
Abstract
As older adults increasingly live with multiple chronic conditions, appropriate medication use and adequate self-efficacy are important components of effective self-management. Self-neglect, characterized by insufficient attention to personal health and self-care, may be associated with health-related behaviors in later life. This study aimed to examine the association between self-neglect and self-efficacy for appropriate medication use among older adults. This descriptive cross-sectional correlational study was conducted in 2024 among older adults attending 11 comprehensive urban health centers in Rafsanjan, southeastern Iran. Participants were selected using proportional random sampling. Data were collected using a demographic questionnaire, the Elder Self-Neglect Scale, and the Self-Efficacy for Appropriate Medication Use Scale. Statistical analyses were performed using SPSS version 22. Participants demonstrated moderate levels of self-neglect (78.71 ± 12.28) and medication self-efficacy (23.80 ± 5.81). A weak inverse association was observed between self-neglect and self-efficacy for appropriate medication use (r = −.20, p = .05). Higher mean self-neglect scores were observed among women and participants with higher levels of education. The findings suggest a weak association between self-neglect and medication self-efficacy among older adults. Given the cross-sectional design and the borderline statistical significance of the association, causal inferences cannot be drawn. Further longitudinal and interventional studies are warranted to clarify the direction and practical significance of this relationship.
Introduction
Population aging represents a major demographic transformation of the current century, driven primarily by declining fertility rates and a global rise in life expectancy (Paul & Nag, 2024). According to the World Health Organization, the proportion of individuals aged 60 years and older is projected to nearly double by 2050, increasing from 12% to 22% of the total global population (World Health Organization, 2021). This demographic shift poses both challenges and opportunities for health and social care systems across all nations (Beard et al., 2016). Iran is no exception to this trend and is rapidly transitioning into an aging society, with estimates suggesting that by 2050, over 30% of the country’s population will consist of older adults (Koosha, 2025).
As the aging population grows, the quality of life and health of older adults have become key public health priorities (Sabatini et al., 2024) Aging is a sensitive life stage characterized by physiological, psychological, and social changes (Kaspar et al., 2024), predisposing older individuals to various health problems and vulnerabilities (Nicholson et al., 2024). One such issue is self-neglect, a complex and multifaceted public health concern (Day & McCarthy, 2016). Self-neglect refers to an individual’s failure to perform essential self-care activities, potentially leading to serious health consequences, including increased morbidity and mortality (X. Q. Dong, 2017). It may manifest as poor personal hygiene, inadequate living conditions, nutritional neglect, and non-adherence to therapeutic or medication regimens (Iris et al., 2010). The National Center on Elder Abuse defines self-neglect in older adults as “a behavior that threatens the health and safety of the senior” (X. Dong & Simon, 2013). This condition is characterized by social isolation, engagement in risky behaviors, diagnostic challenges, and an inability to meet basic needs. Its antecedents include physical, psychological, and socio-environmental factors, while its consequences affect individuals, caregivers, and society as a whole (Zhang & Zhang, 2025).
Older adults are major consumers of medications due to the high prevalence of chronic diseases and multimorbidity in this age group (Masnoon et al., 2017). Polypharmacy, commonly defined as the concurrent use of five or more medications, is highly prevalent among older adults (Fried et al., 2014). Excessive or inappropriate medication use, often resulting from physical or psychological challenges, is a significant concern and may lead to adverse drug effects, sometimes due to self-neglect or improper medication management (Fried et al., 2014; Hsu et al., 2021).
In this context, effective medication management requires not only access to treatment but also adequate cognitive, motivational, and self-regulatory capacities. Therefore, maintaining medication adherence and consistent therapeutic compliance is essential to prevent such complications.
Medication self-efficacy emerges as a critical psychological construct, referring to an individual’s confidence in their ability to manage their medication regimen effectively and safely (Risser et al., 2007; SaeedNia et al., 2022). Hamann et al. (2024) reported that low medication self-efficacy is associated with poor medication adherence, increased medication errors, and negative health outcomes (Hamann et al., 2024). Similarly, SaeedNia et al. (2022) demonstrated a significant association between self-efficacy and medication knowledge among patients with hypertension (SaeedNia et al., 2022). Lubis (2024) also found a significant positive relationship between self-efficacy and adherence to drug therapy indicating that individuals with higher self-efficacy exhibit greater adherence to prescribed treatments (Lubis, 2024).
From a theoretical perspective, Bandura’s self-efficacy theory provides a useful framework for understanding how self-neglect may be associated with medication self-efficacy.
Within this conceptual framework, self-neglect is assumed to reflect deficits in self-care behaviors that may influence medication-related self-efficacy. According to this theory, individuals’ beliefs in their capabilities influence their motivation, persistence, self-regulation, and engagement in health-related behaviors (Bandura, 1986). In older adults, self-neglect may undermine these mechanisms by reducing motivation for self-care, limiting mastery experiences related to medication management, and impairing self-regulatory behaviors. As a result, higher levels of self-neglect may be associated with lower confidence in managing medications appropriately.
Despite growing evidence on self-neglect and medication self-efficacy as separate constructs, the theoretical linkage between these constructs has received limited empirical attention, particularly within aging populations. Existing studies have primarily focused on the consequences of self-neglect or the determinants of medication adherence, with less emphasis on the psychological mechanisms, such as self-efficacy that may connect these phenomena.
In Iran, studies examining the relationship between self-neglect and medication self-efficacy among older adults have not yet been conducted. Clarifying this association is important for informing supportive and preventive strategies aimed at promoting safe medication use and enhancing self-care capacity in later life. Therefore, the present study aimed to investigate the relationship between self-neglect and self-efficacy for appropriate medication use among a sample of older adults in Iran.
Methods
This cross-sectional study was conducted in 2024 at comprehensive health centers and their satellite facilities in Rafsanjan, located in southeastern Iran. The statistical population consisted of all individuals aged 60 years or older with an active record in the 11 comprehensive health centers in Rafsanjan. According to the SIB system (the Iranian Health System Program) statistics, the number of older adults served by these health centers was 34,835 at the time of data collection. Using Cochran’s formula and a 95% confidence level, the sample size was calculated to be 265. To account for potential sample attrition, the final sample size was increased to 330 participants. A total of 30 elderly individuals were selected from each center using a simple random sampling method (through a lottery).
The inclusion criteria were: willingness to participate in the study; absence of Alzheimer’s disease; absence of mental disorders and debilitating physical illnesses that would prevent regular attendance at the center (based on self-declaration and confirmation by the health center nurse); use of one or more medications; non-use of psychotropic drugs; and a literacy level sufficient to comprehend the questionnaires. The exclusion criteria included: the participant’s refusal to continue cooperation at any stage of the research, and incomplete questionnaires with more than 20% missing responses.
Data were collected using the following three instruments:
Demographic and Background Information Questionnaire: This questionnaire, developed by the researcher, included items on age, gender, educational attainment, employment status, marital status, number of children, history of physical and mental illnesses, duration of illness, medication use status, and living situation. Information on the number of concurrently used medications was collected to describe medication burden, commonly referred to as polypharmacy.
Elder Self-Neglect Scale (ESNS): The ESNS was developed and validated in Iran by Motamed-Jahromi et al. (2023). The scale comprises 26 items distributed across six domains: physical environment (five items), physical health (six items), mental health (three items), financial status (three items), social network (three items), and self-determination (six items). The items are evaluated using a 5-point Likert scale, ranging from 1 (never) to 5 (always). The minimum score is 26, while the maximum score is 130. This study categorizes self-neglect as follows: a score below 60 denotes low self-neglect, a score ranging from 61 to 95 indicates moderate self-neglect, and a score of 96 or higher is classified as severe self-neglect. The reliability of this scale was assessed using Cronbach’s alpha, yielding a value of .85 for the entire scale and values ranging from .72 to .90 for the subscales (Motamed-Jahromi et al., 2023).
Self-efficacy Scale for Appropriate Medication Use (SEAMS): The scale was developed by Risser et al. (2007). It comprises 13 items that are administered as a self-report measure. The scoring system is based on a three-point Likert scale, where 1 indicates “not confident” and 3 indicates “very confident.” The minimum score is 13, while the maximum score is 39. Higher scores reflect greater self-efficacy regarding medication use. A score ranging from 13 to 21 indicates low self-efficacy, 22 to 30 signifies moderate self-efficacy, and 31 to 39 reflects desirable self-efficacy. The present study assessed the reliability of this scale using Cronbach’s alpha, which yielded a value of .89 (Risser et al., 2007). The scale’s validity and reliability were assessed in Iran by Sanchooli et al. (2018), who confirmed the questionnaire’s internal consistency as acceptable, with a minimum Cronbach’s alpha of .799 and a maximum of .807. The instrument’s reliability was evaluated through test-retest, yielding a coefficient of .97 as determined by Spearman’s correlation coefficient (Sanchooli et al., 2018).
Data collection was conducted after obtaining the necessary approvals. Potential participants were contacted by phone, during which the purpose of the study was explained and verbal informed consent was obtained. Participants who agreed to take part were then invited to the research setting. Upon arrival, written informed consent was obtained, and the questionnaires were completed using a structured interview format. To minimize interviewer bias, all interviews were conducted by a single trained researcher using standardized instructions. Participants were assured of the confidentiality and anonymity of their responses to encourage honest reporting. Completion of the questionnaire battery required approximately 20 to 30 min per participant. Data were entered into SPSS statistical software, version 22. Descriptive statistics, including mean, standard deviation, frequency, and percentage, were used to summarize participant characteristics and study variables. The Kolmogorov–Smirnov test was applied to assess the normality of data distribution. Inferential analyses included Pearson’s correlation coefficient and linear regression analysis. In the regression analysis, self-neglect was treated as the dependent variable based on the study’s conceptual framework, which considers self-neglect as an outcome reflecting deficits in self-care behaviors that may be associated with psychological factors such as medication self-efficacy. Given the cross-sectional design of the study, the regression analysis was conducted to explore associations rather than to infer causal relationships. The level of statistical significance was set at p < .05. Ethical approval for this study was obtained from the Ethics Committee of Rafsanjan University of Medical Sciences (Ethical approval code: IR.KMU.REC.1403.136; Reg. No. 403000176).
Results
All 330 older adults completed the study. The mean age of participants was 66.8 years (SD = 16.6; range: 60–90 years). Slightly more than half of the sample were women (51.8%). Most participants were married (83%), homemakers (41.2%), lived with their families (90%), and reported at least one chronic disease (75.2%). Educational attainment was generally low to moderate, with 38.5% having completed primary or middle school education (Table 1).
Demographic Characteristics of Older Adults Referring to Comprehensive Health Centers.

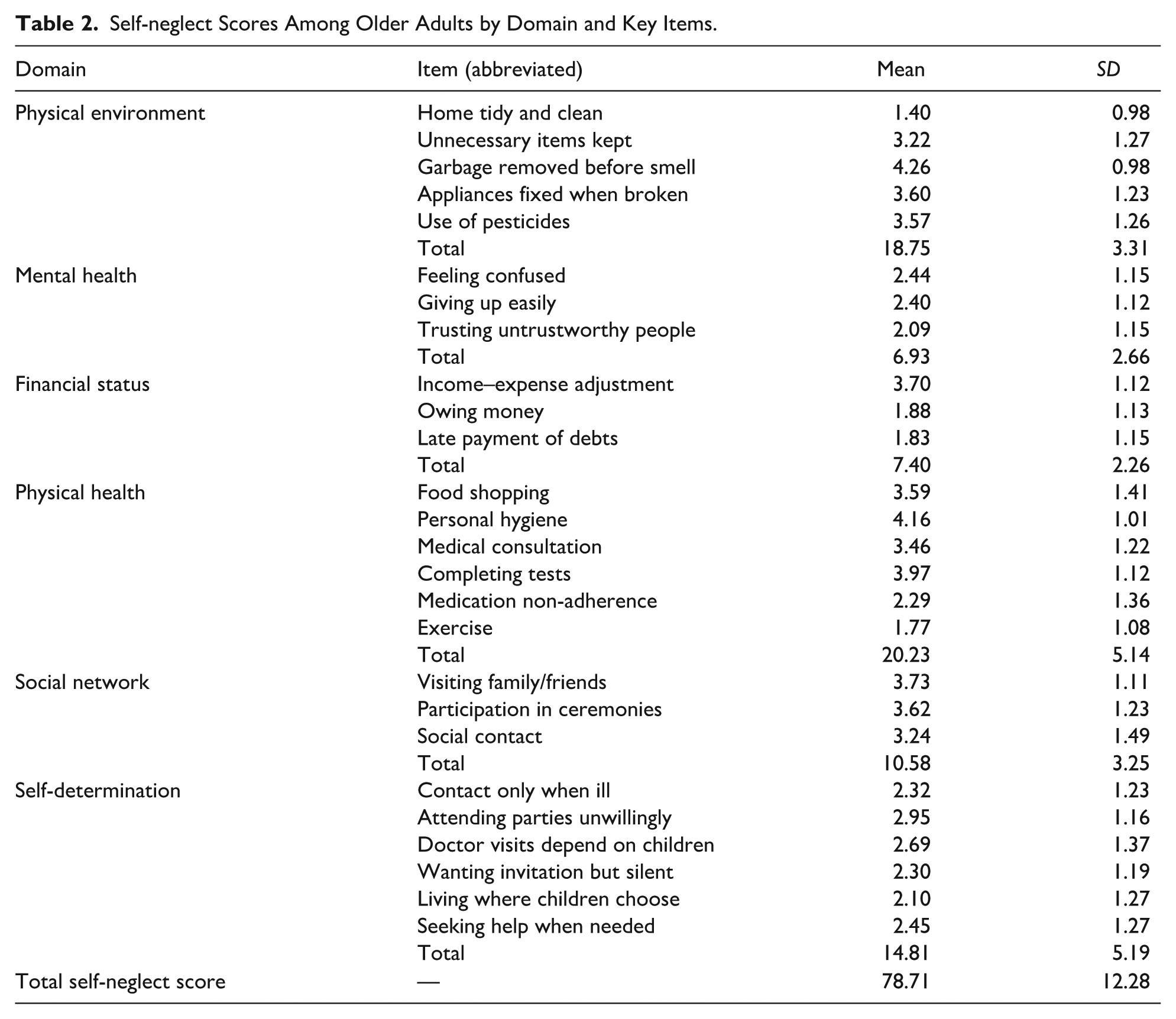
The mean total self-neglect score was 78.71 ± 12.28, reflecting a moderate level of self-neglect. At the domain level, physical living conditions showed the highest mean score. Item-level analysis indicated that “I put the garbage outside before it starts to smell” had the highest mean score within this domain, whereas “My home is tidy and clean” had the lowest. To enhance readability, domain-level and total self-neglect scores are emphasized in Table 2, while item descriptions are presented in abbreviated form.
Self-neglect Scores Among Older Adults by Domain and Key Items.
The mean medication self-efficacy score was 23.80 ± 5.81, indicating a moderate level of confidence in medication use. Among the SEAMS items, the highest mean score was observed for “When the drugs cause some side effects,” while the lowest was related to uncertainty when medications appeared different from usual. Accordingly, Table 3 emphasizes the total medication self-efficacy score, with item-level results presented in a condensed format.
Medication Self-Efficacy (SEAMS) Item Scores Among Older Adults.

Correlation analysis revealed a weak inverse association between overall self-neglect and medication self-efficacy (r = −.20, p = .05). Despite reaching statistical significance, the magnitude of this correlation was small, indicating limited practical strength. Similarly, weak but statistically significant inverse correlations were observed between medication self-efficacy and the mental health (r = −.13), financial issues (r = −.11), and self-determination (r = −.14) domains. No significant associations were found between medication self-efficacy and the physical environment, physical health, or social network domains (Table 4). Overall, these findings reflect modest associations rather than strong relationships.
Correlations Between Self-Neglect Domains and Medication Self-Efficacy.
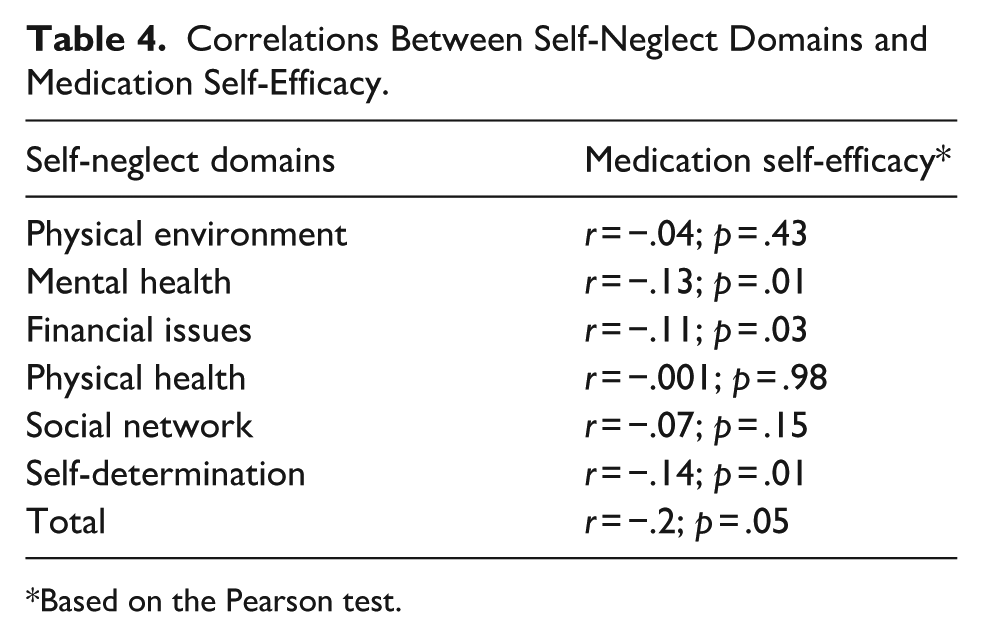
Based on the Pearson test.
Stepwise multiple regression analysis was conducted to examine variables statistically associated with self-neglect scores. Self-neglect was entered as the dependent variable, while medication self-efficacy and demographic characteristics were included as independent variables. The results showed that gender, educational attainment, and medication self-efficacy were significantly associated with self-neglect scores. Medication self-efficacy demonstrated a small inverse association with self-neglect (β = −.11, p = .05), suggesting co-occurrence rather than a causal relationship. Women had higher mean self-neglect scores than men, and higher educational attainment was also associated with higher self-neglect scores (Table 5).
Regression Coefficients for the Effect of Medication Self-Efficacy and Background Variables on Self-Neglect Among Older Adults Visiting Comprehensive Health Centers in Rafsanjan.

Discussion
This study aimed to investigate the relationship between self-neglect and self-efficacy for appropriate medication in older adults attending comprehensive health centers. Findings indicated that both self-neglect and medication self-efficacy levels among the participants were moderate. While a moderate level of self-neglect may be manageable within healthcare settings, any interpretation regarding management or improvement should be made cautiously and cannot be inferred directly from the present data. Importantly, the relationship between these two variables was identified as a statistically significant but weak inverse association, underscoring the need for restrained interpretation.
The current study’s findings regarding moderate levels of self-neglect among older adults are consistent with previous research. Ayaz and Gürsoy (2024), for example, reported a prevalence of self-neglect of 36.6% and identified several socio-demographic and health-related correlates, including living alone, poor self-perceived health, cognitive impairment, dependency, and low educational attainment (Ayaz & Gürsoy, 2024). These similarities suggest that self-neglect is a relatively common phenomenon among older adults across different cultural contexts, although prevalence estimates and associated factors may vary depending on population characteristics and measurement approaches. Another study conducted have likewise highlighted the importance of addressing self-neglect among older adults (Wang et al., 2023).
The findings also indicated that medication self-efficacy among older adults was at a moderate level, suggesting that participants perceived a moderate degree of confidence in managing their medications. Rather than indicating inadequacy, this finding points to potential variability in confidence levels and highlights an area that may benefit from supportive strategies. Previous studies have reported higher levels of medication self-efficacy in specific patient groups, such as individuals with hypertension (Ayaz & Gürsoy, 2024; X. Dong et al., 2013), which may reflect differences in disease-related education, healthcare engagement, or sample characteristics. The comparatively lower scores observed in the present study may therefore be context-dependent rather than indicative of poorer capability. At the item level, the lowest medication self-efficacy score was related to changes in the appearance of medications. This finding may reflect uncertainty or confusion rather than a lack of overall competence and highlights a specific aspect of medication management that could be addressed through clearer communication by healthcare providers. Possible explanations include limited familiarity with generic substitutions, concerns about medication errors, or insufficient counseling at the point of dispensing.
A key finding of this study was the weak inverse association between self-neglect and medication self-efficacy. Although this association was statistically significant, its small magnitude suggests limited practical strength and does not support conclusions about directionality or causality. While self-efficacy theory (Bandura, 1986) provides a useful conceptual framework for understanding how confidence may relate to health behaviors, the present findings should be interpreted as indicating co-occurrence rather than a directional influence. Older adults with lower medication self-efficacy tended to report higher levels of self-neglect, but it is equally plausible that self-neglect coexists with or reflects broader functional, psychological, or social challenges. Similarly, self-neglect may be associated with factors such as depression, social isolation, or cognitive decline, which could also influence medication self-efficacy (X. Dong et al., 2013).
The observed associations between medication self-efficacy and specific self-neglect domains: namely mental health, financial issues; and self-determination were also weak but statistically significant. These findings suggest that psychological well-being, financial stability, and perceived autonomy may be related to confidence in medication management, although the strength of these relationships was modest. Previous research has similarly reported links between depression, financial stress, and reduced self-efficacy among older adults (Kim, 2021; Yoon et al., 2020), supporting the plausibility of these associations.
Another notable finding was the association between self-neglect, gender, and educational attainment. Consistent with prior research, women in the present study exhibited higher self-neglect scores than men. Studies conducted in other cultural contexts have suggested that older women may be more vulnerable to self-neglect due to social roles, economic dependency, or caregiving burdens (Jeong et al., 2022). However, these explanations remain speculative in the absence of qualitative or longitudinal data. The association between higher educational attainment and greater self-neglect was counterintuitive and warrants careful interpretation. Rather than implying that education increases the risk of self-neglect, this finding may reflect complex social or psychological mechanisms. For example, older adults with higher education may have higher expectations regarding independence, autonomy, or quality of life, making them more likely to perceive or report self-neglect-related behaviors. Alternatively, educational attainment may interact with other unmeasured factors such as social isolation, changing family dynamics, or unmet expectations during aging. Given cultural and contextual differences, this finding should be interpreted cautiously, particularly for an international audience, and requires further investigation.
Limitations
Several limitations of the present study should be acknowledged. First, the study relied on self-reported questionnaires, which may be subject to recall bias and social desirability bias. Participants may have underreported or overreported certain behaviors, particularly those related to self-neglect. Second, the cross-sectional design of the study precludes any inference regarding temporal or causal relationships between self-neglect and medication self-efficacy. Third, although some associations reached statistical significance, the observed effect sizes were generally weak, suggesting limited practical significance of the findings. Finally, the study had limited control over several potentially important confounding variables, including polypharmacy, cognitive status, mental health conditions (such as depressive symptoms), severity of chronic illnesses, social support, and access to healthcare services. These factors may have influenced both self-neglect and medication self-efficacy and should be considered in future longitudinal and interventional research
Conclusion
This study found that self-neglect and medication self-efficacy among older adults were at moderate levels, with a weak and inverse association observed between the two variables. Given the cross-sectional design, this relationship cannot be interpreted as causal or directional and should be considered as indicating potential co-occurrence rather than one factor influencing the other. The findings suggest that older adults who report higher self-neglect may also experience lower confidence in managing medications, but this association is modest and likely influenced by other psychological, social, or functional factors. Identification of older adults who may face challenges with medication management, along with attention to psychological well-being, financial concerns, and personal autonomy, could be useful for healthcare planning. However, the effectiveness of specific educational or intervention programs cannot be determined from the present study. Future longitudinal and mixed-methods research is recommended to explore the factors affecting medication self-efficacy more deeply, clarify temporal relationships, and provide stronger evidence to inform the development of targeted and context-sensitive interventions for older adults.
Footnotes
Acknowledgements
We sincerely appreciate the support provided by the Vice-Chancellor for Research at Kerman University of Medical Sciences. We also extend our deepest gratitude to the dedicated officials and staff of the comprehensive health centers in Rafsanjan for their valuable collaboration throughout the study. Most importantly, we are profoundly grateful to the elderly participants whose willingness, time, and cooperation made this research possible. Their trust and contributions are truly appreciated, and without them, this study could not have been accomplished.
Ethical Considerations
The study was approved by the Ethics Committee of Kerman University of Medical Sciences (IR.KMU.REC.1403.136, Reg. No. 403000176). The research was conducted in accordance with the principles of the Declaration of Helsinki and the guidelines of the Committee on Publication Ethics (COPE).
Consent to Participate
All participants provided written informed consent before taking part in the study. They were fully informed about the study objectives, procedures, methods of data collection and recording, the roles of both the researchers and participants, and their right to voluntary participation and confidentiality.
Author Contributions
HA, JF, MMJ, and SKS contributed to conceiving and designing the research. Data was collected by DB. Data analysis and interpretation were made by JF, SKS, and HA, who also participated in data interpretation. MMJ conducted the intervention.SKS, JF, and HA participated in drafting the manuscript. HA, JF, MMJ, and SKS revised the manuscript critically for important intellectual content and final approval of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.