
Abstract
Keywords
Introduction
Residents in long term care settings are often considered frail and thus typically experience a rapid decline in all spheres of health. Many factors can explain these declines, but one is excessive amounts of sedentary behaviour (DiPietro, 2001). Sedentary behaviour composes a large proportion of daily time, especially in long term care settings 89% (Lee et al., 2020), and is defined as a prolonged bout of time spent in a sitting or reclined posture (Pate et al., 2008). Spending such a large amount of time sedentary is concerning, as it is associated with undesirable health conditions, a decline in functional abilities, and increased mortality risk among aging adults (Copeland et al., 2017; Rosenberg et al., 2016). Recent attempts to reduced sedentary time in community-dwelling aging adults have proven successful to improve functional benefits (Chastin et al., 2014; Lewis et al., 2016). Such interventions in long term care settings have not been explored yet. In this setting, such interventions may present additional benefits but also additional challenges as greater frailty and higher level of cognitive impairment are reported in these settings (Ellard et al., 2014).
To our knowledge, no intervention has attempted to reduce sitting time in long term care settings. In a recent study conducted by our group in a long-term care setting concluded that 89 % of the day was spent performing sedentary activities (Lee et al., 2020).
Given the high prevalence of sitting time in long term care settings and the association of sedentary behaviour with functional abilities, it is important to explore strategies to reduce sitting time in this setting. This study was conducted in an attempt to gain insight into the feasibility to stand with a population who spends a large portion of their day sitting. Furthermore, this pilot study was conducted to determine sample size for future trials and understand if participants, long-term care facilities and family members would accept this novel intervention. The specific objectives of this pilot study were to assess the recruitment, attendance to the intervention and to explore the potential functional outcomes.
Methods
Study Setting
This study took place in a long-term care facility between May-September 2018. The selected home was a long-term care home with 24-hour care and approximately 218 beds.
Sample Size
There was no minimum sample size, because this was a pilot study and therefore exploratory in nature. Recruitment was stopped to complete the trial before of the summer 2018. Participants were suggested from staff due to the varying cognitive abilities based on inclusion/exclusion criteria.
Participants
To be eligible for the study participants had to:
Have the status of independent transfer, transfer with or without assistance, based on a classification performed by the province (WorkSafeNB, 2017).
Provide consent or had a power of attorney agree on their behalf to participate in the study.
Be able to maintain a standing position for a minimum of five consecutive minutes while being supervised (walkers were accepted)
Exclusion Criteria
Exclusion criteria included if the long-term care staff deemed a resident would not be safe and may fall by participating. The criterion was recommended and confirmed by nursing staff from the long-term care home.
Recruitment
Potential participants were informed of the study from the long-term care rehabilitation staff. If a resident expressed interest in participating, an approval for participation was obtained by the rehabilitation team to ensure safety. Also, the requirement of an assent form was discussed with the long-term care nurses. If an assent form was needed, the Clinical Research Coordinator at the nursing home, not related to the proposed study, contacted families to inform them of the study and acquire approval. If the participant was able to consent, the research assistant reviewed the consent form with the participant and obtained written consent. Potential participants had the opportunity to discuss their involvement with their family members or the staff before deciding. Once the appropriate paperwork had been received, participants conducted baseline testing prior to the 10-week intervention. Participants were not permitted to stand prior to assent/consent and pretesting.
Intervention
For 10 weeks, participants gather in small groups (4–8 people) to participate in planned and supervised standing sessions. During the sessions, two portable tables were temporary installed as a point of gathering while standing. Attendance of participants were collected at each session. The goal was to have each participant standing position for 10 minutes per session, three times per day, 4 days per week (Monday, Wednesday, Friday, and Sunday). The total time offered per week was 120 minutes. The volume of standing time was based on information from previous research at this home, from the long term care staff, and by the current literature (Fitzsimons et al., 2013). Participants were allowed to take breaks if needed during the 10 minutes period with a maximum of three breaks.
For each standing session research assistants went to the various facility floors to assist the residents to take a standing position and to supervise the session. The start times were approximately 8:30 am, 1:00 pm, and 5:30 pm. During these sessions, there were activities to keep the residents entertained such as jokes of the day, group discussion and topic of the day (e.g., interest for summer festivals, usage of cellular phones for young adults).
Finally, to reduce risk of falls or injury, a Steady Mate was used with high risk residents if it was recommended by a staff. A Steady Mate is an elevated walker with wheels underneath. It allows participants to be caught by support belts when walking or standing if needed.
Outcomes and Measurements
Attendance
The main outcome was attendance at the 10-week intervention to reduce sitting time. To be counted as attending the session a resident had to come to the session and attempt to stand at least once. Percentage attendance was calculated as follow.

Sedentary behaviour
Sitting time was measured by an ActivPAL the week prior to and the last week of the intervention for each participant. The ActivPAL was taped with Tegaderm tape to the resident’s leg, mid-thigh on the front of the body, for seven consecutive days (Taraldsen et al., 2011). This device measured sitting and upright time, the number of daily transfers as well as the number of steps taken. The minimum wear time for recording valid information for sitting time with aging adults is 4 days, 10 hours per day (Aguilar-Farias et al., 2014). If an ActivPAL appeared non-valid based on these criteria, the ActivPAL data was excluded from the analysis.
Functional outcomes
Walking speed was measured prior to the intervention by the research staff using the 10-meter walk test (Kempen et al., 2011). This was completed with or without the use of the Steady Mate based if needed. Two trials were completed, and the average of the two times was recorded. Beginning in a standing position participant were asked to walk as quickly and safely as possible from start to finish without assistance. To increase safety, the test was done along a railed hallway. This test is often used in populations with a decline in mobility and is sensitive to functional decline (Kempen et al., 2011). The minimal clinically important difference (MCID) for walking speed is 0.1 m/sec (Bohannon & Glenney, 2014). Participants were categorized as reaching this change or not.
The chair stand test was completed prior to the intervention by the research staff to asses lower body strength, power and functional abilities. The chair stand test involves starting in a seated position with arms across chest, and moving from a seated to standing position as many times as possible within a 30 second time limit (Reid & Fielding, 2012).
Quadriceps strength was measured prior to the intervention by the research staff using the MicroFET2, a hand-held dynamometer, which is considered industry standard by Hogan Scientific (Pro Healthcare Products, 2016). This device records the force exerted on the device during quadriceps extension when applied against the leg. For this test, residents were seated and asked to extend against the MicroFET2 was held in place by the research assistant. The process was then repeated with the other quadricep. Handheld dynamometers with a standardized measurement protocol can obtain reliable lower limb strength values, even from novice testers (Wang et al., 2002).
Participant characteristics
Participant characteristics were obtained from the long-term care records after receiving ethics approval. Characteristics were age, height, weight, body mass index (BMI) and transfer status. The mobility device used was indicated on their file, such as a cane, walker, or wheelchair. Once recruited, participants were classified by their transfer statuses: independent transfer group (transfer from sit to stand on their own with or without a walker or cane), assisted transfer group (require staff assistance to transfer), and those in the dependent group require mechanical and staff assistance to transfer (WorkSafeNB, 2017).
Data analysis
Descriptive data are reported for all measured outcomes using median and inter-quartile range (25–75th). Pre-post change in ActivPAL data for sitting time (hours /day), steps (per day) upright time (hours/day), sit to stand (#/day), and physical function for walking speed (m/s), quadriceps strength (kg), and 30 second chair stand (#), were tested via Wilcoxon singed-rank tests. For variable that were measured over multiple timepoints (e.g., attendance including time of day (i.e., morning, afternoon, evening), day of week, and time standing per week) a one-way repeated measures ANOVA were used. Mauchly’s test was used to test for sphericity, and a Greenhouse-Geisser correction was applied as necessary. When a significant main effect was detected, Bonferroni Post-Hoc tests were run to identify differences between time points. Mann-Whitney U test and Chi-square tests were conducted to determine if personal characteristics were different between the groups (i.e., meeting or not the MCID for outcomes).
Results
Descriptive statistics for the participants who started the intervention are presented in Table 1. The group was predominately female (n = 17, 60.7%) and had a body mass index (BMI) of 26.5 kg/m2. The median age of the sample was 82.7 years and the majority of participants were able to consent for themselves (57.2%). Based on transfer status, the majority of the sample was independent, and 32.1% of them were ambulating with a wheelchair.
Participant Characteristics.

Note. Data shown as median (Interquartiles (IQR-25–75th) or N (%).
Figure 1 displays the process of recruiting participants as well as drop out of participants. Out of the beds available in the long-term care setting, the staff selected units of the long-term care setting to implement the intervention based on the need and potential interest of the residents. Staff recommended 41 residents to participate from a total of 80 potential residents for the study. Of these, 42.8% required an assent form. Ten residents recommended by the long-term care staff could not participate because a family member refused because of fear of falls (N = 4), because they believed their loved one would not be interested (N = 4) or themselves were not interested (N = 2). The 31 remaining participants were recruited. Three of these participants never started the intervention, as they shown no interest when the program started. Therefore, a total of 28 participants were enrolled. During the study, two participants left due to a lack of interest, and two due to illness. Twenty-four participants that completed the entire study. Of these 24, a sub sample of 13 had valid ActivPAL at both pre and post evaluation. Data related to physical function was analyzed for all participants (N = 24).
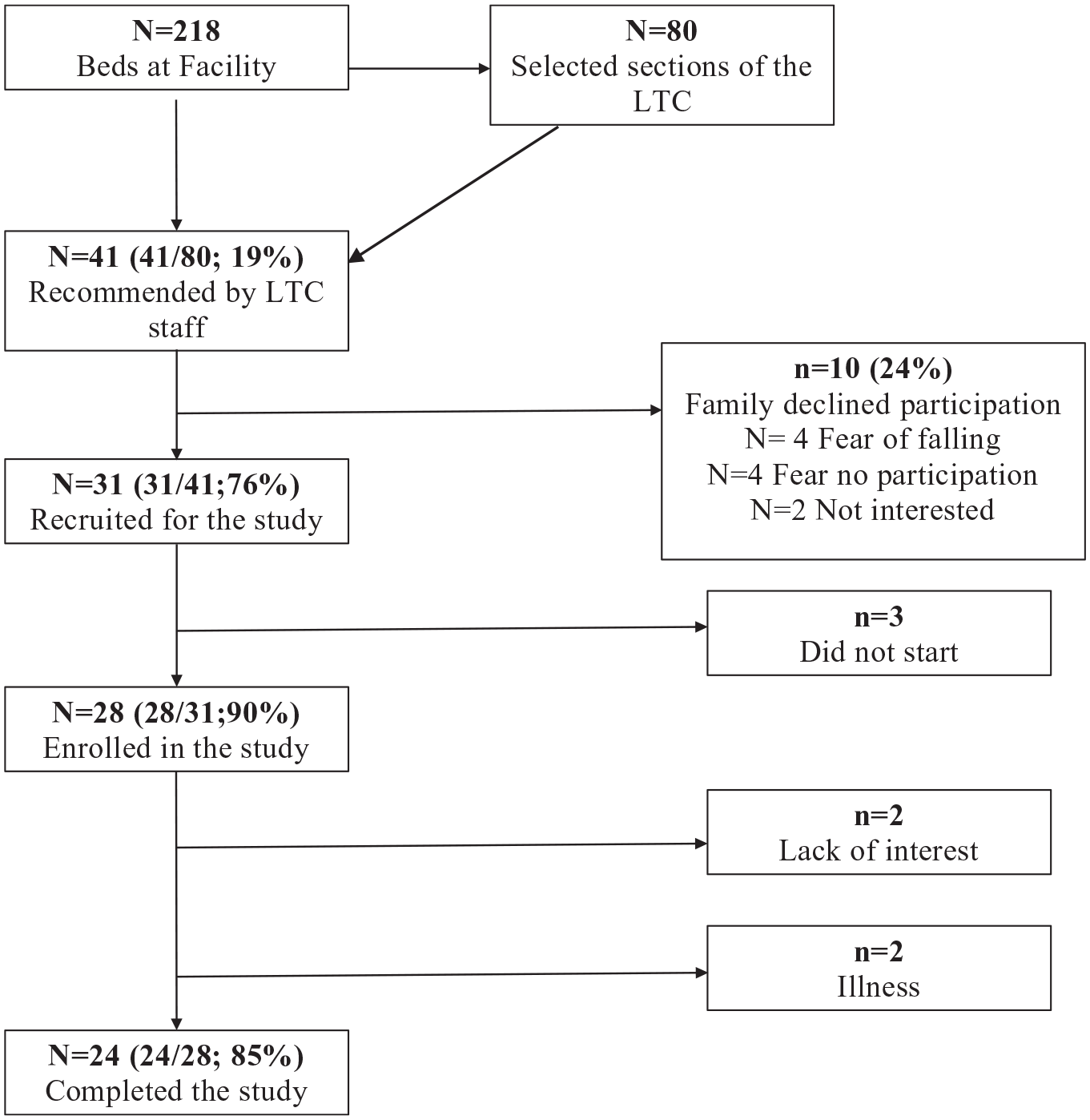
Participant flow chart.
Thirteen participants who completed the intervention wore ActivPALs pre and post-study. Reasons to not have ActivPAL data (11/24) included: the equipment irritating their skin (n = 1), their condition resulted in them being forgetful and frightened by the ActivPAL (n = 4), they did not meet the valid wear days criteria (more than 4 days) (n = 6). Participants who did not wear the ActivPAL at follow-up were in typically in an older age range and most required an assent form to participate in the study; p < .03.
Attendance Outcomes
Figures 1 to 3 present information on attendance of the participants during the study in terms of time of day (Figure 1), day of the week (Figure 2), time standing per week (Figure 3). On average participants attended 35% of the sessions (38 sessions out of 108), attended four times per week (out of 12) and spent an average of 45 minutes standing per week. When standing, the average time per session was 10.66 minutes. There was a significant main effect of time of day on participant attendance p = .01. Morning sessions (M = 15.96, SE = 1.66) were more highly attented than lunch sessions (M = 11.79, SE = 1.32), p = .02, and evening sessions (M = 7.04, SE = 1.3) [Wlik’s Lambda p < .01; F = 17.95; p = .01]. There was also a significant main effect of day of the week on participant attendance [Wlik’s Lambda p < .01; F = 28.34; p = .01). Post-hoc analysis showed no difference in attendance between Monday (M = 11.96, SE = 1.28) Wednesday (M = 12.04, SE = 1.35), or Friday (M = 10.8, SE = 1.23) attendance. However, attendance was significantly reduced on Sunday (M = 7.38, SE = 1.22), when compared to the other days (Figure 4; p = .01). There was a significant main effect of week on the overall (p = .03). However, post-hoc analysis found this difference only existed between week 1 (M = 5.33, SE = 0.58) and week 7 (M = 3.54, SE = 0.56), p = .03. There was no effect of week of participation on time spent standing (p = .22).

Average attendance by time of day.

Average attendance by day.
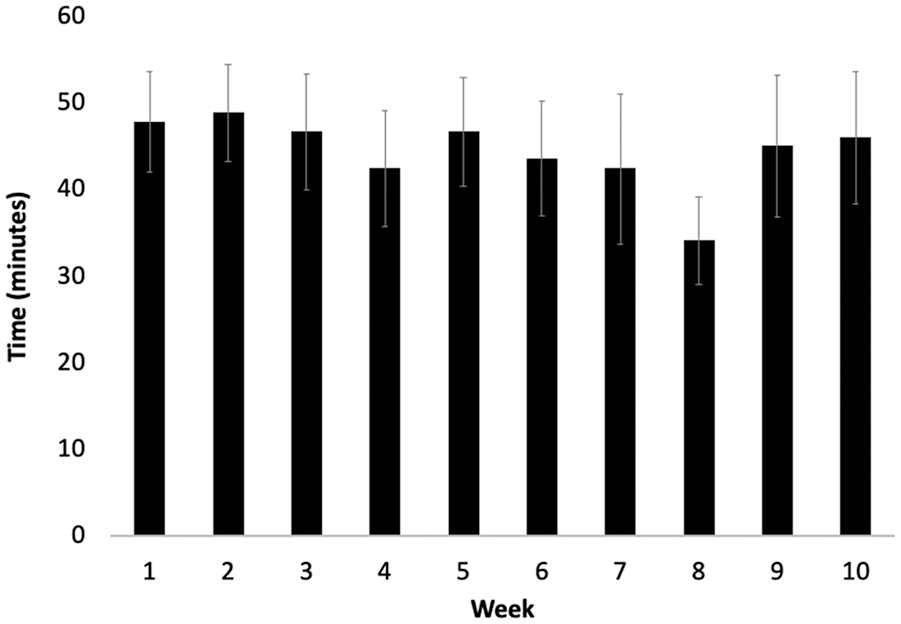
Average time standing during the intervention.
Exploratory Outcomes
Table 2 depicts the results of pre- and post-tests for those who completed the intervention. Surprisingly, the sitting time increased significantly (p = .03), the number of steps decreased significantly (p = .01) and the number of sit to stand movements also decreased significantly (p = .05). No significant improvement was observed in the median value of the functional tests with the exception of the 30-second chair stand test that improved for a median of three (p < .05).
Results of pre- and post-tests by completers (N = 24).
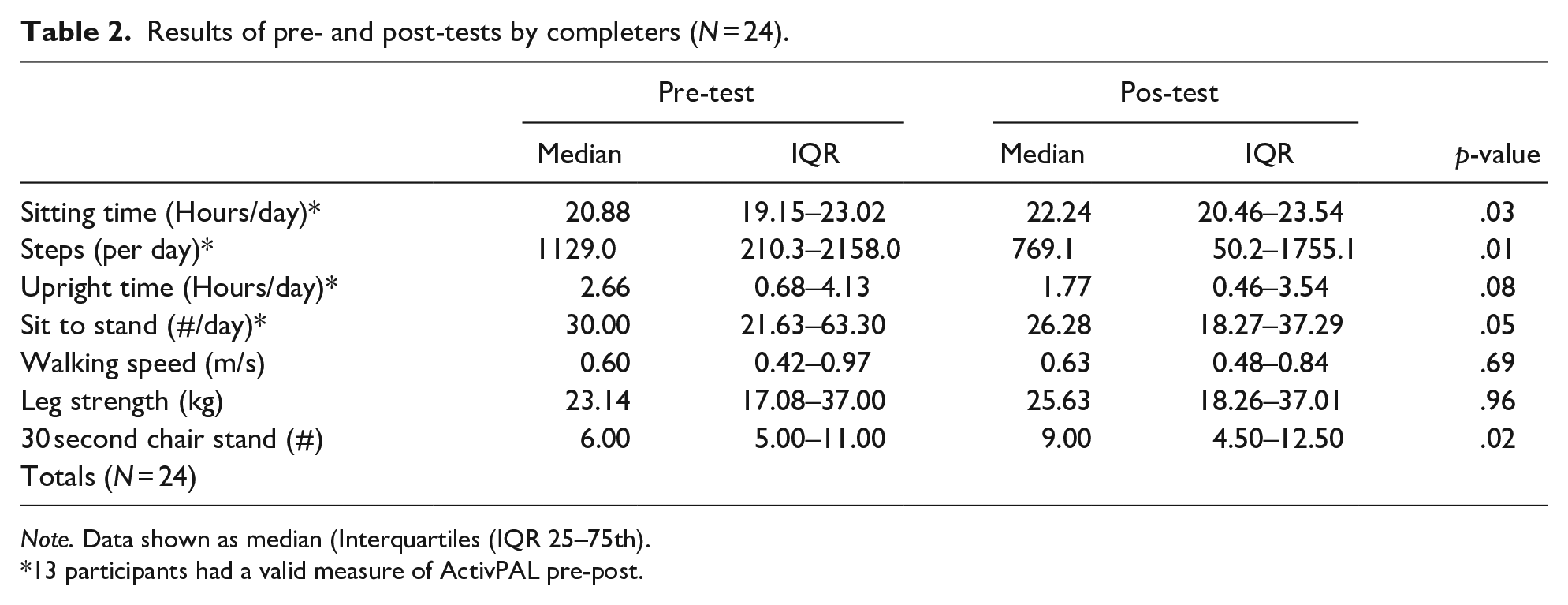
Note. Data shown as median (Interquartiles (IQR 25–75th).
13 participants had a valid measure of ActivPAL pre-post.
Despite that no significant improvement was observed for walking speed, eight of the participants improved their walking speed above the clinical minimal important difference of 0.1 m/sec (Bohannon & Glenney, 2014).
Discussion
The main objective of this study was to assess the attendance of the proposed intervention to reduce sitting time in a long-term care setting, and to explore the potential functional benefits. On average, participants attended 35% of the sessions offered (38/108), averaged four sessions per week and spent an average of 45 minutes upright per week during treatment sessions. This represents about 11.25 minutes per active day, but this average was higher when excluding Sundays and evenings. The attendance was at its highest during the morning session compared with the afternoon and evening session. Weekdays were more attended compared with Sundays. The second objective was to explore the potential functional benefits. There was a significant improvement in the 30 second chair stand test, and despite the fact that no significant improvement was observed on the quadricep strength and the walking speed, eight participants improved their walking speed above the clinical minimal important difference. Due to the small sample size, these results are interesting but need to be carefully interpret.
Perhaps 5 days per week only offering morning and afternoon sessions should be offered in the future. Doing so, the average time standing could increase to 62 minutes per week based on our data. Currently there are no standing trials in long term care settings reporting attendance with aging adults. Other studies in the literature with similar recruitment (N = 27) have shown a greater attendance and total standing minutes when receiving a daily intervention, and used personal goals (Lewis et al., 2016). It is possible that the sample was less likely to attend because of greater health issues or the fact that this study’s sample was older than typical community dwelling samples aiming to reduce sitting time through an intervention (Copeland et al., 2017). Another reason that could explain the difference in attendance could be the fact that the sample needed to stand on a schedule and standing time in the community is often self-reported (Kallings et al., 2009). Finally, the cognitive state of participants was unclear as 41.7% of participants needed a power of attorney to sign assent for them.
Even if walking speed did not improve significantly, it is possible that this is due to a type II error because of the small the sample size, sample variation, or that the time standing was not sufficient to improve significantly. In fact, Rosenberg et al. (2016) observed that for every overall decrease in 60 minutes of measured sedentary time, aging adults in retirement communities improved their 400 m walk test by 21 seconds, which is a clinically meaningful difference. The participants stood on average 45 minutes per week but were a slightly lower level of physical functioning. Therefore, it may be possible to capture more improvements in physical function with other tests, and if participants were able to increase the volume of weekly standing.
Despite the intervention, participants did not decrease their sitting time, as noted when analyzing the ActiPAL data; contrarily, it increased significantly by a median of 82 minutes per day. This is shocking at first glance but may be explained by looking further into the results of the program. The ideal situation would have been a decrease in sitting time of 120 minutes per week due to the intervention or an average of 17 minutes per day. In other words, the time standing as part of the intervention could lead to, at the most, a decrease in sitting time of 16.8 minutes in a day; down to 1236 minutes total sitting time per day. This means that the intervention did not affect enough time of their week to give it the opportunity to be significant.
Although it is now clearer why residents could not significantly reduce their sitting time, it is still unclear why it significantly increased. It is possible that long term care staff may have reduced the number of times they offered to stand or walk participants that were in the study, as the staff knew these residents were already offered to stand for the research. Additionally, it is also possible residents may have declined other opportunities to stand or walk as they knew that they may stand with us. Perhaps residents increased sitting time on their own as it is known that mood and activity level vary considerably from day to day in this population (DiPietro, 2001) or with the progression of their illnesses. Due to the variability of this setting, future studies should attempt to ensure participants continue typical daily activities during the study.
Lastly, it is important to note that this intervention had success in gathering aging adults in long term care settings to conduct standing sessions. Moreover, there were no falls or adverse events and the staff as well as the family members were encouraging and supportive. Therefore, this intervention appears safe and well-accepted.
Limitations
There were several limitations noted in this study. The first being the variability observed in outcomes related to the small sample size, as well as the lack of control group. Another limitation is the inclusion of many long-term care residents who are considered independent. Staff at the long-term facility care suggested participants that they believed could do the intervention, not based on who would benefit the most from the intervention.
There were also limitations for using the ActivPAL, even if considered the gold standard. The device was small, which was an asset for comfort, but also made it easy to misplace. This has also resulted in residents throwing out devices due to size and forgetting to use it. This resulted in only 13 of the 24 participants having ActivPAL data.
Aging and illness were limitations as some participants had to leave the study due to illness or the progression of their disease. Holidays as well as unexpected closures were also a limitation as participants could not attend. Another limitation was the lack of acceptance from some staff. Some staff and family members were non-supportive or fearful of residents standing. This could be resolved with proper education of the purpose of the project, as well as the safety procedures in place.
Conclusion
As part of the study, we were able to gather information that may help future studies involving aging adults in long term care settings with the goal of reducing sitting time. Information such as most attended time of day, most attended days, and the assurance of safety was gathered. The participants showed increased attendance on weekdays over weekends, and morning session over other sessions and the morning and lunch sessions over evening sessions. It would be helpful to have activity staff assist in bringing residents to the standing locations. It would also be beneficial for their activities to be scheduled at different times than the intervention, to prevent conflicts. Future studies could also take advantage of the gathering for sedentary activities to have the participants stand before or after that activity. It would also be helpful to have the staff dress the participants first so they can attend the morning session.
Even if attendance was lower than expected, it could be improved with the feedback that was received. Functional benefits are possible and would be worth testing with the appropriate sample size and study design. Because of the considerable amount of time that aging adults in long term care settings spend sitting, it is important to continue research in this area and to build on the proposed strategy in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.