
Abstract
As unpaid family caregiving of older adults becomes increasingly prevalent, it is imperative to understand how family caregivers are socialized and how they understand the caregiving role. This PRISMA-ScR-based scoping review examines the published literature between 1995–2019 on the socialization of potential and current unpaid family caregivers of older adults. Of 4,599 publications identified, 47 were included. Three perspectives of socialization were identified: (1) role acculturation; (2) role negotiation and identification; and (3) specialized role learning. The findings show how socialization involves different contexts (e.g., cultures), imperatives for action (e.g., circumstances), socialization agents (e.g., family), processes (e.g., modeling), and internal (e.g., normalization) and external (e.g., identification) consequences for caregivers. Future research could fruitfully explore how caregivers manage key turning points within the socialization process, disengage from the caregiving role, and negotiate the socialization and individualization processes within diverse cultural and funding contexts.
Introduction
The United Nations Population Division (2019) reports that “there were 703 million persons aged 65 years or over in the world in 2019,” projecting that this number will double to 1.5 billion in 2050, such that “one in six people in the world will be aged 65 years or over” (p. 1). Due to reduced mobility, age-related illnesses, or chronic conditions, many of these older adults will require some form of medical care, social support, and assistance with the activities of daily living. The high cost and limited capacity of formal long-term residential care combined with older adults’ desire to remain at home has led many countries to encourage home-based care. Such care often relies on the efforts of unpaid caregivers who provide “help to older family members, friends and people in their social network, living inside or outside their household” (OECD, 2019, p. 232). This review uses the term family caregiver to designate these varied unpaid caregiver-care recipient relationships, where family refers to nuclear and extended family members as well as “families of choice.”
A comprehensive understanding of family caregiver socialization is needed to support these individuals in managing increasingly complex caregiving responsibilities. Extant literature provides a kaleidoscopic view of family caregiving. Some studies examine structural factors such as formal care availability and welfare state orientation to predict if family members will adopt a caregiver role (e.g., Haberkern & Szydlik, 2010). Others focus on the burden, benefits, and experiences of family caregivers already engaged in caring for an older adult across diverse cultural contexts (e.g., Schultz et al., 2020). Further, sometimes family caregivers providing care do not identify with the caregiving role (Eifert et al., 2015; Molyneaux et al., 2011). Hence, this scoping review focuses on how potential and actual caregivers develop understandings of the caregiver role.
We use Jablin’s (2001) definition of socialization to better understand how individuals learn who should care and how they recognize, accept, and enact the role within a social unit. Socialization has two dimensions (Jablin, 2001): process and content. The first, processual dimension identifies four key phases of role acquisition and performance. The anticipatory phase describes how potential caregivers learn about the caregiver role and who should perform it. The encounter phase refers to moments where caregivers’ emergent role expectations bump up against daily realities. Metamorphosis encompasses caregivers’ adaptation to role expectations and ability to seed changes within the social unit by tailoring the role to suit their personal preferences. Disengagement involves caregivers reducing their cognitive, emotional, and physical engagement, although not necessarily exiting the caregiving role. Jablin’s second dimension, which focuses on the content of socialization, examines how individuals and families (best) learn what they need to know in order to carry out the new role.
Keeping this definition in mind, our review questions how the research literature conceptualizes the socialization of family caregivers who care for older adults, examines how distinctive perspectives of socialization frame caregiving, and identifies future research directions. The following sections detail our method, report findings, and discuss the contributions and gaps in the family caregiver socialization literature.
Method
Research Design
By mapping out a complex, heterogeneous evidence base, scoping reviews enable us to summarize, classify, and more effectively disseminate research findings. Our review adopted Arksey and O’Malley’s (2005) five-step methodological framework, which is reported following the PRISMA-ScR as a rigorous way to report choices (Tricco et al., 2018). PRISMA-ScR is a checklist of items that increases “understanding of relevant terminology, core concepts, and key items to report for scoping reviews” (Tricco et al., p. 467).
Data Collection
In order to document how socialization was conceptualized, we searched for texts written between 1995 and 2019 across five social sciences databases: PsychInfo, Web of Science, Sociological Abstracts, Social Sciences Abstracts, and Communication Abstracts (most recent search: 12/12/2019). Our final search strategy used synonyms for each key term: (socialization OR socialisation OR learning OR support) AND (family care* OR kin care* OR informal care* OR unpaid care*) AND (elder* home-care OR community based elder* care). Online Appendix A explains how we developed the search strategy. We also searched the reference lists of retained texts and consulted an expert in caregiving for older adults.
Selecting Relevant Literature
The first round used a priori selection criteria, which reduced the number of results of texts from 4,599 to 124 results (see Figure 1). We excluded texts that did not (1) focus on unpaid family caregivers (e.g., spouses, siblings, children, extended family, neighbors, friends, volunteers, religious groups) regardless of type or amount of care or health condition; (2) discuss home-based care of older adults; (3) explicitly address caregiver socialization; or were (4) in-progress studies. Using the first criterion, we excluded literature about paid professionals. The second allowed us to exclude studies about formal care contexts (e.g., hospitals, assisted living, palliative care units, nursing homes, respite care, and day centers), as well as analyses of social policy, national care regimes, and care not centered on older adults. The third criterion, caregiver socialization, was interpreted broadly to include studies that dealt with anticipatory socialization or reported on vocational learning about care (e.g., training programs, web-based interventions, and support groups). Because the review examined the process of becoming a caregiver, we excluded outcome-based studies about caregiver burden; caregivers’ health outcomes and quality of life; and caregiver experiences not focused on learning, training, or knowledge acquisition.
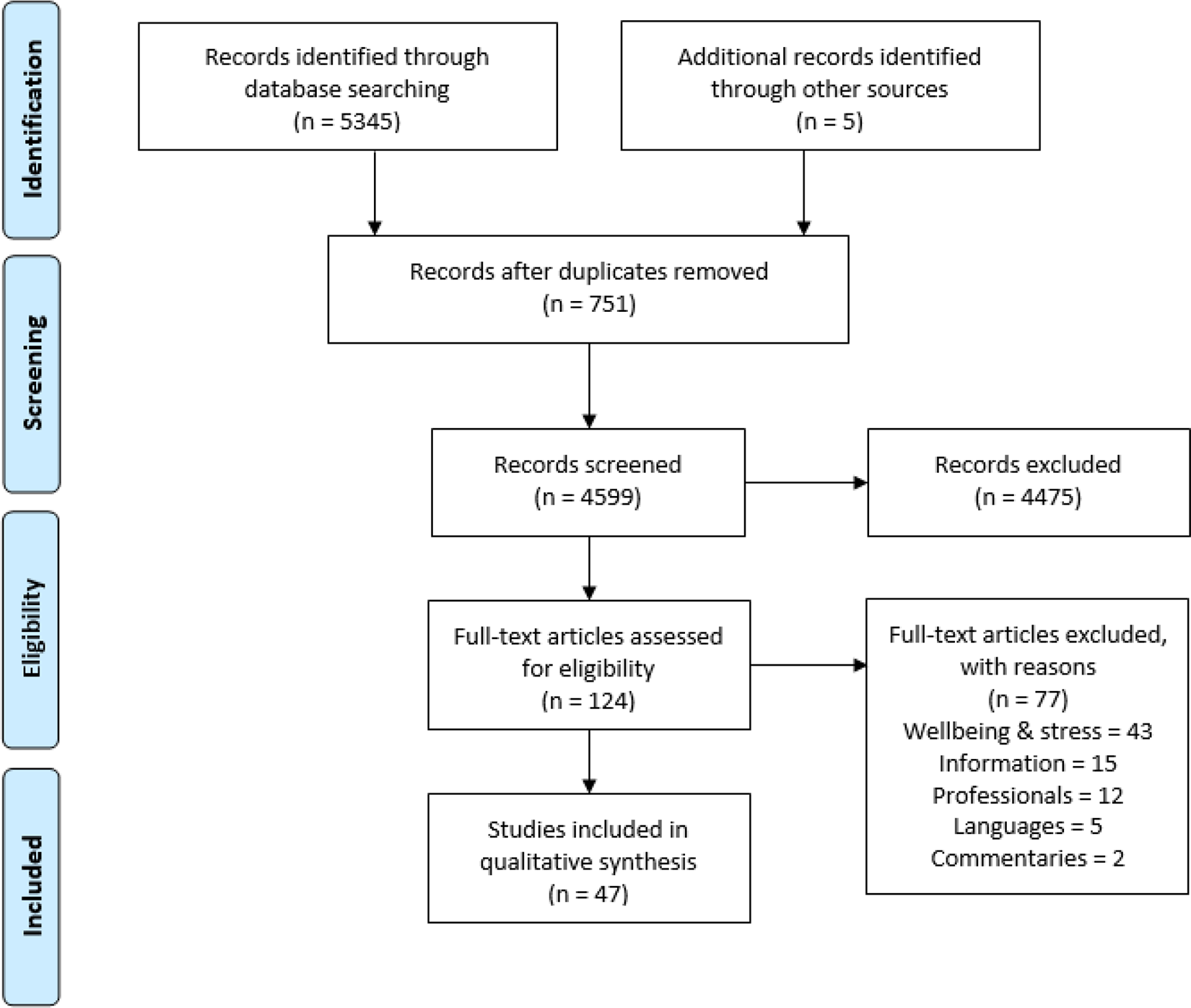
Prisma flow diagram.
During the second screening round, we refined criteria further. We excluded texts where socialization focused on caregivers’ wellbeing, stress, or needs rather than on how caregivers recognized or learned to enact the caregiving role. We also distinguished between information and knowledge acquisition, excluding articles that only mentioned information availability. We excluded articles about professionals supporting caregivers by integrating paid caregivers into home-based care, rather than developing interventions that targeted caregivers. Although we sought articles representing a wide range of cultural contexts, we excluded studies not written in English, French, or Spanish, languages the authors read fluently, as well as commentaries, editorials, and book reviews.
Literature Analysis
First, using an Excel spreadsheet, team members independently extracted content from retained studies to document (1) definitions of socialization; (2) organization of care/division of labor; (3) family structure; (4) family and cultural assumptions about caregiving; (5) family caregivers who were socialized; (6) key findings; (7) study method; (8) type and number of participants; and, in the case of intervention-based studies, (9) program and training methodology. Second, after discussing emerging patterns, thematic analysis of extracted content was conducted: The first author coded extracted content that focused on definitions and descriptions of the socialization process using NVivo, generating 186 distinct nodes or first-level codes of one to five words. Nodes were grouped into larger second-level codes or overarching categories.
Third, team discussions team led to a distribution of second-level codes into three distinctive perspectives on caregiver socialization. However, we noted our first analysis was more descriptive than analytical, so the first and second authors returned to the Excel spreadsheet and re-coded the explicit and implicit definitions of socialization. Focusing on definitions rather than empirical manifestations of socialization helped to identify the distinctive dimensions of socialization across our literature base: contexts, imperatives for action, agents of socialization, core processes, and internal and external changes brought about by socialization (see Table 1).
Three Perspectives of Family Caregiver Socialization.
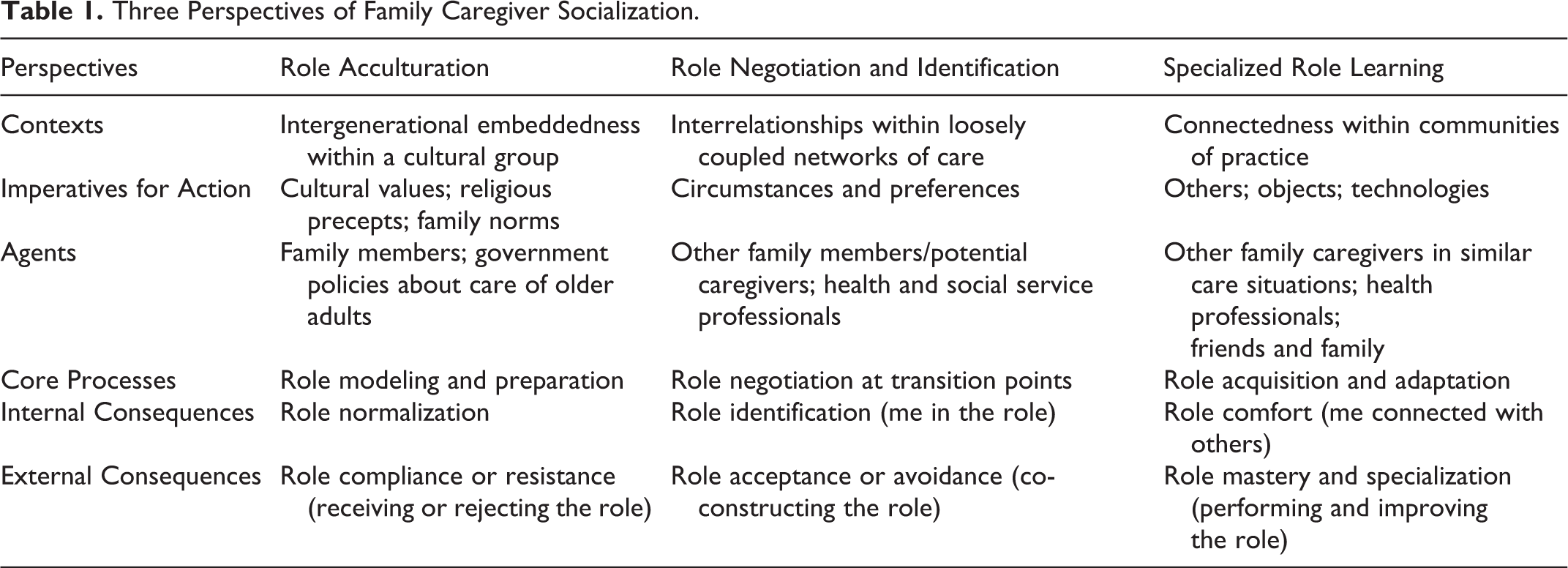
We present the three perspectives of socialization as role acculturation, role negotiation and identification, and specialized role learning in the following section.
Socialization as Role Acculturation
Role acculturation included 19 studies representing socialization as implicit and intergenerationally-transmitted. These were case studies (Au et al., 2012; Bryant & Lim, 2012; Chan et al., 2012; Hsueh et al., 2008; Mendez-Luck et al., 2017; Nance et al., 2018; Sasat, 1998; Wallhagen & Yamamoto-Mitani, 2006; Wu, 2009); ethnographies (Crosato et al., 2007; Gerdner et al., 2007; Holroyd, 2001: Jenike, 2002; McAuley, 2001; Sánchez-Ayéndez, 1998); phenomenological analyses (Faronbi et al., 2019 Pharr et al., 2014); grounded theory (Mendez-Luck et al., 2016); and textual analysis (Abdugafurova et al., 2017) studies.
The contexts of socialization for these studies highlight caregivers’ embeddedness within religious belief systems (Muslim, Christian) or purportedly collective cultural groups or locations (Hong Kong, Taiwan, Japan, Thailand, Mexico, Puerto Rico, Nigeria, Indigenous Canadian communities, all-Black towns and migrant Latinx communities in the United States), where members’ identities and practices derive primarily from their connection to the wider group. In addition to other family members, socialization agents include government agencies that, through funding arrangements for care for older adults, structure the range of alternatives available to family caregivers. Holroyd (2001) notes that Hong Kong policy (1965 to early 1990s) encouraged family caregiving by making places in government-funded care homes available only for older adults without children. In all-Black towns in Oklahoma (U.S.), experiences of racial discrimination and lack of external support generated an ethos of community self-reliance that led town members to informally assist older community members (McAuley, 2001).
The imperatives for action center on cultural and religious values that specify gender roles and family norms. In most studies, daughters and daughters-in-law internalized responsibility for caregiving, due to their gender, birth order, or relationship by marriage (Abdugafurova et al., 2017; Au et al., 2012; Jenike, 2002; Sasat, 1998). This is particularly so in Japan where, traditionally, a woman who leaves her maiden family and marries into the family of her husband is obliged to care for her in-laws at home. Although policy changes in Japan in 2000 increased availability of community-based day care for older adults, redefining how care responsibilities were shared between family and community, cultural-legal pressures still reify existing care arrangements (Jenike, 2002). Women across a range of cultural contexts described family caregiving in terms of “social expectedness” and “a cultural imperative” (Walhagen & Yamamoto-Mitani, 2006, p. 69). One Puerto Rican woman said, “My parents and grandparents always told me that the youngest daughter [me] was the one who had to look after the parents when they aged” (Sánchez-Ayéndez, 1998, p. 79). Japanese women took care of “the elderly” because “it was their position (…) as a matter of course (…) something one must follow without question” (Wallhagen & Yamamoto-Mitani, 2006, p. 68), and Indigenous Canadian women “accepted this responsibility because it was unheard of to deny the elderly care” (Crosato et al., 2007, p. 6).
Nance et al.’s (2018) study of male Mexican caregivers demonstrates the pervasiveness of gender norms. As Mexican cultural norms of masculinity imply that a “good” man cares for his family, male Mexican caregivers stated that giving personal care to mothers, wives, or in-laws was not unusual. Yet, while 18 of 21 older male care-recipients in focus groups in one city had their sons caring for them, these participants underlined their expectation that their youngest daughters should be the ones to care. Mendez-Luck et al. (2016) notes that men tend to be “insulated” (p. 468) from caregiving because they are working or are considered ill-suited for care work.
Other imperatives for action are family norms such as familism and the notion of filial piety. Some literature embedded socialization in the concept of familism, which underscores the interconnectedness of extended family (siblings, aunts, uncles, cousins, and in-laws) and creates expectations that family members will care for each other (Mendez-Lucket al., 2016). Other studies explained how the Confucian norm of filial piety leads children to reciprocate their parents’ sacrifices by providing material care and demonstrating obedience, reverence, and respect (Holroyd, 2001). A study of Chinese Australian family caregiving highlights parents’ hierarchical power (e.g., a mother-in-law threatened to starve herself to death if placed in a nursing home) and positions care as reciprocal and cyclical (Bryant & Lim, 2012).
The core processes of socialization begin early and center on role modeling and preparation. For some, roles are assigned at birth (Escandón, 2006). For all, socialization starts early with children observing others providing care (Mendez-Luck et al., 2016). Such role modeling combined with learned cultural values prepares them to take on a family caregiving role. Indeed, Asian American, Hispanic American and African American participants in Pharr et al.’s (2014) focus groups stated that decisions to care for family members arose “naturally” without conscious thought. In only one study were norms imposed rather than learned: Abdugafurova et al.’s (2017) analysis of fatwas (a legal opinion issued by qualified Islamic jurists at a believer’s request) shows that legal decisions reinforced women’s caregiving role. Although the Qur’an commands all Muslims to care for older adults and traditional Islamic law states that care is obligatory for sons, fatwas issued by Islamic legal institutes in Egypt, Central Asia, and the United States framed care of older adults as a “voluntary” activity whereby wives demonstrate their commitment to their marriage.
However, the socialization process also includes the possibility of resistance. Caregivers do not always enact the role in line with dominant cultural frameworks: They may also reinterpret or resist key norms and values. Holroyd (2001) explains that cultural “discourses of obligation are (…) embedded in a complex process of understanding, experience and life circumstances” (p. 1128). Despite the importance of filial piety in Confucian-heritage cultural contexts, some studies document challenges to traditional notions of filial piety. Some adult children vehemently criticized their parents’ belief that they had earned the “right” to receive care (Holroyd, 2001), and adult children caring for a parent with Stage-4 cancer in Hong Kong rejected authoritarian relationships driven by obligation and obedience in favor of reciprocal relationships based on compassion and mutual support (Chan et al., 2012). Another study finds that Taiwanese daughters-in-law who stepped in when other family members stepped back were motivated by affection rather than an obligation to “pay back” the older generation (Wu, 2009; see also Hsueh et al., 2008).
The internal consequences for caregivers who accept caregiving as part of their life trajectory include building resilience and framing problems associated with care as private. African American women in Gerdner et al.’s (2007) study relied on their Christian faith to continue caregiving despite inadequate social support. They expected life to be hard and their faith-inspired resilience, which had “enabled them to endure in the past” (p. 370), socialized them to accept and confront difficulties. Similarly, Hong Kong Chinese caregiving is shaped by the Confucian value of ren, “facing adversity with magnanimity” (Au et al., 2012, p. 1431). Although this value enabled family caregivers to face challenges, cultural norms governing face meant that caregivers avoided “bothering” others or sharing their need for help, because loss of face brought shame and embarrassment to family and self. These strategies risk making care invisible to family members who do not provide care or support the caregiver. In some cases, caregivers participate in creating their own invisibility. A Hong Kong woman caring for her mother at home hid many of the care needs from her husband and instead inveigled her daughters to do the work without telling their father (Holroyd, 2001). Unwittingly, this caregiver socialized her daughters to both provide and to hide care.
The studies show that external consequences of adopting the caregiver role can include a lack of collective resource-sharing, insufficient social support, and even criticism from family members. Faronbi et al.’s (2019) study of Nigerian caregivers indicates that when the extended family system is effective, the entire family provides care, although they assert such collective efforts are uncommon. Indeed, a study of African American caregivers of older adults with chronic confusion shows that family support was not as extensive as outsiders perceived, with half the caregivers reporting no family support (Gerdner et al., 2007). Other studies also document inconsistencies between cultural expectations and actual demonstrations of family support. One such study reports Mexican women caregivers’ frustration at the unequal distribution of caregiving in and across households, which was not aligned with the principles of familism (Mendez-Luck et al., 2016). Despite professed familial solidarity, these women ended up caring alone. Their experience is similar to that of Nigerian caregivers where a spouse exclaimed, “None of his relatives or family members is coming around; I am the only one here” (Faronbi et al., 2019, p. 11). Japanese caregivers also faced a tradition “assigning the total responsibility of care for a frail elderly parent to only one family member, even when there are other members who could share the care burden” (Jenike, 2002, p. 81). For example, as the wife of an eldest son, Mrs. Shimura is obliged to care for her 92-year-old mother-in-law with advanced dementia. Her two unmarried children and sisters-in-law do nothing and have never offered help, with one actively refusing her requests. Furthermore, non-caregiving family members criticize caregivers. The siblings of Puerto Rican women caregivers complained about the quality of care and caregivers’ children grumbled that their parents were unavailable (Sánchez-Ayéndez, 1998). Even grandchildren caring for grandparents were not immune to criticism from their own parents (Wu, 2009).
The fact that various caregivers report they would not wish their children to be socialized as they were suggests the consequences of socialization can be problematic. Caregivers currently caring for parents at home indicated a willingness to receive what they perceived to be inferior care in nursing homes to avoid burdening their own offspring (Mendez-Luck et al., 2017). One Japanese caregiver warned her daughter not to marry an eldest son to avoid caring for her future spouse’s parents (Jenike, 2002).
In sum, socialization as role acculturation shows how potential caregivers learn who is mostly likely to become a caregiver, although they may conform to or resist this role.
Socialization as Role Negotiation and Identification
Role negotiation and identification includes 15 studies that represented socialization as families discussing who would take responsibility for caregiving. The emphasis on interaction between caregivers, families, and health professionals is seen in the nine case studies (Barker, 2002; Burton, 1996; Connidis & Kemp, 2008; Dunér, 2010; Ebenstein, 2005; Egdell, 2012, 2013; Escandón, 2006; Heenan, 2000; O’Connor, 2007; Robinson, 1999; Turner et al., 2016). The remaining studies included longitudinal (Leopold et al., 2014) and narrative (MaloneBeach et al., 2004) studies, and a literature review (Moral-Fernandez et al., 2018).
The contexts of socialization for these studies are networks of family, community, and formal care, characterized by “interlocking pathways” (Burton, 1996, p. 200) where changes in one individual’s pathway cause ripple effects in others’ lives. Other family members (potential caregivers) and health and social care professionals are socialization agents who influence role negotiation and shape understandings of what the care role means.
The imperatives for action, which include circumstances of other potential caregivers and preferences of care recipients, influence the uptake of caregiving roles and care-task distribution (Connidis & Kemp, 2008; Dunér, 2010; Egdell, 2013). Leopold et al.’s (2014) study of 641 U.S. families comprising 2,452 parent-child dyads found that care recipients’ expressed preferences, path dependency (caregiver already provides some care), and existing affective commitment reinforced siblings’ acceptance of the caregiver role. Some siblings avoided caregiving because of external attributes such as competing care demands, geographical distance, and the income and educational attainment that they would forgo or not put to use if they provided care (Connidis & Kemp; Dunér). Other siblings perceived to be more competent and suitable, or available, were assigned the caregiving role (Connidis & Kemp; Egdell; Leopold et al.).
The core processes of role negotiation at various transition points are captured in Escandón’s (2006) three-phase conceptual model of intergenerational caregiving. The first phase of role making, includes role introduction (early-age responsibilities and observation of caregiving) and role reconciliation, which requires role assignment, appropriate support by other family members, and role transition. The second phase of role recognition occurs when caregivers embrace the role, “consciously clarify and interpret messages received, (…) [and] crystallize and personalize the role” (p. 571). The timing of role entry may influence the second and third phase of role execution. Burton’s (1996) study found that “on-time” intergenerational caregiving among African American women (motherhood and grand-motherhood) led them to seamlessly take up responsibilities for the adjacent generation (e.g., great-grandmothers cared for great-great-grandmothers), whereas women who experienced unexpected role transitions refused to provide care. If alternative care options do not exist, caregiving may be an unexpected life event in response to a crisis than a somewhat inevitable career (MaloneBeach et al., 2004).
Role negotiation is evident in Moral-Fernandez et al.’s (2018) qualitative meta-synthesis of the start of caring for a dependent older family member. Transitioning to care generates shock, uncertainty, and confusion when changes in care recipients’ health or others’ (in)ability to care for them unexpectedly propel family into the caregiving role. Frequently, a caregiver “who usually knows only the most central of the requisite role behaviors [must] slowly and sometimes painfully take on responsibilities in a variety of ways” (Escandón, 2006, p. 581). They begin to realize needs before implementing strategies to deal with their new reality by seeking help, reordering family and social relationships, and devising strategies to decrease negative emotions and stress (Moral-Fernandez et al.). Despite the possibility of a difficult transition (Moral-Fernandez et al.), a desire to put up a good front can lead caregivers to not ask for help until they arrive at crisis points that then become “passports” to support not previously accessed (Egdell, 2012, p. 452).
Role negotiation is not always explicit. Barker (2002) found that neighbors or friends may help an older adult with small everyday tasks or more instrumental tasks in short-term casual or bounded relationships. Over time, these may develop into complex committed and/or incorporative care relationships where the neighbor/friend is involved “in the life world of the care recipient” and either they or the care recipient becomes “incorporated into the other’s family nexus” (p. S164). The internal consequences of socialization involve accepting the care role and integrating it within one’s identity (Ebenstein, 2005). Some studies, however, problematize the meanings given to the caregiving role over the lifespan. Rural Northern Irish women caring for parents or in-laws insisted that “all women who have a family are carers; it’s as simple as that. It’s part of family life: I don’t know any women who aren’t carers” (Heenan, 2000, p. 861). Other caregivers justify “doing what you gotta do” (Robinson, 1999) as a natural consequence of their marriage vows (Turner et al., 2016) and frame care work as a natural extension of their existing relational role. A participant in one study explained this difference: In our group nobody ever calls themselves a caregiver (…) I’m taking care of my husband (…) I’m taking care of my mother (…) And even this fellow whose wife is in palliative care (…) he doesn’t refer to himself as Molly’s caregiver. If he does use the term “caregiver” it’s these people he’s hired to take care of Molly. Not him. (O’Connor, 2007, p. 169)
External consequences include positioning of self, care recipient, and care tasks. Positioning oneself as caregiver rather than family member gives people a new set of discursive resources. In O’Connor’s (2007) study, caregivers objectified care recipients by relying on medicalized explanations of problematic behaviors and “routinely positioned their family member as a generic ‘they’ or reverted to more abstract discussions about the ‘Alzheimer’s patient’” (p. 172). In a similar vein, Robinson (1999) adopts a theatrical metaphor to explain how the home becomes a “stage” modified for a new care performance, with the cast starring the family caregiver and the care recipient in a supporting––and implicitly less agentic––role. She describes how, by performing daily care tasks, family caregivers “learn to ‘talk the talk’ and ‘walk the walk’ of the script of a ‘lay nurse’” (pp. 73–74) who has significant knowledge of caregiving and involvement in healthcare decision-making, before eventually embracing and becoming “enmeshed” in the role.
In sum, socialization as role negotiation and identification situates caregivers within an interconnected network of care that can limit and expand their choices. In negotiating transitions, caregivers may identify with the caregiver role or challenge it by locating caregiving as a feature of existing family relationships.
Socialization as Specialized Role Learning
Specialized role learning includes 13 studies, which present socialization as the acquisition of specialized knowledge and practical skill development. The emphasis on caregiver practice, knowledge, and skills in carrying out their role with greater competence and confidence may help to explain the prevalence of intervention design and evaluation (Farran et al., 2003; Guerra et al., 2011; Hanson et al., 2011; Jansson et al., 1998; Mulatilo et al., 2000; Toseland et al., 2001) and program evaluation research design (Bank et al., 2006; Barbabella et al., 2018; Brown et al., 2012). The remainder included case studies (Casado et al., 2015; Lundberg, 2014; Simpson et al., 2018) and a literature review (Aksoydan et al., 2019).
The contexts of socialization highlight the integration into and movement of caregivers across communities of care practice. Within these communities, socialization agents helped caregivers to increase their knowledge and develop role expertise. Agents included other caregivers in similar situations (Aksoydan et al., 2019; Bank et al., 2006; Brown et al., 2012; Ebenstein, 2005; Jansson et al., 1998; Lundberg 2014; Simpson et al., 2018) and health and social service professionals (Farran et al., 2003; Guerra et al., 2011; Hanson et al., 2011; Mulatilo et al., 2000; Toseland et al., 2001).
The imperatives for action center on information, technologies, and people with expertise and experience. Methods include technology-based supports (Barbabella et al., 2018; Lundberg, 2014), telephone support groups (Bank et al., 2006; Farran et al., 2003), and in-person training (Brown et al., 2012; Toseland et al., 2001; Wu, 2009). Most studies, however, adopt an individualistic frame whereby socialization enables primary caregivers to learn to provide better quality care and to cope with and continue carrying out their role. The exceptions were the Portuguese Pro-Families program that aimed to help families adapt to living with a person with dementia (Guerra et al., 2011); the Swedish Circle program where volunteers offered families 4-5 hours of respite care per week (Jansson et al., 1998); and the Samoan caregiving program where community nurses advocated for policy changes to encourage other villagers to provide relief for family caregivers (Mulatilo et al., 2000).
Socialization included in-person and mediated caregiver support groups that offered emotional and informational support (Brown et al., 2012; Guerra et al., 2011; Mulatilo et al., 2000; Toseland et al., 2001). These exchanges of knowledge and experience (Hanson et al., 2011; Jansson et al., 1998; Simpson et al., 2018) allowed caregivers to learn from and teach each other and to value their emerging knowledge. Some caregivers dropped out of support groups because the care recipient did not yet have significant symptoms (Ebenstein, 2005; Guerra et al., 2011) or their situation had changed (e.g., moved into residential care; Bank et al., 2006). Also, caregivers may respond to support groups more at some stages than others during the socialization process. Thus, caregivers acquire specialized knowledge and skills and adapt in response to current, emerging, and expected changes, using just-in-time learning as they go (Casado et al., 2015).
The socialization process involves role acquisition where caregivers observe behaviors, gather new information, watch experts, ask for help and feedback, engage in trial and error, and share experiences with and learn from other caregivers (Barbabella et al., 2018; Farran et al., 2003; Wu, 2009). Thus caregivers can try new ideas, validate that they are doing all they can, and realize they not alone (Farran et al., 2003). Participants can use information from programs to plan ahead for their family members as well as themselves and learn skills that enable them to support end-of-life care, give medications, use equipment, monitor vital signs and manage oxygen, dialysis, and intravenous treatments among other skilled care activities (Brown et al., 2012). One Web-based support program prepared participants for future caregiving needs by reading current caregivers’ “walls” and comments (Barbabella et al., 2018).
The consequences of socialization for caregivers are firstly internal. Here, the caregiver reaches some level of comfort with the role which may manifest as improved emotional self-efficacy, a sense of control in the role and/or of the situation (Guerra et al., 2011), and role satisfaction with the caregiving experience (Brown et al., 2012). Secondly, external consequences center on role mastery (Brown et al.), which may manifest in improved care provision and reflexive practice (Farran et al., 2003). Still, socialization is not always effective in improving caregivers’ care delivery. Aksoydan et al.’s (2019) systematic review of 24 studies notes that training for informal caregivers could but did not always improve care quality with the most effective interventions developing problem-solving techniques, rather than pre-determined strategies. Skilled caregiving comprises complex, well-integrated, and goal-directed behaviors that are developed through practice over time (Farran et al.). Skilled caregivers use a broader repertoire of strategies to deal with difficult behaviors because they can spot potential causes and identify how their actions (de)escalate them (Farran et al.). Socialization as specialized role learning, then, hinges on caregivers’ ability to respond to care recipients’ condition and needs and to reflect on and change their own practice (Farran et al.).
In sum, by fostering caregivers’ skills and knowledge, socialization as specialized role learning expands caregivers’ choices. In learning from other caregivers and health professionals, caregivers participate in (new) communities of practice.
Discussion
This scoping review identifies three distinct perspectives to describe the socialization of family caregivers of older adults. The first positions socialization as role acculturation. Studies document how cultural values, family norms, and government policies “set apart” certain family or community members, usually women, who are assumed to have a “natural” obligation to provide care. Caregiving, then, becomes a predetermined role performance where caregivers are presumed to have little choice but to comply with role expectations. Although cultural messages normalize family caregiving, some family members resist by problematizing traditional cultural norms, especially as values evolve.
This form of assimilative socialization, where the collective acculturates newcomers to assume their roles and prioritize the needs of others, falls squarely within the ambit of Jablin’s (2001) notion of socialization. It tends to make care work invisible to those not actively engaged in assisting older relatives with long-term health needs (Kaplan Daniels, 1987). Many policies maintain that “families are able to care for older relatives at home because individuals are embedded within webs of social relationships (…) which are said to have the potential to provide support and care” (Fast et al., 2004, p. 6). However, latent support networks only develop into active care networks (Egdell) that support both care recipients and caregivers when caregiving is visible and shared (Chiu & Yu, 2002). Unfortunately, the scoping review indicates that without wider family involvement, primary caregivers end up caring alone (Gelman, 2014) and avoid asking for and using external resources such as daycare or home help (Carpentier et al., 2008).
The second perspective describes socialization as role negotiation and identification in contexts where a collective cultural contract cannot be taken for granted. Although age norms, family/generational expectations, and important life course transitions may propel individuals toward or pull them away from a caregiving role, caregivers have more agency at key turning points (e.g., sudden illness of an older relative), either accepting or avoiding the role (Leopold et al., 2014). By privileging what Jablin (2001) termed individualization whereby individuals interpret and/or modify roles in line with their own needs and circumstances, this approach to socialization introduces an element of indeterminacy that is not present in the role acculturation perspective, which insists that roles are reasonably fixed.
This perspective also underlines the importance of interaction not just in deciding who will care but in co-constructing the caregiver identity. Some family members made caregiving more formal, more official, and therefore more recognizable by outsiders, while others, who interpreted care as part of their usual family responsibilities, denied they were caregivers at all (Heenan, 2000; O’Connor, 2007; Robinson, 1999). Such dis-identification with the caregiver identity is problematic because it means that family caregivers are less likely to access support services and financial benefits (Montgomery & Kosloski, 2009).
In contrast, the third perspective which focuses on role learning to improve caregivers’ practice, makes caregiving a highly visible object of intervention and legitimacy, thus enabling family caregivers to access resources. This perspective also frames the informational and emotional support offered by health- and social-care professionals and peer caregivers as fundamental to developing role comfort and mastery during the encounter and metamorphosis phases of Jablin’s (2001) model. By increasing caregivers’ repertoire of strategies and fostering their sense of competence, programs and support initiatives also solidify their identity as caregivers. Interestingly, this perspective does not privilege role individualization, but instead creates a new collective “we” composed of other caregivers or even health and social service professionals.
Although this scoping review has allowed us to map out and categorize research findings across a body of multi-disciplinary literature (e.g., anthropology; gerontology; nursing; public health; social work), it has several limitations. First, in terms of our search strategy, we did not use Google Scholar, due to its tendency to include non-academic publications, which may have led us to miss relevant work. Moreover, within the databases we used, pertinent texts may have been overlooked because they did not contain the word socialization or its synonyms. Second, although scoping reviews allow researchers to describe and organize a vast evidence base, they do not seek to assess the robustness of research design or the quality of methods used (Arksey & O’Malley, 2005). Hence, we did not evaluate potential research bias in the studies we cited. Third, because scoping reviews aim to synthesize the literature, we focused on common patterns in socialization processes across multiple cultural contexts, rather than highlighting cultural differences.
The scoping review also points to several future research directions. First, it shows that research into the socialization process is somewhat uneven. Although we benefit from a considerable body of research on anticipatory socialization, fewer studies delve into how family caregivers manage the turning points within the metamorphosis phase of socialization (Carpentier et al., 2008) and how socialization and individualization processes are worked out in diverse cultural contexts with particular types of care regimes (funding, available alternatives, etc.). Familial, social, and political needs lead us to concentrate on how caregivers step up to the caregiving role. Future research could examine how some family members justify lower levels of or lack of engagement as well as the processes involved in disengagement, when caregivers pull back or reduce their caregiving responsibilities. Empirical studies with a longitudinal design would also facilitate analysis of the socialization process across time and over the life course (Evans et al., 2017), bearing in mind the type and amount of care provided (assistance with activities of daily living, dementia care) and care recipients’ needs.
The role of culture in family caregiver socialization also warrants further clarification. Most studies comparing “Korean,” “Cuban,” or “White” caregivers adopted functionalist or essentialist views of culture. Such views understand culture as the shared values, traditions, or practices common to members of a national or ethnic group, without interrogating the differences among members. Likewise, we also need to explore how socialization unfolds in non-Western and non-Confucian cultural contexts.
In conclusion, this review used socialization as a conceptual framework to analyze the literature on how family caregivers learn who should care and how to recognize, accept, and enact the role. The findings point toward three different perspectives of socialization that structure how caregiving is understood: socialization as role acculturation frames caregiving as predetermined role performance; socialization as role negotiation and identification positions caregiving as a career or unexpected event within the life course. Finally, socialization as specialized role learning frames caregiving as skills and knowledge that allow caregivers to provide care recipients with needed attention and resources. This framework highlights how socialization processes can make caregiving more or less visible and caregivers more or less likely to access support as they engage in the important work of family caregiving.
Supplemental Material
Supplemental Material, sj-docx-1-roa-10.1177_01640275211005092 - The Socialization of Unpaid Family Caregivers: A Scoping Review
Supplemental Material, sj-docx-1-roa-10.1177_01640275211005092 for The Socialization of Unpaid Family Caregivers: A Scoping Review by Kirstie McAllum, Mary Louisa Simpson, Christine Unson, Stephanie Fox and Kelley Kilpatrick in Research on Aging
Supplemental Material
Supplemental Material, sj-docx-2-roa-10.1177_01640275211005092 - The Socialization of Unpaid Family Caregivers: A Scoping Review
Supplemental Material, sj-docx-2-roa-10.1177_01640275211005092 for The Socialization of Unpaid Family Caregivers: A Scoping Review by Kirstie McAllum, Mary Louisa Simpson, Christine Unson, Stephanie Fox and Kelley Kilpatrick in Research on Aging
Footnotes
Acknowledgments
We would like to acknowledge Lise Higham’s assistance in running the database searches for the scoping review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.