
Abstract
Introduction
Definition and Relevance of the Issue
Self-neglect has been defined as “The inability (intentional or non intentional) to maintain socially and culturally accepted standards of self-care” (Gibbons, Lauder, & Ludwick, 2006, p. 16). These authors consider that a person may self-neglect either intentionally or due to a lack of ability. However, a number of other institutions, such as the National Center on Elder Abuse (2017), determine self-neglect as nonintentional. This institution defines elder self-neglect as . . . the behavior of an elderly person that threatens his/her own health and safety. Self-neglect generally manifests itself in an older person as a refusal or failure to provide himself/herself with adequate food, water, clothing, shelter, personal hygiene, medication (when indicated), and safety precautions. (National Center on Elder Abuse, 2017)
This research study shares the perspective proposed by Gibbons et al. (2006) because to help both groups of people, it is first necessary to detect the two different types of situations. Intervention varies greatly from one case to another; however, an initial contact with a professional is always necessary.
Self-neglect should be considered as a significant social health care problem due to its prevalence rates and the serious consequences that can result. Available prevalence data vary. In the United States, self-neglect is reported to have a 9% prevalence rate (persons aged 65 and older; Day & McCarthy, 2018). Data from Europe suggest that, in Scotland, the prevalence rates (all ages) vary from 166 to 211 per 100,000 people (Lauder & Roxburgh, 2012), whereas in Ireland, data from a retrospective review suggested that the prevalence rate for self-neglect (persons aged 18 and older) is 142 per 100,000 people (Day, Mulcahy, & Leahy-Warren, 2016). In Spain, there are no population-based studies on self-neglect. There are only partial data, such as a study in Madrid reporting that self-neglect was the primary type (27%) of elder abuse case (persons aged 65 and older) reported to the Servicio de Asistencia Municipal de Urgencia y Rescate (SAMUR)-Madrid Citizen Protection Emergency Service between January and May 2008 (Serrano et al., 2009). In the United States, self-neglect has also been the primary type (41.9%) of cases reported to Adult Protective Services (Dong, 2017).
Self-neglect can seriously affect the health of elders and increases the risk of hospitalization and mortality (Dong, Simon, & Evans, 2012). Moreover, it is important to consider that elders who are unable to perform tasks to cover their basic everyday needs and to ensure their own safety may negatively affect and even endanger their neighbors and family. For example, inappropriate use of an electric heater may result in a fire (Day, Mulcahy, Leahy-Warren, & Downey, 2015), or hoarded material provides a breeding ground for rodents or insects, resulting in infestation (Andersen, Raffin-Bouchal, & Marcy-Edwards, 2013). This should result in increasing concern about self-neglect among policy makers and the public.
Risk Factors
Self-neglect results from complex interactions between medical, psychological, and social risk factors (Lee & Kim, 2014). In terms of medical and psychological issues, the factors that are currently under the greatest degree of study are cognitive impairment and depressive disorders (Band-Winterstein, Doron, & Naim, 2012; Burnett et al., 2006; Day, Leahy-Warren & McCarthy, 2013; Snowdon, Shah, & Halliday, 2007). Numerous researchers point to dementia as a risk factor, although the possible failure of executive function is also currently a focus of study (Dyer, Goodwin, Pickens, Burnett, & Kelly, 2007; Hildebrand, Taylor, & Bradway, 2014).
One of the risk factors for which we currently have the most data is the reduction in social resources (Burnett et al., 2006; Dyer et al., 2007). Research studies demonstrate that self-neglecting elders reduce their participation in social activities and have a reduced informal social support network.
Band-Winterstein et al. (2012) state that self-neglect does not appear suddenly but rather that the individuals who suffer from these problems have already presented self-neglecting behavior at previous periods in their life and, above all, during times of crisis.
Most recent self-neglect research studies highlight the need to analyze the heterogeneity of the problem. Burnett et al. (2014) have identified four subtypes of self-neglect. These authors manifest their interest in studying whether the variables that bring about the situation of self-neglect are different for each type of self-neglect.
Detection
Given the severity of the problem, we need to improve detection methods. Health and social service professionals are well situated to detect the presence of elder self-neglect that requires comprehensive assessments for health, welfare, and safety (Dong, 2017). Based on previous research (Band-Winterstein et al., 2012; Dong et al., 2012; Dyer et al., 2006; Hurley, Scallan, Johnson, & De La Harpe, 2000; Nathanson, 2009; Turner, Hochschild, Burnett, Zulfiqar, & Dyer, 2012), we consider that the following points demonstrate key areas in the assessment of elder self-neglect:
deterioration of personal hygiene,
lack of self-health care,
deterioration of home and possessions,
difficulty understanding their situation, and
difficulty accepting help.
In Spain, the older adult protection policy is now beginning to unfold. Self-neglect mandatory reporting laws for health care professionals do not exist. The primary care social service teams and, in some communities, social service team specialists in working with older adults are responsible for managing self-neglect cases. Nevertheless, the lack of studies on self-neglect in the Spanish population and the lack of validated screening instruments have made it difficult for professionals to detect.
Study Objectives
The main objective of this research study was to provide information relevant for detecting potential self-neglecting elders in a Spanish population. To achieve this main objective, we compared the characteristics of these individuals and their environment with those of a group of elders at increased risk of domestic abuse and of another group of elders who receive presumed adequate treatment (AT) from their trust relationships. The rationale for this comparison is that these are the other two types of situations in which community-dwelling vulnerable older people can be living according to the type of treatment provided by caregivers, family members, or next of kin.
We defined adequate treatment as a situation in which the actions of caregivers, family members, or next of kin guaranteed the elder’s physical, psychological, and/or social well-being. The concept of risk of domestic abuse included the definitions of both inadequate treatment and abuse cases. We defined inadequate treatment as a situation in which the actions of the caregivers, next of kin, or family members did not guarantee the elder’s physical, psychological, and/or social well-being. Abuse was considered the most extreme form of inadequate treatment, as it presented the most danger to the quality of life of the elder and violated his or her rights to the greatest extent. For the purposes of this study, we used the definitions of domestic abuse proposed by the National Research Council (2003) and the definitions provided by the National Center on Elder Abuse (2017) for the different classifications of domestic abuse (physical, psychological, financial exploitation, neglect, abandonment, and sexual abuse) and for self-neglect. The only difference was that the definition of self-neglect of our study did not exclude situations in which older people with no cognitive decline/impairment, who, therefore, understood the consequences of their decisions, made a conscious and voluntary decision to engage in acts that threatened their health or safety as a matter of personal choice.
To attain the main objective of this study, we also tested whether the indicators considered by Burnett et al. (2014) as common to all types of self-neglect (difficulties in performing daily life activities, instrumental activities, and medical problems due to inadequate care) demonstrated a high predictive value in the study sample.
Method
Participants
This study analyzed the records of 269 social services clients located in 46 local councils of Majorca (Spain). The total number of records included 94 men and 175 women. Their age ranged from 63 to 101 years, with an average age of 81.22 years (SD = 7.75 years). The age range of the male group was 64 to 95 years, with an average age of 78.55 years (SD = 7.34 years). The age range of the female group was 63 to 101 years, with an average age of 82.65 years (SD = 7.61 years). The age difference was statistically significant, with the female group presenting a higher average, t(219) = 4.26, p < .001.
Social service professionals selected cases from their own active caseload, and categorized them as AT cases, presumed inadequate treatment cases, at increased risk of domestic abuse cases, and at increased risk of self-neglect (SN), taking into account the definitions exposed above related to the presumed quality of treatment provided by caregivers, family members, or next of kin, or presumed self-neglect.
For the purposes of conducting statistical analyses, we formed three distinct groups: AT (n = 90), at increased risk of abuse (RA; n = 132), and at SN (n = 47). The RA group includes the cases of inadequate treatment and domestic abuse. There was no significant age difference between the elders in the three groups, F(2, 266) = 2.47, p = .086. The average age was 82.46 years (SD = 7.84 years) for the AT group, 81.06 years (SD = 7.71 years) for the increased risk of domestic abuse group, and 79.43 years (SD = 7.44 years) for the SN group.
Regarding gender, the AT group consisted of 32 men and 58 women. The increased risk of domestic abuse group comprised 43 men and 89 women. Finally, the SN group was made up of 28 women and 19 men.
Procedure
The study was carried out in several phases:
Presentation: The study was presented to the Institute of Social and Sports Services of the Insular Council of Majorca that approved its implementation. Thereupon, the study was presented to the social service professionals. A total of 46 professionals (40 social workers and six psychologists) from the social services teams of 32 municipalities in Majorca were interested and confirmed their voluntary participation.
Training course: The professionals attended a training course on definitions of domestic abuse and self-neglect, how to distinguish between self-neglect and abuse, and how to detect domestic abuse and self-neglect.
Participant selection: The social service professionals selected and categorized the study cases from among their existing client base. They used a nonprobability sampling method: the quota sampling. The population was divided into subgroups based on the established criteria for sample selection ([a] AT cases, presumed inadequate treatment cases, at increased risk of domestic abuse cases, and at SN cases; [b] age; [c] sex; and [d] geographical distribution), and cases were selected on the basis of a given proportion.
Cases assessment: The social service professionals completed an information collection protocol to assess the analyzed variables. Whenever possible, different professionals working in the same social service team made the selection than those who completed the protocol. Informed consent was not requested. The regulations for the use of data in investigations were followed. Assigning identification codes to all the participants and dissociating their personal identification data from the data utilized by social service professionals guaranteed the duty of professional secrecy and the participants’ anonymity.
Instruments
We created a data collection protocol for use by the professionals. The protocol included both open and closed questions as well as a series of items to be evaluated on a 5-point response scale according to the professional’s degree of agreement with each statement (1 = strongly disagree, 2 = slightly disagree, 3 = slightly agree, 4 = strongly agree, 5 = completely agree). The professionals based their assessments on the existing reports on each case, as all cases were social services clients. Data for the following variables were collected:
Sociodemographic information of the elder: The professionals provided information on the elder’s age, sex, and marital status.
Mental health and behavioral problems: On a scale from 1 to 5, the professionals assessed whether the elder presented the following problems: mental health issues, behavioral problems, problems with alcohol or other drugs, signs of cognitive impairment, and occurrences of self-neglecting behavior in previous periods of their lives.
Economic situation of the elder: The professionals evaluated on a 5-point scale whether the financial income of the elder was sufficient to maintain an adequate quality of life.
Living situation of the elder: The professionals provided information about whether the elder was the homeowner and whether he or she lived with anyone else.
Type of informal support received: The professionals provided information on a 5-point scale assessing whether the elder’s contact with family members, friends, and neighbors was less frequent than needed to attend to his or her needs, and the level of the elder’s satisfaction with the relationships maintained with family members, friends, and other next of kin.
Type of formal support received: Using a 5-point scale, the professionals assessed whether the individual was reluctant to receive help, whether he or she received sufficient social care to cover his or her basic needs, and whether he or she received the health care that he or she required.
Characteristics of the home: The professionals assessed on a 5-point scale the state of the elder’s home.
Hygiene and personal care: Using a 5-point scale, the professionals evaluated the physical appearance and hygiene of the elder.
Ability to care for own health: The professionals used a 5-point scale to assess the lack of necessary medical aids (e.g., eyeglasses, hearing aids, dentures), the quality of eating habits maintained by the elders, their ability to comply with medical treatment, and their ability to ask for help when required.
Type of treatment: An evaluation of the elder made by the social worker from social services was used. The cases had been analyzed by and were known to the professional for a long time (M = 34 months, SD = 40.43 months). The professionals classified the elders according to whether they considered their cases to be AT, presumed inadequate treatment, at increased risk of domestic abuse (indicating physical abuse, psychological abuse, neglect, financial exploitation, abandonment, or sexual abuse), and at SN cases.
The scales used were created for this investigation. The internal consistency of the 5-point scales was analyzed and an alpha coefficient of .93 was obtained. The degree of interrater agreement could be analyzed for 14 cases that were assessed independently by two different professionals. The results showed a significant correlation, rs(14) = .99, p < .001.
There was no instrument for assessing the risk of abuse validated with the Spanish population; also, there is no gold standard to measure adequate treatment, inappropriate treatment, abuse, or self-neglect. For this reason, the criterion used to allocate the participants to these groups was the professionals’ expert judgment on whether the treatment received by the elder guaranteed his or her well-being and the aforementioned definitions of domestic abuse and self-neglect. It is not possible to provide data on the validity of this measurement.
Data Analyses
We used the Kruskal–Wallis test to analyze the differences that may have existed between the elders with AT, the elders at RA, and the elders at SN groups in the analyzed variables (personal hygiene and appearance, hygiene conditions and habitability of the home, health care problems, professional and informal support, functional state and mental health problems). We used post hoc analysis with the Mann–Whitney U test to observe between which group differences would be produced. In addition, we applied Bonferroni correction to avoid an increase in the global probability of yielding results from multiple comparisons, with an established significance level of p ≤ .017. Furthermore, we analyzed dichotomous variables using the Cochran–Mantel–Haenszel test.
We employed multinomial logistic regression with the aim of studying the predictive power of the variables highlighted by Burnett et al. (2014) as suitable indicators for all types of self-neglect.
Results
There were no detected cases of suspected sexual abuse. The analysis found a significant relationship between marital status and type of treatment received, χ2(2, 267) = 6.25, p = .044. In 15% of the cases, the professionals indicated that the elder at SN did not present any form of cognitive impairment or mental health problems. This may suggest that the detected cases were situations of intentional and nonintentional self-neglect (Gibbons et al., 2006).
The SN group had significantly higher scores than the AT and RA groups for all variables indicating deterioration in hygiene and personal appearance (Table 1). Medium and high effect sizes were observed in the first case; however, in the second case, the effect sizes were low. The SN group had significantly higher scores than those in the AT group with regard to the lack of adequate hygiene conditions and habitability problems in the home. The effect sizes were medium and high. In comparison with the RA group, the SN group also had significantly higher scores for hygiene conditions of the home, yet the effect size was small.
Deterioration of Personal Hygiene and Appearance, Hygiene Conditions, and Habitability of the Home.
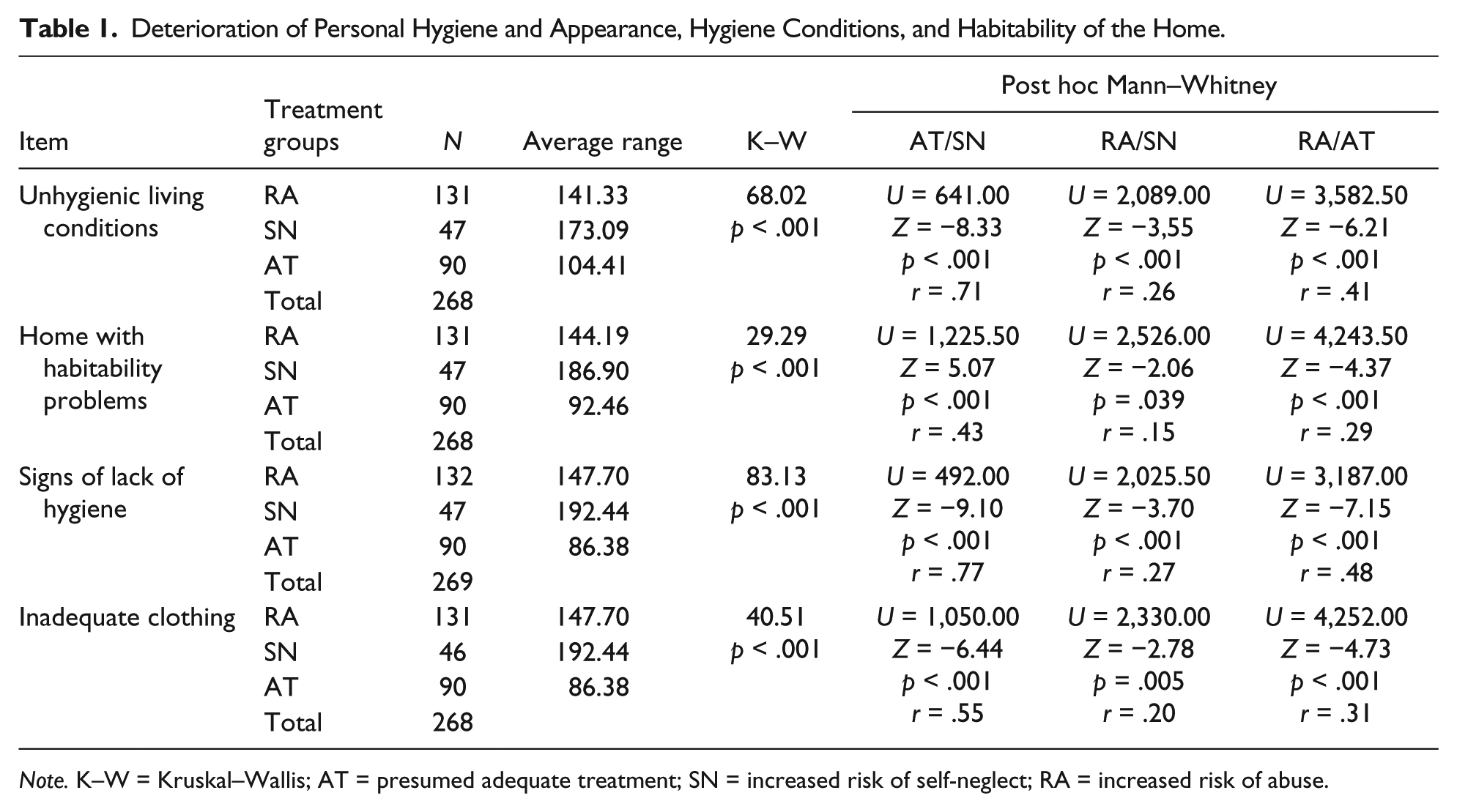
Note. K–W = Kruskal–Wallis; AT = presumed adequate treatment; SN = increased risk of self-neglect; RA = increased risk of abuse.
Table 2 contains the obtained results for the variables related to health and health care problems. The SN group had significantly higher scores than the AT group for all variables. There was no difference from the RA group with regard to the lack of necessary medical aids (e.g., eyeglasses, hearing aids, dentures), health problems due to inadequate treatment, or untreated medical problems. The SN group also had significantly higher scores than the other groups for the rest of the variables related to health and health care problems. Medium and high effect sizes were found in the differences obtained between the SN and AT groups, whereas the effect sizes were small in the comparisons with the RA group.
Health and Health Care Problems.
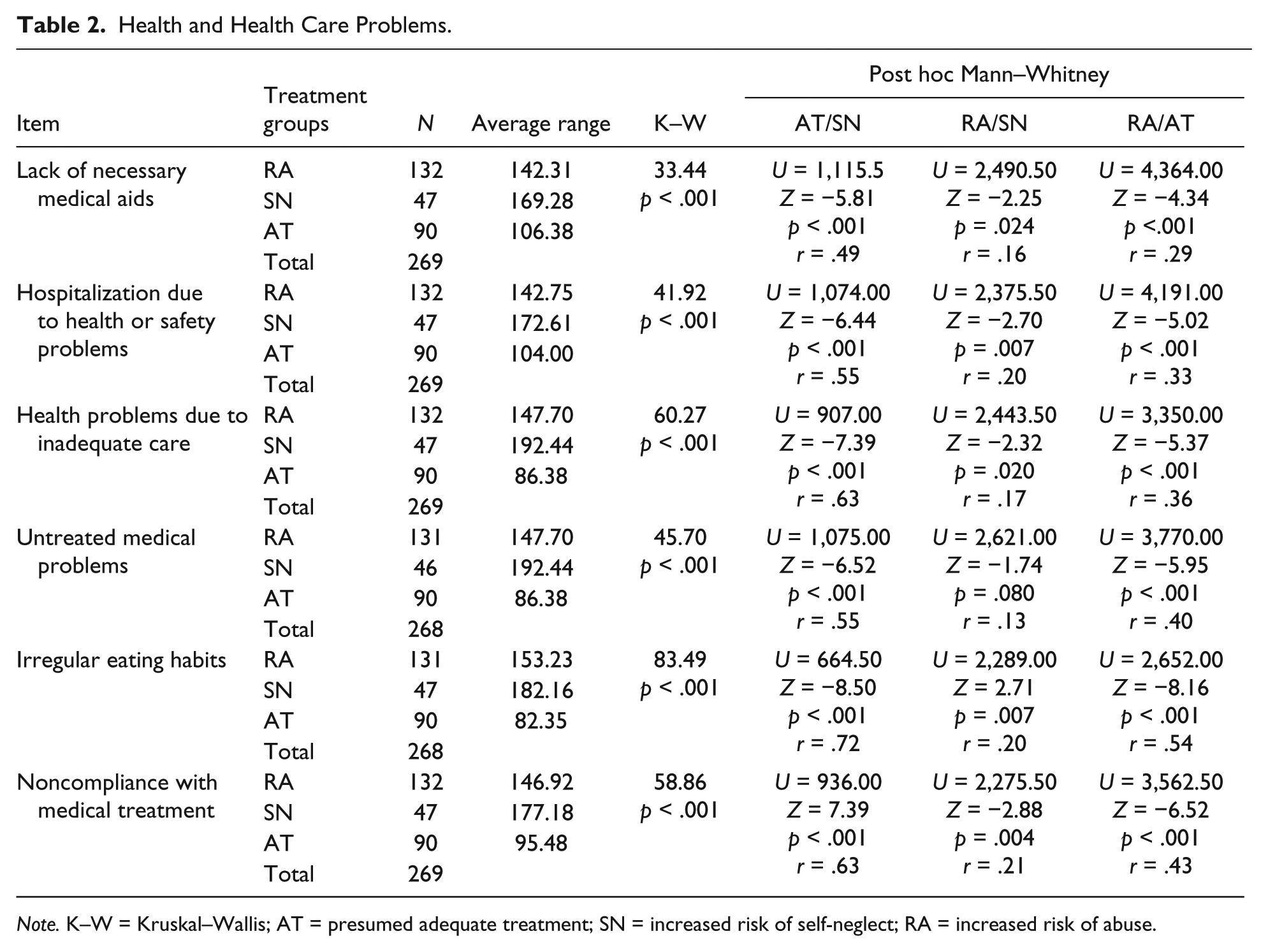
Note. K–W = Kruskal–Wallis; AT = presumed adequate treatment; SN = increased risk of self-neglect; RA = increased risk of abuse.
The Kruskal–Wallis contrast test showed statistically significant differences between the groups when assessing the elders’ expectations of their situation, χ2(2, 268) = 72.98, p < .001. The SN group presented more unrealistic expectations than the AT group (U = 436.500, Z = −8.18, p < .001, r = .42) and the RA group (U = 1,391.00, Z = −5.66, p < .001, r = .42).
The analyses found a connection between receiving professional help and being at increased risk of self-neglecting conduct, χ2(2, 267) = 28.38, p < .001. Analysis of the differences between the three groups demonstrated that 93% of the individuals in the AT group received professional help, as opposed to 54.3% in the SN group and 78.6% in the RA group.
As shown in Table 3, the assessments made by the professionals regarding the characteristics of professional and informal help received by the elders were different in the majority of the studied variables. This was observed in the SN, RA, and AT groups.
Characteristics of Those Who Received Professional and Informal Support.
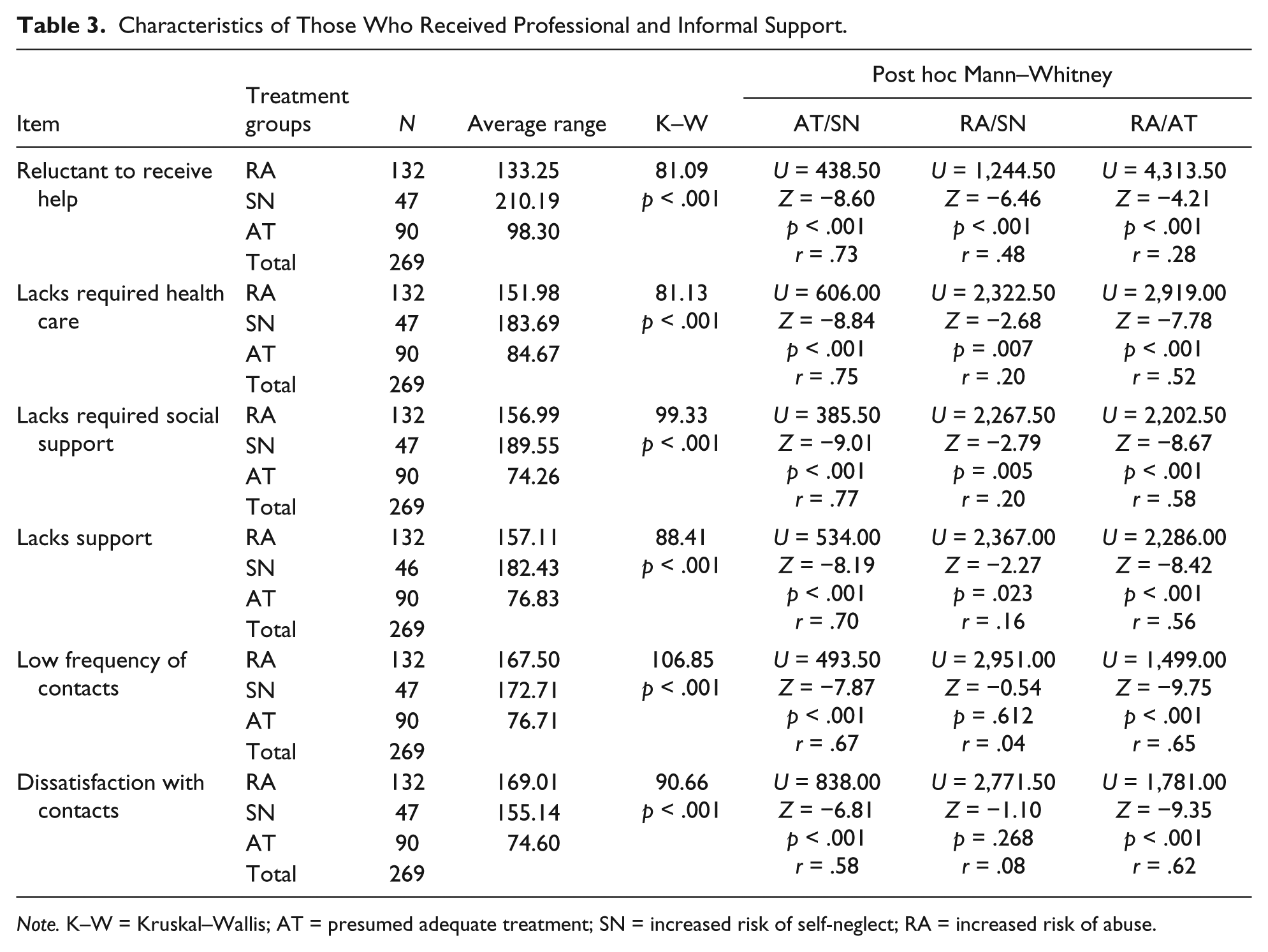
Note. K–W = Kruskal–Wallis; AT = presumed adequate treatment; SN = increased risk of self-neglect; RA = increased risk of abuse.
The results demonstrated differences among the three groups in terms of the person’s reluctance to receive help. The SN group presented most difficulties in this area. High effect sizes were found in the comparison of the SN and AT groups, and medium effect sizes were found in the comparison with the RA group. Despite this observation, it is important to highlight that 14.8% of elders at SN did not demonstrate this difficulty.
The professionals estimated that there were differences in the manner in which the social and health care needs of the elders were being covered. The SN group presented significantly greater difficulty in these aspects than the RA and AT groups. The effect sizes were high and small, respectively.
With regard to informal support, the SN group had a significantly greater lack of support, a significantly lower contact frequency, and a higher dissatisfaction than the AT group. The effect sizes for these variables were high. However, there were no significant differences found between the SN and RA groups in any of the three variables.
In addition, the three groups demonstrated differences in the degree of family conflicts. The Kruskal–Wallis contrast test displayed statistically significant differences between the groups, χ2(2, 268) = 101.45, p < .001. Post hoc analysis with the Mann–Whitney test presented significant differences between the SN and AT groups (U = 809.50, Z = −6.99, p < .001, r = .59) but not between the SN and RA groups (U = 2,717.50, Z = −1.08, p < .027, r = .08). The RA group demonstrated the most troublesome social relationships.
The results demonstrated a significant relationship between living alone and the type of treatment received, χ2(2, 267) = 44.239, p < .001. Sixty-six percent of people at SN lived alone compared with 16.7% of elders at RA and 27.4% of people receiving AT.
Regarding the functional state and mental health problems presented by the elders, in Table 4, we can observe that the SN group had fewer difficulties than the RA group when performing daily life activities and instrumental activities. However, the effect sizes were small. There were no observed differences in these aspects when compared with the AT groups.
Functional State and Mental Health Problems.

Note. K–W = Kruskal–Wallis; AT = presumed adequate treatment; SN = increased risk of self-neglect; RA = increased risk of abuse.
The SN group presented more behavioral and mental health problems than the AT group. The effect sizes were medium. However, there were no differences in these aspects when compared with the RA group. There were no differences between the groups in terms of alcohol and drug consumption problems. With regard to the degree of cognitive impairment, the SN group could not be differentiated from the other two groups. However, there was a difference observed between the AT and RA groups, with the latter presenting a greater degree of cognitive impairment according to the assessments made by the professionals. Nevertheless, the effect size was small.
The results demonstrated an association between the type of treatment and the presence of self-neglecting behavior in previous periods of life. Post hoc analysis demonstrated significantly higher scores in the SN group than in the other two groups. The effect sizes in the SN group were higher than those in the AT group and medium in comparison with those in the RA group.
In terms of the financial situation of the elder, the Kruskal–Wallis test showed statistically significant differences between the groups, χ2(2, 268) = 17.62, p < .001. The AT group presented less financial difficulty than the SN group (U = 1,374.50, Z = −4.15, p < .001, r = .35). There were no significant differences observed between the RA and SN groups (U = 2,793.00, Z = −1.15, p < .250).
We applied multinomial logistic regression analysis to test the predictive value of the indicators proposed by Burnett et al. (2014). The results obtained are displayed in Table 5. The variables related to the functional assessment of the elder (assessment of daily activities and functional abilities) were insignificant. The variance percentage explained by the dependent variable with predictive variables was 42% (R2 de Nagelkerke = .42).
Equation Variables.

Note. LL = lower limit; UL = upper limit; RA = increased risk of abuse; DLA = daily life activities; IA = instrumental activities; RA = increased risk of abuse; SN = increased risk of self-neglect; CI = confidence interval.
The variables enabled us to predict AT, correctly classifying 91.1% of cases. However, many errors were made when predicting cases of at RA (only predicting 58.3% of cases) and cases at SN (23.4%).
Discussion
The aim of this study was to provide information relevant for detecting potential self-neglecting elders in a Spanish population. The results for the possible existence of intentional and unintentional self-neglect cases confirmed the findings of other studies (Burnett et al., 2014; Gibbons et al., 2006) in terms of the heterogeneity of those who self-neglect and the possible existence of different types of self-neglect with diverse etiologies.
The components previously described as key to defining self-neglecting people proved to be effective in differentiating between the AT group and the RA group. The elders at SN demonstrated more difficulties than the other two groups in terms of hygiene and personal appearance, living conditions, and availability of social and health care assistance. Furthermore, they had more unrealistic expectations about their situation and were more reluctant to receive help.
In addition, the results coincided with the findings of other research in highlighting the lack of social support for people who self-neglect (Burnett et al., 2006; Dyer et al., 2007). The elders at SN received less professional support than elders with AT, and elders at RA. Only 54.3% of the elders at SN received some sort of professional help, as opposed to 93% of AT cases and 78.6% of elders at RA. The informal social support received by the elders at SN also differed from that received by the elders in the presumed adequate care group. These results are in line with the findings of Burnett et al. (2014).
Living alone and having presented self-neglecting behavior in previous periods of life have been shown to be risk factors for self-neglect (Ban-Winstertein et al., 2012; National Research Council, 2003). The results of our study showed a statistically significant relationship between living alone and the type of treatment received, and a higher percentage of people living alone in the group of elders at SN than in the groups of elders with AT and elders at RA. Our results also found that elders at SN were the ones who obtained significantly higher scores in the presence of self-neglecting behavior in previous periods of life.
Our findings produced no significant differences between elders at SN and people at RA in terms of the degree of severity of behavioral and mental health problems, or financial difficulties. As shown in previous studies, these variables could be risk factors for both situations (Dyer et al., 2007; National Research Council, 2003). Similarly, there were no significant differences observed between people at SN and people at RA in three of the indicators related to health problems and health care: lack of necessary medical aids (e.g., eyeglasses, hearing aids, dentures), health problems due to inadequate care, and untreated medical problems. The existence of risk factors and indicators that are common to both situations can complicate the detection of specific cases of SN and RA, especially when the latter form of abuse is neglect.
As mentioned in the “Introduction” section, an extremely important current line of research (Dyer et al., 2007) focuses on studying how difficulties in performing daily life activities and instrumental activities, together with other variables, can bring about the onset of self-neglect. This investigation found no significant differences between elders at SN and elders receiving AT. However, people at SN did present fewer difficulties than people at RA. Furthermore, it is important to note that these variables did not prove to be predictors of receiving AT, being at RA, or being at SN. These results could be explained due to the lack of support enabling elders to continue living in their homes. The individuals suffering the most severe degree of self-neglect and presenting the highest level of difficulty in their everyday life may have been referred to residential services or may have had a family member take charge of their care. In these cases, the elders would have passed to either being adequate treated or being at risk of abuse.
The obtained results partially support the proposal of Burnett et al. (2014) regarding the indicators that are common to all types of self-neglect. We have already highlighted the poor predictive value of the variables related to difficulties in conducting daily life activities and instrumental activities. The other three variables applied to the equation (health problems due to inadequate care, noncompliance with medical treatment, and hospitalization due to health or safety problems) obtained significant results. The predictive model derived from the results of the multinomial logistic regression analysis demonstrated that it could correctly classify those elders who received AT to a relative degree of precision. However, it made many predictive errors when classifying elders at RA and, especially, elders at SN.
According to the obtained results, professionals should suspect self-neglect when they observe signs of deterioration in cleanliness and personal appearance or hygiene condition, poor living conditions, admissions to the hospital due to health problems or failure to maintain personal safety, noncompliance with prescribed medical treatment, or inadequate eating habits. In addition, self-neglect is associated with people who lack the social and health care assistance that they need and who are reluctant to receive help.
The results of this study highlight the need for further research into the risk indicators and factors that help detect situations of self-neglect. Future research studies must consider that self-neglect cases are heterogeneous in character and may present a diverse set of etiologies and indicators. Likewise, because different risk of abuse situations share the same common aspects, it is necessary to uncover variables that are specifically related to self-neglecting behavior. Our results also show that it is essential to study the difficulties that professionals face when trying to get self-neglecting people to accept help, and how self-neglecting people perceive the professional help that is offered to them. Moreover, it would be interesting to conduct longitudinal studies to observe the transformation of the support networks of these people according to the deterioration or improvement of their situation.
Limitations of the Study
It is necessary to take into account the limitations of the study, which are mainly due to the type and size of the sample. The reduced number of at SN cases used in this study, and the fact that social service teams selected all the elders included in the study mean that the observed data are not representative of all elders at SN. The same could be said with regard to the cases of AT and at RA. The sample size could have influenced the fact that certain risk factors were underrepresented, such as problems with alcohol abuse and other drugs, which have a low prevalence in the population. Furthermore, the small sample size may have influenced the fact that no cases of sexual abuse were found. The small sample size was due to several factors, such as the number of older people who were clients of social services in Majorca. However, professionals’ barriers to detecting cases of domestic abuse and cases of self-neglect (lack of training, for example) and the overload of work due to collaborating on the study were also relevant factors in explaining the small sample size. In our community, there are no adult protection services, which makes intervention and research difficult. Due to all these reasons, it would be interesting to compare the results obtained in this research study with those obtained from larger samples that are more representative of the general population. Another important limitation of the research was not being able to use validated instruments for the Spanish population. In addition, using a retrospective design prevents from establishing temporal sequences between events.
Despite the indicated limitations, we consider this study to be valuable, as it is one of the first investigations of self-neglect conducted in Spain. Moreover, our research could contribute toward the development of future research lines and ultimately help improve the quality of life of elders.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.