participation among the participants.
Applications of study findings
• We propose a strengths-based view of older adults living with and without dementia as they enact their social citizenship through participation in activities and places in their communities. • To develop more targeted programs, policies, and built environment interventions for older adults living with and without dementia, there is a need to focus on maintaining participation in specific activities and places in the community.
Background and Objectives
Out-of-home participation is considered to promote and maintain health and well-being among older adults living with and without dementia (Douglas et al., 2017; Evans et al., 2019), and yet existing substantive knowledge in this area and methodological understanding are limited. Health and well-being benefits associated with out-of-home participation include social interaction (Livingston et al., 2020), mental health promotion (Mackenzie & Abdulrazaq, 2021), cognitive stimulation (Evans et al., 2019), physical activity, and mobility (Odzakovic et al., 2020). However, health and well-being are more than individual concerns; they are also socially constructed (Douglas et al., 2017).
Increasingly, research suggests that older adults living with and without dementia participate in activities and places outside their home not only for health, functional and mobility benefits, but also as a way to enact their social citizenship (Bartlett, 2021; Nedlund et al., 2019). In dementia research, social citizenship refers to “a relationship, practice or status, in which a person with dementia is entitled to experience freedom from discrimination, and to have opportunities to grow and participate in life to the fullest extent possible” (Bartlett & O'Connor, 2010, p. 37). Our conceptualization builds on the theory of social citizenship which recognizes that older adults living with and without dementia are active agents with competencies, histories, rights, and responsibilities, which link the person to a community and country of residence (Bartlett & O'Connor, 2010).
A theory of social citizenship provides a lens, which helps understand the ways in which older adults, including those living with dementia, enact their agency and citizenship though participation in “ordinary places” (Nedlund et al., 2019). Older adults can enact their citizenship outside the home through their ongoing and everyday participation in “ordinary places” such as the neighborhood, a grocery store, and a friend or family member’s place (Bartlett, 2021; Fransen-Jaïbi et al., 2021). Activities are embedded in these places, and thus, activities and places are integrally linked. For the purposes of this study, participation is viewed as linking the person, place, and activities (Gan et al., 2021).
The present study’s conceptualization of social citizenship is aligned with a strengths-based view of out-of-home participation that draws on the lived experience of older adults and frames places outside the home as zones of mastery, opportunity, and challenge (Ward et al., 2021). This approach acknowledges the agency of older adults living with or without dementia to enact their social citizenship by choosing to participate in some activities and places, and not others; thus, focusing on out-of-home activities and places that are abandoned, as well as those that are maintained.
Both aging and living with a diagnosis of dementia can affect older adults’ out-of-home participation (Hedman et al., 2017; Nygård & Kottorp, 2014). These age-related changes such as decline in functional, sensory, physical, and cognitive capabilities may impact participation, for instance, due to reduced range of movement, stamina or coordination, which may inhibit mobility (Brorsson et al., 2020; Kuspinar et al., 2020; Mick et al., 2018), or exacerbate wayfinding or navigation related challenges (Wiener & Pazzaglia, 2021) while outside the home.
The complexity of out-of-home participation suggests that individuals’ cognitive status and age need to be considered in relation to other factors potentially influencing out-of-home participation, such as the “living environment” (Kuspinar et al., 2020; Ward et al., 2021). For the purposes of this study’s focus on out-of-home participation, the living environment encompasses the different activities and places where older adults may enact their social citizenship outside of their homes, including the neighborhood and community at large. There are structural and contextual aspects that influence the living environment; thus, opportunities for out-of-home participation may vary among different countries (Townsend et al., 2021). Structural and contextual aspects include city planning, urban design and walkability (Biglieri, 2018; Houston et al., 2020), proximity to nature (Sturge et al., 2021), socio-economic status (d'Orsi et al., 2014; Gaber et al., 2020; Wallcook et al., 2021), access to public transport and transport services (Kizony et al., 2020; Mouratidis, 2018), access to health care services including diagnostic and support services for older adults living with dementia and other age-related or disabling conditions (Gan et al., 2021).
In addition to structural and contextual aspects of participation in the living environment, there are also social aspects to consider. Cultural norms and values concerning age and dementia can impact out-of-home participation (Bartlett & Brannelly, 2019; Blackman et al., 2003). For older adults living with dementia, there can be additional social stigma which may increase the risk of stress, shame, and embarrassment in public places, leading them to avoid out-of-home participation (Blackman et al., 2003; O'Connor et al., 2018; Renn et al., 2021); this consequently diminishes the health and well-being benefits of out-of-home participation. Dementia-friendly communities encompass places and initiatives that seek to address these considerations by empowering and supporting the equal rights and resources of older adults living with dementia and their care partners, through several strategies including increasing public awareness, supportive programs and services, responsive social practices and adaptation of the physical environment (Biglieri, 2018; Gan et al., 2021; Wiener & Pazzaglia, 2021). Thus, dementia-friendly communities may facilitate opportunities for social citizenship. Nonetheless, there is insufficient knowledge on comparative out-of-home participation as an indication of social citizenship in various countries, and whether there are significant similarities or differences between older adults living with or without dementia.
Based on our conceptualization and earlier research, in this study, we hypothesized that (a) older adults living with dementia would participate in fewer activities and places outside the home than older adults living without dementia; (b) older adults living with dementia would have abandoned a higher number of activities and places outside the home between the past and present than older adults living without dementia; and (c) that having a diagnosis of dementia and the country of residence would have a significant effect on out-of-home participation, when controlling for age. Thus, this study aimed (a) to investigate out-of-home participation among older adults living with and without dementia in four countries and (b) to compare aspects of stability or change in out-of-home participation across those countries.
Methods
Study Design and Setting
Overview of the Contextual Characteristics of the Sample of Older Adults Living With and Without Dementia in the Four Participating Countries.
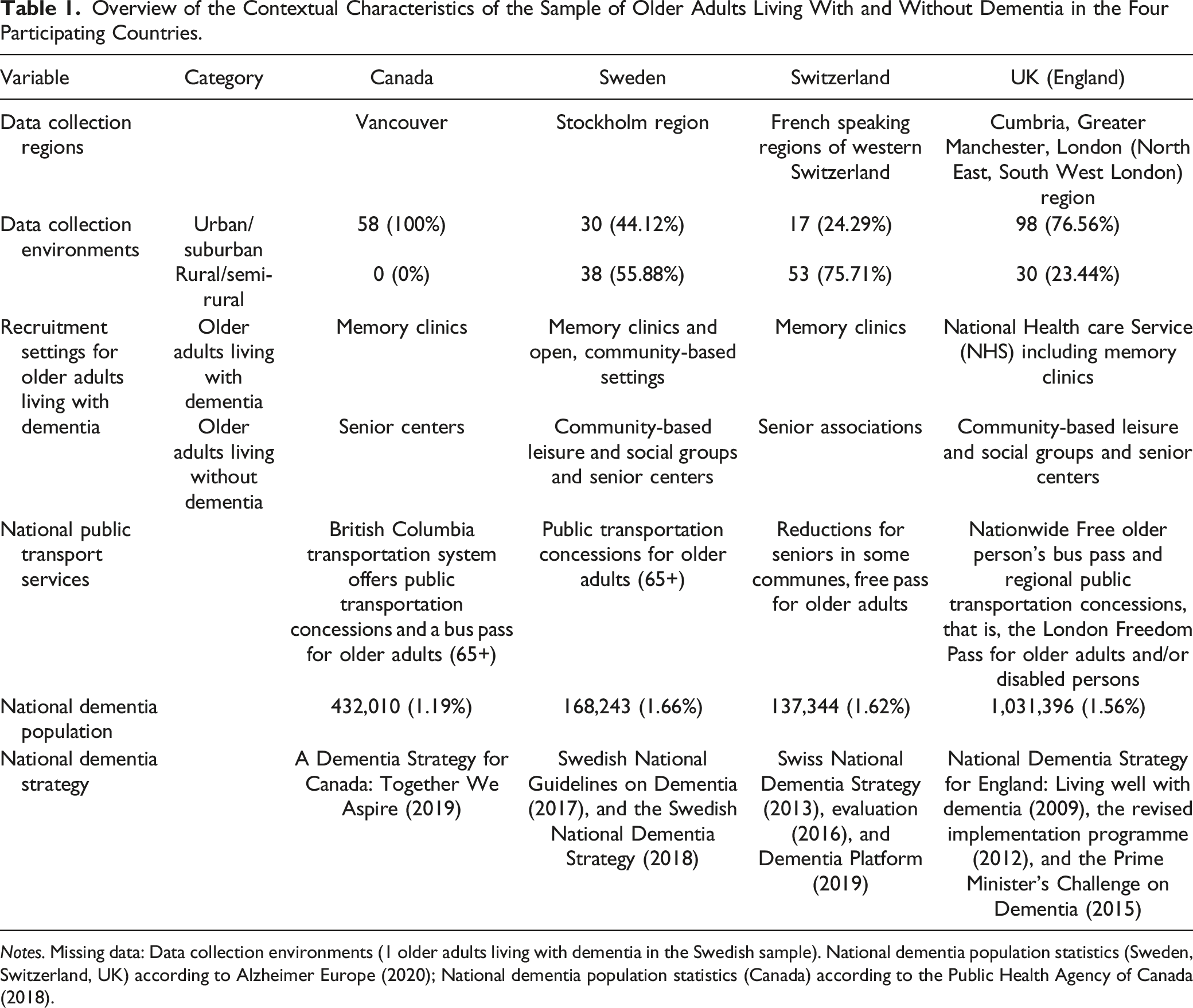
Notes. Missing data: Data collection environments (1 older adults living with dementia in the Swedish sample). National dementia population statistics (Sweden, Switzerland, UK) according to Alzheimer Europe (2020); National dementia population statistics (Canada) according to the Public Health Agency of Canada (2018).
Participants
Background Characteristics of the Sample (n = 325).
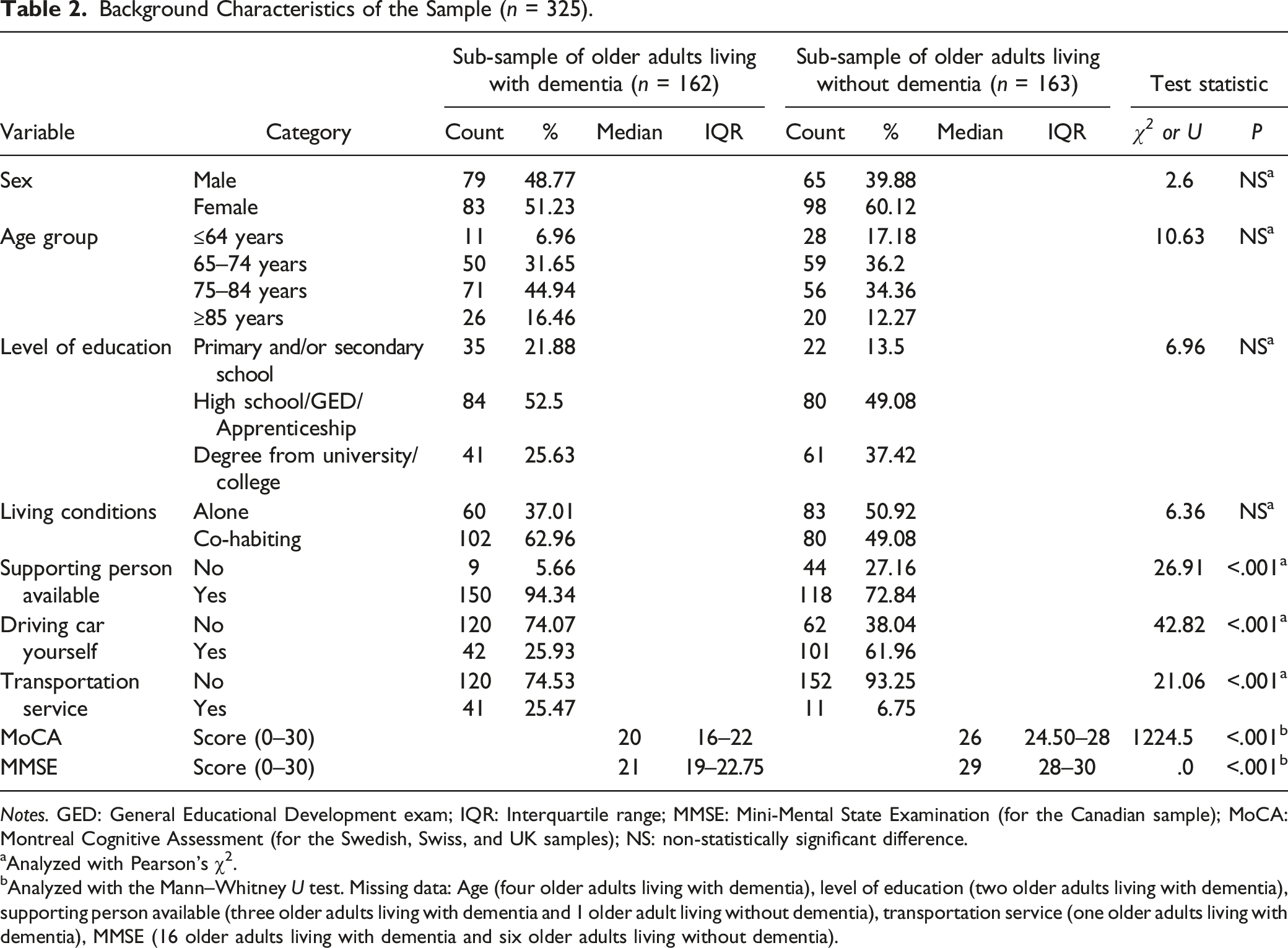
Notes. GED: General Educational Development exam; IQR: Interquartile range; MMSE: Mini-Mental State Examination (for the Canadian sample); MoCA: Montreal Cognitive Assessment (for the Swedish, Swiss, and UK samples); NS: non-statistically significant difference.
aAnalyzed with Pearson’s χ2.
bAnalyzed with the Mann–Whitney U test. Missing data: Age (four older adults living with dementia), level of education (two older adults living with dementia), supporting person available (three older adults living with dementia and 1 older adult living without dementia), transportation service (one older adults living with dementia), MMSE (16 older adults living with dementia and six older adults living without dementia).
The same inclusion and exclusion criteria were adopted across the four countries. Older adults were included if they were aged 55 years and above, living at home in their community, and they could communicate for themselves during an interview. For those living with dementia, a diagnosis of dementia was given by a physician and the participants were recruited from memory clinics (Canada, Sweden, snd Switzerland) and the National Health Service (UK). The data collectors used the brief cognitive screening tools that were commonly used in clinical practice at each recruitment site. Thus, the data collectors in Sweden, Switzerland, and the UK used the Montreal Cognitive Assessment (MoCA), whereas the data collectors in Canada used the Mini-Mental State Examination (MMSE). The older adults living without dementia were recruited through senior centers (Canada), senior associations (Switzerland), and local networks, such as community-based leisure and social groups (Sweden, UK). All participants provided their verbal and written informed consent for inclusion before they participated. This research was granted ethical approval by the Office of Research Ethics at Simon Fraser University (2017s0052) for the Canadian sample, the Regional Board of Research Ethics (2015/77-31-5) for the Swedish sample, the Commission cantonale d’éthique de la recherche sur l'être humain in Lausanne (protocol 452/15) for the Swiss sample, and the Health Research Authority (IRAS project ID: 215654, REC reference: 17/SW/0091) for the UK sample. This study adhered to the principles of the Helsinki Declaration (World Medical Association, 2013).
Measures and Materials
Total Out-of-Home Participation
This paper used the Participation in ACTivities and Places OUTside Home Questionnaire (ACT-OUT) as a novel tool to explore social citizenship through the older adults’ patterns of out-of-home participation in activities and places (Margot-Cattin et al., 2019). The ACT-OUT questionnaire was developed with older adults living with and without dementia and an in-depth explanation of the development process in three languages (English, French, and Swedish) can be found elsewhere (Margot-Cattin et al., 2019). Earlier studies using the ACT-OUT questionnaire in different countries (Chaudhury et al., 2021) and in conjunction with other instruments (Gaber et al., 2021; Margot-Cattin et al., 2021; Wallcook et al., 2021) contribute to the validity of the ACT-OUT questionnaire. Further psychometric testing is underway.
The ACT-OUT questionnaire has three parts. Part one maps past and present participation in 24 types of places and activities, part two elicits more detail about the activities performed in two places for each domain, and part three enquires about perceived risks when participating outside the home. For the purposes of this study, only part one was utilized to map participation according to four domains: (A) Consumer, administrative and self-care places (n = 6), (B) Places for medical care (n = 5), (C) Social, cultural and spiritual places (n = 6) and (D) Places for recreational and physical activities (n = 7). The participants responded yes (1) or no (0) to participating in each type of place in the past and present and these responses were used to calculate total out-of-home participation scores out of a maximum of 24 places. The past and present time-points for participation were self-determined by each participant.
Factors
Sociodemographic and other background characteristics collected using a demographic questionnaire were selected as factors (i.e., categorical variables) (Table 2). These factors were selected due to the statistically significant differences between the sub-samples of older adults living with and without dementia (i.e., supporting person available, driving a car yourself, and access to a transportation service) and based on earlier research which indicates that age (Hedman et al., 2017), cognitive status or diagnosis of dementia (Nygård & Kottorp, 2014) and differences between countries (Gan et al., 2021) may influence out-of-home participation.
Procedures
Data Collection
Data were collected between 2015 and 2017. For the ACT-OUT and demographic questionnaires, the investigators elicited questions and recorded the participants’ responses using the data collection tools. Data were collected using face-to-face interviews at the participants’ homes or another location of their choice. Participants could elect to have a significant other (i.e., spouse, partner, or any caregiver such as a sibling, or adult child) present for support during the interview, but not for proxy-reporting. To ensure a flexible approach to meet the participants’ needs, abilities and routines, the interview procedure could be spread across three different sessions with each session lasting under 90 minutes.
Data Analysis
Analyses first compared stability and change in out-of-home participation between the sub-samples of older adults living with and without dementia in the four countries using descriptive statistics (hypotheses a and b). The next stage of analyses investigated the effects of the factors using univariate analyses and a multivariate model investigating whether having a diagnosis of dementia and the country of residence would have a significant effect on out-of-home participation, when controlling for age (hypothesis c).
Differences between the sub-samples of older adults living with and without dementia were investigated using the independent samples t-test. Differences comparing past and present participation within each sub-sample were tested using the dependent samples t-test. To minimize the risk of Type I errors, the significance value was set at p < .01 for all analyses, including Bonferroni corrections. The results were interpreted according to the effect size thresholds for partial eta squared (.01 = small; .06 = medium; .14 = large effect) (Cohen, 1988).
Preliminary tests revealed no violation of the assumptions to ensure the data fulfilled criteria for a two-way analysis of variance (ANOVA) i.e., normality, linearity, homogeneity of variances or collinearity. One outlier was identified; however, sensitivity analyses showed no significant effect on the results when the outlier was removed from the models; thus, it was included in the analyses. Univariate analyses were performed, followed by a backward selection procedure to identify, and to remove, statistically redundant variables with a significance value less than .01 (supporting person available, driving a car yourself, transportation service). The backward selection procedure was motivated by the lack of earlier research regarding the relationship between the variables. In the final multivariate model, we conducted a two-way ANOVA to investigate the main and interaction effects of diagnosis group and country of residence on total out-of-home participation, when controlling for age group (Table 5). Moreover, we performed pairwise comparisons using the Least Significant Difference test, to determine statistically significant differences in total out-of-home participation between diagnosis, country of residence and age groups (Table 6)
Results
We begin by presenting the background characteristics of the two sub-samples. Next, we present the descriptive results in relation to hypotheses a and b, followed by the main results from the statistical model, to address hypothesis c.
Background Characteristics of the Sub-Samples
Table 2 presents comparisons of background characteristics and identifies the significant differences between the sub-samples of older adults living with and without dementia.
Total Out-of-Home Participation (Hypothesis a)
Mean Out-of-Home Present Participation in the ACT-OUT Questionnaire According to the Total Number of Places and for Each Domain A-D.
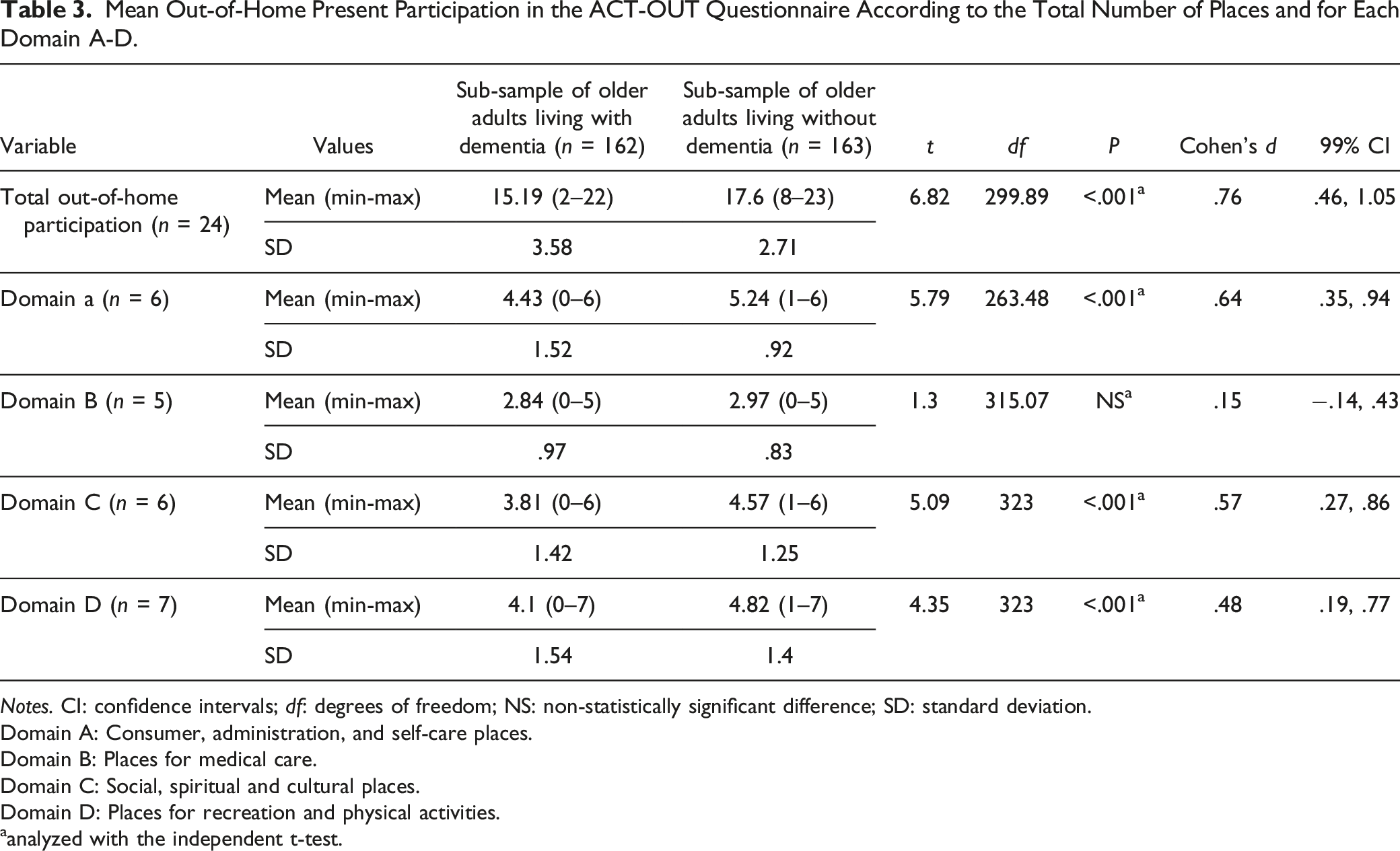
Notes. CI: confidence intervals; df: degrees of freedom; NS: non-statistically significant difference; SD: standard deviation.
Domain A: Consumer, administration, and self-care places.
Domain B: Places for medical care.
Domain C: Social, spiritual and cultural places.
Domain D: Places for recreation and physical activities.
aanalyzed with the independent t-test.
Stability and Change in Out-of-Home Participation According to Place Type (Hypothesis b)
Percent Difference in Past and Present Out-of-Home Participation in the ACT-OUT Questionnaire According to Each Type of Place.
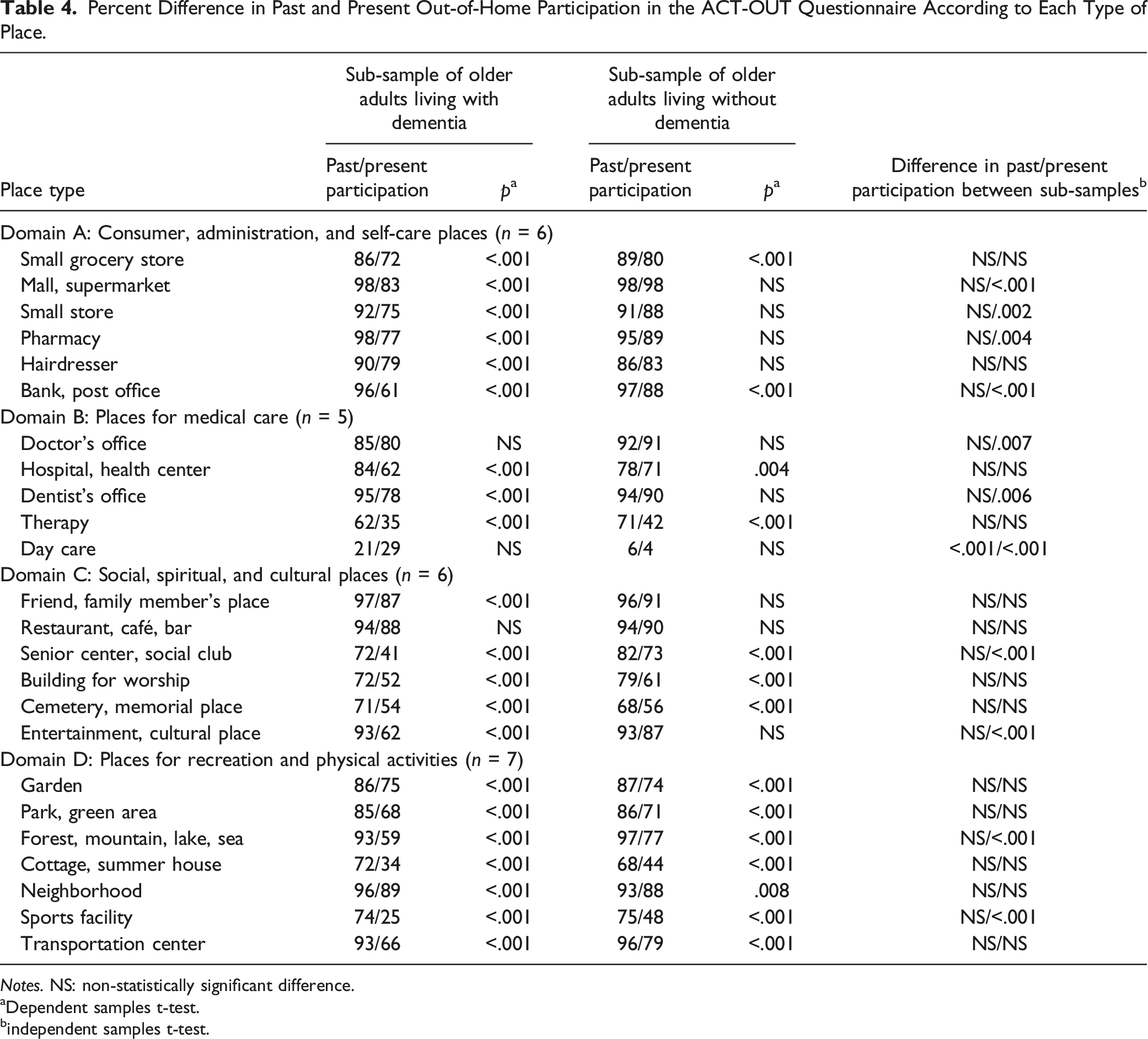
Notes. NS: non-statistically significant difference.
aDependent samples t-test.
bindependent samples t-test.
Results from the two-way analysis of variance (ANOVA) (Hypothesis c)
Results From ANOVA.
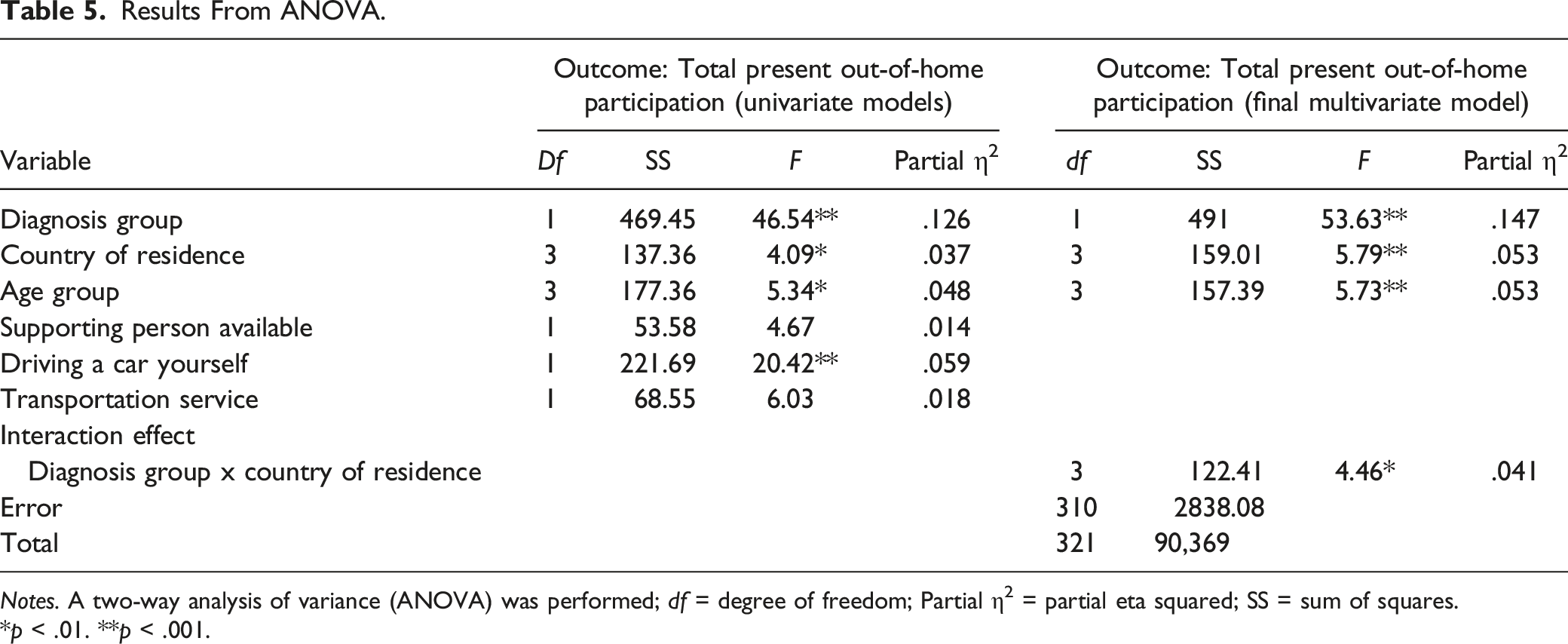
Notes. A two-way analysis of variance (ANOVA) was performed; df = degree of freedom; Partial η2 = partial eta squared; SS = sum of squares.
*p < .01. **p < .001.
Pairwise Comparisons Between Country of Residence and Age Groups
Pairwise Comparisons of Total Out-of-Home Participation Between Diagnosis, Country of Residence, and Age Groups.
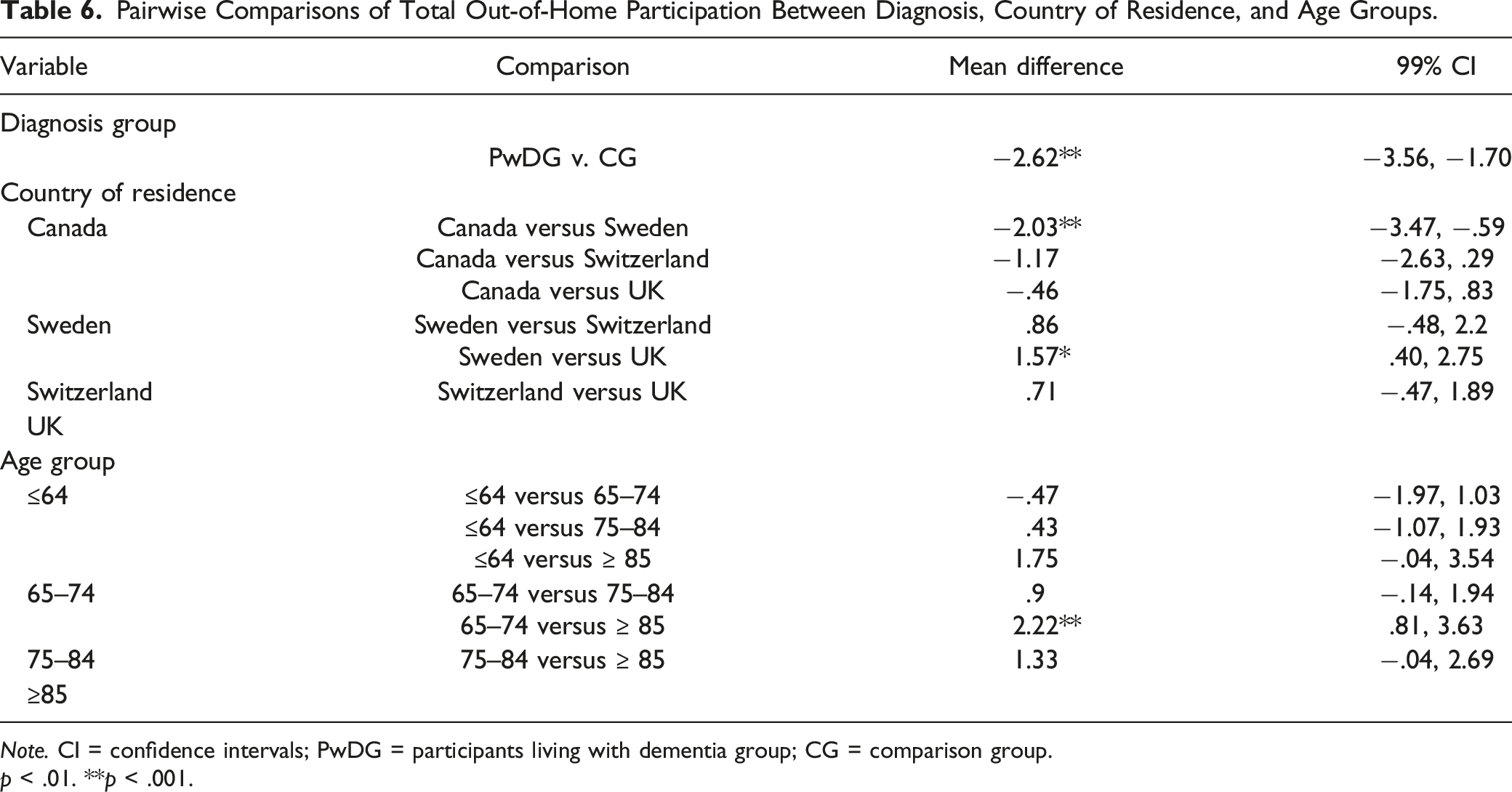
Note. CI = confidence intervals; PwDG = participants living with dementia group; CG = comparison group.
p < .01. **p < .001.
Discussion and Implications
The older adult study participants living with and without dementia participated in activities and places outside the home which can be seen as a way of enacting their social citizenship. However, the data from this study support our hypothesis (a) that older adults living with dementia participated in fewer activities and places outside the home than the older adults living without dementia.
The close examination of the older adults’ participation in domains and places of the ACT-OUT questionnaire in this study contributes increased understanding of older adults’ social citizenship by being engaged in the community. The pattern of significantly lower out-of-home participation among older adults living with dementia compared to those living without dementia was evident in the following place domains: Consumer, administration, and self-care places; Social, spiritual and cultural places; and Places for recreation and physical activities. However, there was no statistically significant difference in participation in Places for medical care between the sub-samples. Participation in Places for medical care is important for older adults, particularly those living with a diagnosis of dementia (Bayat et al., 2021). However, there may be detrimental consequences for the older adults’ social citizenship, health, and well-being, when they are no longer able to participate in those activities at the places that have been abandoned over time (Douglas et al., 2017; Evans et al., 2019). Further research is required to understand the individual level cognitive, perceptual and affective challenges, and socio-environmental barriers in the community, that may influence the lower out-of-home participation in the various types of activities and places, among older adults living with dementia. We also need to have a more in-depth and nuanced understanding of the relevance and meaning of lowered participation in maintaining or enacting social citizenship.
Regarding aspects of stability and change in out-of-home participation, the results support our hypothesis (b) that the older adults living with dementia abandoned a higher number of activities and places outside the home between the past and present than the older adults without dementia. Despite the decreases in out-of-home participation, both older adults living with and without dementia continued to participate in a variety of places. For older adults living with dementia, their experiences of socially rich “third places” in the community decline more over time than other older adults, which can exacerbate negative health effects due to less social stimulation (Oldenburg, 1989). “Third places” are places that provide opportunities for social engagement outside of home (first place) or work (second place) (Oldenburg, 1989). Participation among older adults living with dementia may decline in “third places,” including Social, spiritual and cultural places such as going to a Restaurant, café or bar, and visiting a Senior center or social club, or Places for recreation and physical activities such as sitting in a Park, green area. These represent a range of places for different purposes, levels of social engagements and activities that can provide an opportunity to be social, to observe and to talk to other people without the burden of formal social interactions which older adults living with dementia may perceive as challenging (Burton & Mitchell, 2006). Thus, future research may benefit from a deeper exploration of participation in these “third places” among older adults living with dementia (Mouratidis, 2018).
The finding that older adults living with dementia retained some place types and abandoned others underscores the need to conduct in-depth research on the socio-environmental characteristics and processes of engagement in specific place types. Table 4 shows that present participation was significantly lower in 10 place types among the sub-sample of older adults living with dementia compared to the sub-sample without dementia. The significantly lower participation in these 10 place types may be due to various reasons, including the preferences of the older adults themselves. However, it may also be due to accessibility issues or insufficient opportunities to participate in activities in these place types (Gan et al., 2021; Houston et al., 2020). Earlier research focused on participation in grocery stores and supermarkets suggests that older adults living with dementia experience increased challenges related to both their personal capabilities and the characteristics of the place which can limit participation (Brorsson et al., 2020).
The 10 place types at greater risk of being lost among older adults living with dementia point to the importance for developing responsive policy, services and programs for social practices, built environmental features, and organizational commitment in these place types. Increased knowledge is needed about the nature of experience of those activities and places where there was lower participation among the older adults living with dementia, to explore the meaning of lower out-of-home participation in relation to social citizenship and to promote cohesion between person and place through age-friendly communities in general and dementia-friendly communities specifically (Gan et al., 2021). To facilitate social citizenship, communities should consider the activities and places that older adults living with dementia value or need to participate in their everyday lives, but also whether older adults living with dementia can be supported to participate in these places (Houston et al., 2020; Sturge et al., 2021). Thus, this study contributes to the knowledge base regarding the types of activities and places which may benefit from targeted interventions and adaptations to enable older adults to enact their social citizenship through out-of-home participation.
We can also accept our hypothesis (c) that having a diagnosis of dementia and the country of residence have a significant effect on out-of-home participation, when controlling for age among our sample. The statistically significant interaction effect suggests that the experience of living with dementia may vary between countries and reinforces the call for research to focus on other aspects of participation, such as contextual consideration, in relation to the older adults’ diagnosis of dementia (Chaudhury & Oswald, 2019; Gan et al., 2021). More specifically, pairwise comparisons indicated that the mean total out-of-home participation was significantly higher for the older adults living with and without dementia in Sweden compared with those living in Canada and the UK. Further research is needed to unpack these cross-national aspects of out-of-home participation on a more granular level, including differences in experiences of stigma, whilst controlling for differences between samples.
The mean total out-of-home participation was significantly higher among participants aged 65–74 years than participants in the oldest age group (i.e., ≥85 years), and this corroborates earlier research linking increased age with decreased participation in activities among older adults (Hedman et al., 2017; Henning et al., 2021). However, it is somewhat surprising that the highest mean total out-of-home participation was among participants aged 65–74 years as opposed to the youngest age group (i.e., ≤64 years). This age group corresponds to the age of retirement among the four countries, and thus, retirement-related changes in out-of-home participation should be explored in future research.
Limitations
The interpretation and contribution of this study’s results should be considered according to the following limitations. Due to the cross-sectional study design, it was possible to identify associations but not causal relationships among the study factors. Each participant interpreted past participation individually and retrospectively. Thus, the heterogeneity of responses is a limiting factor for comparisons across individual participants. The relatively small sample size recruited using purposive sampling was sufficient to meet the assumptions of the statistical models; however, it may limit the generalizability of the results particularly due to contextual differences between countries (Table 1). The results from this exploratory study may be investigated further employing a larger sample size, with balanced groups, and randomized sampling methods.
Conclusion
This study has proposed a strengths-based view of the older adults living with and without dementia who enacted their social citizenship through participation in activities and places in their communities. The results underline the importance to consider not only older adults’ diagnosis of dementia, but also structural and contextual aspects of their country of residence which may also significantly impact out-of-home participation. More specifically, to enable the social citizenship of older adults, it is important to closely examine the types of activities and places where older adults living with dementia had significantly lower participation than older adults living without dementia, and to identify implications for responsive programs, policies and built environmental interventions.
Footnotes
Acknowledgments
The authors wish to thank all study participants and the statisticians at the Medical Statistics Unit, Department of Learning, Informatics, Management and Ethics (LIME), Karolinska Institutet, for their statistical consultation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Kamprad Family Foundation in Sweden (20180057). Additional funding was awarded by the Swedish Research Council (2017-02768); the Swedish Council for Health, Working Life and Welfare (FORTE) (2013–2104); the H2020 Marie Sklodowska Curie Actions–Innovative Training Networks, H2020-MSCA-ITN-2015, (676265); the Swiss Alzheimer Association; the Swiss Occupational Therapy Association; and the Social Science Humanities Research Council (SSHRC) Institutional Grant, Canada.
Ethical Approval
This research was granted ethical approval by the Office of Research Ethics at Simon Fraser University (2017s0052) for the Canadian sample, the Regional Board of Research Ethics (2015/77-31-5) for the Swedish sample, the Commission cantonale d'éthique de la recherche sur l'être humain in Lausanne (protocol 452/15) for the Swiss sample, and the Health Research Authority (IRAS project ID: 215654, REC reference: 17/SW/0091) for the UK sample.